You might also like
- Brief History of ClassDocument2 pagesBrief History of ClassamlanbabaiNo ratings yet
- Vicinity Map: Ralph Luis D. Cardano Adamson University Ian Ray L. DecenaDocument1 pageVicinity Map: Ralph Luis D. Cardano Adamson University Ian Ray L. DecenaGecilo TabogonNo ratings yet
- Sheet UTS BenjutDocument2 pagesSheet UTS BenjutJasonSamuelNo ratings yet
- GSM Mobile Role in Originating Call ContextDocument2 pagesGSM Mobile Role in Originating Call ContextLeuLeuNo ratings yet
- Everything You Need to Know About Understanding IP Addressing and Solving Internet Scaling IssuesDocument21 pagesEverything You Need to Know About Understanding IP Addressing and Solving Internet Scaling IssuesAdnan SohailNo ratings yet
- Expolre Readiing A1 Progress 2Document1 pageExpolre Readiing A1 Progress 2Christian David Rodriguez GNo ratings yet
- BMS34A00182Document2 pagesBMS34A00182Rohit Parmar (Computer Operator, Bangalore)No ratings yet
- Mabilo-Model pdf7Document1 pageMabilo-Model pdf7Jennylou DingalNo ratings yet
- GSM Originating Call Overview ContextDocument2 pagesGSM Originating Call Overview ContextLeuLeuNo ratings yet
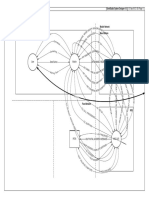
- Number Date Modification E OwnerDocument1 pageNumber Date Modification E Owneroscar aguilarNo ratings yet
- Urutonde RW Abahamwe N Icyaha Cya Ruswa Gicurasi-Kamena 2020Document10 pagesUrutonde RW Abahamwe N Icyaha Cya Ruswa Gicurasi-Kamena 2020Josephine MukamahoroNo ratings yet
- Mazda CX 5 2011 en Connection Points 1 Can Bus Ds500Document1 pageMazda CX 5 2011 en Connection Points 1 Can Bus Ds500Florin Sorin Bila NicolaNo ratings yet
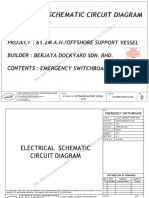
- BJ 55 Esb - AbsDocument61 pagesBJ 55 Esb - AbsHatem GhabiNo ratings yet
- Alfonso Alvarado CV PDFDocument32 pagesAlfonso Alvarado CV PDFFonsAlvaradoNo ratings yet
- 1 - GSM Inter MSC Handover Call FlowDocument1 page1 - GSM Inter MSC Handover Call FlowMek WoluNo ratings yet
- Bentuk Surat PenyediaDocument1 pageBentuk Surat PenyediaAkbar Iman SNo ratings yet
- White Entrance: London New Year'S Eve FireworksDocument4 pagesWhite Entrance: London New Year'S Eve FireworksCorrosion EngNo ratings yet
- Fast Set Green Adhesive: General DescriptionDocument1 pageFast Set Green Adhesive: General DescriptionBaugh Graphic DesignNo ratings yet
- Tuscany S 01Document1 pageTuscany S 01francis sebastian lagamayoNo ratings yet
- Ild 22Document1 pageIld 22Felipe GarciaNo ratings yet
- Packing PlanDocument2 pagesPacking Planmungkin bisaNo ratings yet
- Ellingham DiagramDocument1 pageEllingham Diagrammathan baNo ratings yet
- Multi ProsDocument13 pagesMulti ProsRohit BaraskarNo ratings yet
- Dhan 29Document2 pagesDhan 29Kshitij NagraleNo ratings yet
- MDPC Airport InfoDocument28 pagesMDPC Airport InfoLiviu 22100% (1)
- Leci PDFDocument5 pagesLeci PDFMiguel Angel MartinNo ratings yet
- Req - Ladrillo King KongDocument1 pageReq - Ladrillo King KongJhon OrtegaNo ratings yet
- Location Map: Stevenage, UKDocument2 pagesLocation Map: Stevenage, UKTanzyy.2018No ratings yet
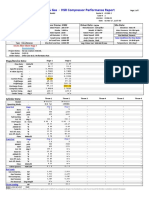
- Gas-HS Compressor Performance Report SummaryDocument6 pagesGas-HS Compressor Performance Report SummaryparathasiNo ratings yet
- BrgyBantayanon Calatrava NegrosOccidental DDDDocument31 pagesBrgyBantayanon Calatrava NegrosOccidental DDDNoel PagalingNo ratings yet
- Packing PlanDocument2 pagesPacking Planmungkin bisaNo ratings yet
- Gucci FactureDocument1 pageGucci FactureflorianduplouyNo ratings yet
- Station Limits (Line 2) : Matchline Sta. 0+400Document1 pageStation Limits (Line 2) : Matchline Sta. 0+400Temoteo L Pupa IIINo ratings yet
- Site infrastructure as-built planDocument1 pageSite infrastructure as-built planJing JingNo ratings yet
- Vira Long BaseDocument1 pageVira Long Basemohammad khoraminiaNo ratings yet
- Vas 3Document1 pageVas 3api-240936355No ratings yet
- VasnewDocument1 pageVasnewapi-240936355No ratings yet
- Map5 SouthPole ASMA v10Document1 pageMap5 SouthPole ASMA v10Ricardo Salinas FournierNo ratings yet
- RAKC COOLROOM WAREHOUSEDocument3 pagesRAKC COOLROOM WAREHOUSEfebriNo ratings yet
- Adobe Scan 29 Nov 2022Document1 pageAdobe Scan 29 Nov 2022Devendra TyagiNo ratings yet
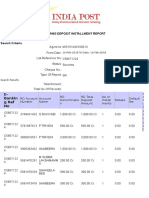
- Recurring Deposit Installment Report: E-Bankin G Ref NoDocument4 pagesRecurring Deposit Installment Report: E-Bankin G Ref NoShahazad ShaikNo ratings yet
