You might also like
- Entertainment Performance ContractDocument4 pagesEntertainment Performance ContractSammy Gaines Jr.100% (3)
- Global Edge Software Limited: Payslip For The Month of December - 2018Document1 pageGlobal Edge Software Limited: Payslip For The Month of December - 2018Manoj SahooNo ratings yet
- Advertising and SalesmanshipDocument18 pagesAdvertising and Salesmanshipsailesh3167% (3)
- Hospitality SecurityDocument315 pagesHospitality SecuritySummer Calf100% (3)
- BianDocument1 pageBianArie Wibowo SutiarsoNo ratings yet
- SIMS ReportDocument2 pagesSIMS Reportr_i_k_yNo ratings yet
- Contracts Case Brief ChartDocument40 pagesContracts Case Brief Chartnlandsmanuchicagoedu100% (1)
- TSR 007-Trk-Pmj-Terex 60-TR112 - T 8821378-Replace Ecm-Slamet Wahyu WDocument4 pagesTSR 007-Trk-Pmj-Terex 60-TR112 - T 8821378-Replace Ecm-Slamet Wahyu WFrigia IsudibyoNo ratings yet
- Case Study School Heads Performance in Terms With The 5 KraDocument11 pagesCase Study School Heads Performance in Terms With The 5 KraRM Ferrancol100% (2)
- Indian OIL TenderDocument40 pagesIndian OIL TenderthengaNo ratings yet
- General Conditions of Contract Qatar May 2007Document58 pagesGeneral Conditions of Contract Qatar May 2007Leonidas AnaxandridaNo ratings yet
- Vio55-6a Parts ManualDocument303 pagesVio55-6a Parts ManualJason Serwa100% (1)
- Layered Process Audits: How To Improve Quality From The Ground UpDocument22 pagesLayered Process Audits: How To Improve Quality From The Ground UpMoraru Ciprian100% (1)
- Saudi Aramco Test Report: In-Process Inspection of Field Coating SATR-H-2006 27-Jan-19 CoatDocument3 pagesSaudi Aramco Test Report: In-Process Inspection of Field Coating SATR-H-2006 27-Jan-19 CoatMoghal AliNo ratings yet
- Cobbledick Layered Process Audits PDFDocument22 pagesCobbledick Layered Process Audits PDFelyesNo ratings yet
- Peñaranda Vs BagangaDocument1 pagePeñaranda Vs BagangachugamiNo ratings yet
- Coal Boiler OptimizationDocument45 pagesCoal Boiler OptimizationSuriyan ArifNo ratings yet
- Design and Construction Agreement - TemplateDocument6 pagesDesign and Construction Agreement - Templatelengjavier100% (2)
- CoCu 1 Foot ReflexologyDocument20 pagesCoCu 1 Foot ReflexologySITI NAJIBAH BINTI MOHD NORNo ratings yet
- Denah Instalasi PDFDocument1 pageDenah Instalasi PDFMuhammad RafiqNo ratings yet
- 09.2 Gyro Compass Annual MaintenanceDocument1 page09.2 Gyro Compass Annual MaintenanceTC Atilla KarakaşNo ratings yet
- B5 A06 5F Option 02Document1 pageB5 A06 5F Option 02Malik RiazNo ratings yet
- A B C A B C: Third Floor Plan Roof Deck PlanDocument1 pageA B C A B C: Third Floor Plan Roof Deck PlanJeanelyn DioNo ratings yet
- Wednesday, March 11, 2009Document2 pagesWednesday, March 11, 2009steve413100% (2)
- KW 24.25junioDocument1 pageKW 24.25junioJavi MorNo ratings yet
- Aarambh New BrochureDocument21 pagesAarambh New BrochureSarika MayekarNo ratings yet
- Assigned by Work Control: Equipment Tag No. Building Name Room No. Hot Water New Steam ReplacementDocument2 pagesAssigned by Work Control: Equipment Tag No. Building Name Room No. Hot Water New Steam ReplacementArnoldNo ratings yet
- Plan at El (+) 16.200/el (+) 15.500M LevelDocument1 pagePlan at El (+) 16.200/el (+) 15.500M Levelsubramanian SivaNo ratings yet
- GTT, CAAT 1, PATVEP, TEI REVISED PLANS-ModelDocument1 pageGTT, CAAT 1, PATVEP, TEI REVISED PLANS-ModelMARK BENEDICT FEDERIONo ratings yet
- Sign. & Barication PlanDocument1 pageSign. & Barication PlanMuhammad AtifNo ratings yet
- Saudi Aramco Test Report: SATR-H-2011 27-Jan-19 Mech Surface Preparation of Internal Pipe End/Joints For FBE CoatingDocument2 pagesSaudi Aramco Test Report: SATR-H-2011 27-Jan-19 Mech Surface Preparation of Internal Pipe End/Joints For FBE CoatingMoghal AliNo ratings yet
- 7villa-Om-Me-01 Ducted Split Ac UnitsDocument52 pages7villa-Om-Me-01 Ducted Split Ac UnitsAravindhan ANo ratings yet
- Organization Chart For RamadanDocument1 pageOrganization Chart For RamadanSehna SerajNo ratings yet
- Pre-Stowage Plan-Maputo 01 23 02 2022Document1 pagePre-Stowage Plan-Maputo 01 23 02 2022Zb ZbNo ratings yet
- DPR Dated 05-12-2023Document103 pagesDPR Dated 05-12-2023Rakshith MarichennaiahNo ratings yet
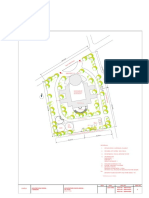
- Final Architectural CollegeDocument1 pageFinal Architectural Collegethrigya myakalaNo ratings yet
- Service Report: Final Action Code Description OutcomeDocument1 pageService Report: Final Action Code Description OutcomeJoel CieltoNo ratings yet
- 9TH FloorDocument1 page9TH Floorkapil chughNo ratings yet
- Cobbledick Layered Process Audits PDFDocument22 pagesCobbledick Layered Process Audits PDFelyesNo ratings yet
- 7villa-Om-Me-02 DX Hi Wall Split Ac UnitsDocument60 pages7villa-Om-Me-02 DX Hi Wall Split Ac UnitsAravindhan ANo ratings yet
- KMIADocument31 pagesKMIAjackpilot32No ratings yet
- KW 22.23 - JunioDocument1 pageKW 22.23 - JunioJavi MorNo ratings yet
- WMKADocument12 pagesWMKAAbdullah Zubair100% (1)
- Djibouti - HDAMDocument18 pagesDjibouti - HDAMsadjuharNo ratings yet
- RIR & SIR - 6 Monthly Safety Inspection - TCMSDocument4 pagesRIR & SIR - 6 Monthly Safety Inspection - TCMSRonny DoankNo ratings yet
- Schedule of Doors and WindowsDocument1 pageSchedule of Doors and WindowsKevin RamosNo ratings yet
- G-Series Servo Drive: @, R88D-GT@Document14 pagesG-Series Servo Drive: @, R88D-GT@HOFFMAN STEINHOWERNo ratings yet
- Satr-W-2010Document1 pageSatr-W-2010Joni Carino SuniNo ratings yet
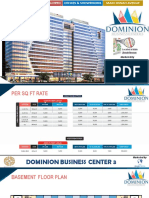
- Dominion Business Center 3 FinalDocument6 pagesDominion Business Center 3 FinalBlue Earth PropertiesNo ratings yet
- Bharat Broadband Network Limited: As Built Drawing (Abd) For Increment Ofcable Route For Nofn ProjectDocument36 pagesBharat Broadband Network Limited: As Built Drawing (Abd) For Increment Ofcable Route For Nofn ProjectAlexander MccormickNo ratings yet
- Orca Share Media1639477405853 6876466641284393633Document1 pageOrca Share Media1639477405853 6876466641284393633Sweet HusainNo ratings yet
- %/.) (-Ma Am.L.0 - K: MS.M/.), R/T) HMSRMC MmbgnoDocument63 pages%/.) (-Ma Am.L.0 - K: MS.M/.), R/T) HMSRMC Mmbgnoابو الكلام غلامNo ratings yet
- Daily Report 14 Feb 23Document2 pagesDaily Report 14 Feb 23Galang PratamaNo ratings yet
- F4 PDFDocument1 pageF4 PDFMarvin ObilloNo ratings yet
- SBCN - Rnav Utnor 1a 1b - Utkal 1a 1b Rwy 09 27 - Sid - 20201105Document1 pageSBCN - Rnav Utnor 1a 1b - Utkal 1a 1b Rwy 09 27 - Sid - 20201105Lucas CastroNo ratings yet
- Lay Out Workshop TeritibDocument1 pageLay Out Workshop TeritiblilikNo ratings yet
- GCPD-Verification Certification-Master List - MAY 31Document34 pagesGCPD-Verification Certification-Master List - MAY 31Sheri DiĺlNo ratings yet
- Denah Bu Yan Ti PuspogiwangDocument1 pageDenah Bu Yan Ti PuspogiwangirfanmisbakhulNo ratings yet
- Captura de Pantalla 2023-07-03 A La(s) 12.21.27Document1 pageCaptura de Pantalla 2023-07-03 A La(s) 12.21.27pochillommNo ratings yet
- Gi Meshwire 10 AWGDocument1 pageGi Meshwire 10 AWGNAQIB METKARNo ratings yet
- Stolen Vehicle Tracking & Recovery Systems in MalaysiaDocument6 pagesStolen Vehicle Tracking & Recovery Systems in MalaysiaTan_Wei_Chan_3670No ratings yet
- DR CD 101 00 DR CD 101 00Document1 pageDR CD 101 00 DR CD 101 00AslamNo ratings yet
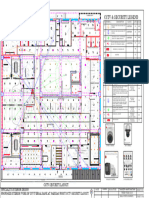
- CCTV SecurityDocument1 pageCCTV SecurityvedangnuNo ratings yet
- As Model PDFDocument1 pageAs Model PDFKimberlyNo ratings yet
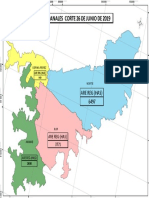
- Area Re Por Canales 2Document1 pageArea Re Por Canales 2leonardo vargasNo ratings yet
- Third FloorplanDocument1 pageThird Floorplanvillarealjayson362No ratings yet
- 100M Running TrackDocument1 page100M Running TrackMohammed Uzeman ChhipaNo ratings yet
- Denah Penanaman Semak Lantai 1: A B CD E F G H I J K L M N O PDocument1 pageDenah Penanaman Semak Lantai 1: A B CD E F G H I J K L M N O PDeni WahyudiNo ratings yet
- D038 Evs Co000 1092 - 00Document1 pageD038 Evs Co000 1092 - 00Mussarat BabasahebNo ratings yet
- 3 Level Split Type Floor PlanDocument1 page3 Level Split Type Floor PlanJohn Marines EstiocoNo ratings yet
- Inspection Request (Ir) : Project Name: 2.private Villa (G+1+P) MR. Jaralla AL Samikh Al RayyanDocument4 pagesInspection Request (Ir) : Project Name: 2.private Villa (G+1+P) MR. Jaralla AL Samikh Al RayyanMohammed JavidNo ratings yet
- Fixed Assets Listing As at 310123Document8 pagesFixed Assets Listing As at 310123SITI NAJIBAH BINTI MOHD NORNo ratings yet
- 202008270436Document2 pages202008270436SITI NAJIBAH BINTI MOHD NORNo ratings yet
- AEON - AR2021 (Part 4)Document66 pagesAEON - AR2021 (Part 4)SITI NAJIBAH BINTI MOHD NORNo ratings yet
- HR Interview Questions Based On IndustrialDocument7 pagesHR Interview Questions Based On IndustrialRANG28120% (1)
- Resume Cover Letter For Receptionist PositionDocument7 pagesResume Cover Letter For Receptionist Positionafmrgjwjcowaov100% (1)
- Spec Contract Appointment Letter.Document5 pagesSpec Contract Appointment Letter.zeeshan100% (1)
- Organization Behaviour-Chap6Document13 pagesOrganization Behaviour-Chap6Thảo Lê Ngọc PhươngNo ratings yet
- Payslip YemplateDocument2 pagesPayslip YemplateCristine GonzalesNo ratings yet
- Classification of Individual TaxpayerDocument4 pagesClassification of Individual TaxpayerJj helterbrandNo ratings yet
- Scope of Work (SOW) & Special Conditions of Contract (SCC) : Section-IDocument10 pagesScope of Work (SOW) & Special Conditions of Contract (SCC) : Section-IRavinder MittalNo ratings yet
- Introduction To Human Resource ManagementDocument17 pagesIntroduction To Human Resource Managementolivia hoNo ratings yet
- Vidhyanand NayakDocument3 pagesVidhyanand Nayakdeepak tamboliNo ratings yet
- Essay 10Document3 pagesEssay 10Dung Đỗ Lê NghiNo ratings yet
- HR ProjectDocument4 pagesHR Projectsweety2403No ratings yet
- Department of Labor: Agency Responsible Overpayment by Cause All StatesDocument40 pagesDepartment of Labor: Agency Responsible Overpayment by Cause All StatesUSA_DepartmentOfLaborNo ratings yet
- VGSM Manufacturing Strategy - Jan 2011Document405 pagesVGSM Manufacturing Strategy - Jan 2011Ignacio Gutierrez NarvaezNo ratings yet
- Current Affairs August 2015 PDF V1 by AffairsCloudDocument222 pagesCurrent Affairs August 2015 PDF V1 by AffairsCloudvoldemort1989No ratings yet
- Litton v. HillDocument2 pagesLitton v. HillMike Zaccahry MilcaNo ratings yet
- SHRM Chapter 01Document26 pagesSHRM Chapter 01papripetals07No ratings yet
- Merritt Morning Market 3052 - Sept 11Document2 pagesMerritt Morning Market 3052 - Sept 11Kim LeclairNo ratings yet
- Chapter FourDocument14 pagesChapter FourMuzamel AbdellaNo ratings yet
- Notes On Separation PayDocument2 pagesNotes On Separation PayTheodore DolarNo ratings yet