- 1868 en EDocument16 pages1868 en EMohamed100% (1)
- City Council Districts For The City of Los Angeles, CaliforniaDocument1 pageCity Council Districts For The City of Los Angeles, Californiapolitix100% (1)
- Data CenterDocument21 pagesData CenterMan TheNo ratings yet
- Wtve-Llc: Huntington Park, CA 90255 2315 Nadeau Street Direct Billing 800.586.9701Document4 pagesWtve-Llc: Huntington Park, CA 90255 2315 Nadeau Street Direct Billing 800.586.9701Rohit BaraskarNo ratings yet
- Railway Track and Signalling: Defined Interstate NetworkDocument25 pagesRailway Track and Signalling: Defined Interstate NetworkibrgazdharNo ratings yet
- Placement of The Screw Press Skid: As-BuiltDocument1 pagePlacement of The Screw Press Skid: As-BuiltjdmamsresurreccionNo ratings yet
- 905J ROD Assy ST/STL 905J BODY Assy ST/STL Steelwork (Not by Pa) 30Document1 page905J ROD Assy ST/STL 905J BODY Assy ST/STL Steelwork (Not by Pa) 30SACHIDANANDA SNo ratings yet
- BCTS Rose Swanson Mountain Recommended Harvest MapDocument1 pageBCTS Rose Swanson Mountain Recommended Harvest MapMeganNo ratings yet
- FLSmidth Packing List for Quellaveco ProjectDocument45 pagesFLSmidth Packing List for Quellaveco ProjectChris VilaNo ratings yet
- Ward 23 Mogalakwena Local MunicipalityDocument1 pageWard 23 Mogalakwena Local MunicipalityFrans KutumelaNo ratings yet
- Mw629e-026-21 Electrical Power System Studies Short-Circuit Analysis - 78536523Document18 pagesMw629e-026-21 Electrical Power System Studies Short-Circuit Analysis - 78536523kundankundan singhNo ratings yet
- Acer Swift 3 Setup GuideDocument8 pagesAcer Swift 3 Setup GuideHuaseongNo ratings yet
- Estimate of Slab Culvert in ExcelDocument6 pagesEstimate of Slab Culvert in ExcelVivek ShuklaNo ratings yet
- FileDownLoad, 19217, en PDFDocument57 pagesFileDownLoad, 19217, en PDFontaarabNo ratings yet
- Lero PDFDocument5 pagesLero PDFMiguel Angel MartinNo ratings yet
- SBPP Omni-Rwy-04-22 Sid 20211202Document1 pageSBPP Omni-Rwy-04-22 Sid 20211202Furuss del reignoNo ratings yet
- BH Pier-04Document1 pageBH Pier-04Shamsul IslamNo ratings yet
- Role of Actuaries in InsuranceDocument46 pagesRole of Actuaries in InsurancePranav ViraNo ratings yet
- A Lady / A Elite Lady: ProtectionDocument37 pagesA Lady / A Elite Lady: ProtectionRaheel ShaikhNo ratings yet
- CFPB Small Entity Compliance Guide, 2014Document56 pagesCFPB Small Entity Compliance Guide, 2014ed_nycNo ratings yet
- Bilingual List-December-2023Document2 pagesBilingual List-December-2023kailasiyerNo ratings yet
- 01 Market Organization and Structure PDFDocument23 pages01 Market Organization and Structure PDFNgân Hà Nguyễn0% (1)
- BFS L0 Ques464Document360 pagesBFS L0 Ques464Aayush AgrawalNo ratings yet
- Job Analysis ProjectDocument29 pagesJob Analysis Projectapi-663278461No ratings yet
- Banking Financial Services Management Lesson PlanDocument3 pagesBanking Financial Services Management Lesson PlanRamalingam Chandrasekharan0% (1)
- Loan PolicyDocument5 pagesLoan PolicyAyesha FarooqNo ratings yet
- Terrorism Insurance Terms & ConditionsDocument10 pagesTerrorism Insurance Terms & ConditionsKároly DezsőNo ratings yet
- Peter Van Kerckhoven - 4 PDFDocument16 pagesPeter Van Kerckhoven - 4 PDFEmil AzhibayevNo ratings yet
- VN Salary Guide 2023Document80 pagesVN Salary Guide 2023Nguyen Quang HuyNo ratings yet
- OT Fu Acc II ch5Document18 pagesOT Fu Acc II ch5newaybeyene5No ratings yet
- DepEd School Building Asset Details ReportDocument46 pagesDepEd School Building Asset Details ReportJohn Eric Peregrino100% (1)
- Data Analysis and InterpretationDocument12 pagesData Analysis and Interpretationsaimhatre1122004No ratings yet
- Insurance Principles and PracticesDocument16 pagesInsurance Principles and Practicesshakhawat hossainNo ratings yet
- Investment Banking Preparation Week 1Document12 pagesInvestment Banking Preparation Week 1daniel18ctNo ratings yet
- Sea Pearl Prospectus PDFDocument245 pagesSea Pearl Prospectus PDFImtiaz ChowdhuryNo ratings yet
- Luzern Associates LLC Investment Opportunity PresentationDocument19 pagesLuzern Associates LLC Investment Opportunity PresentationAli Gokhan KocanNo ratings yet
- IC 38 Question Bank MCQs PDFDocument42 pagesIC 38 Question Bank MCQs PDFnirmal100% (2)
- 2014 US Loan PrimerDocument27 pages2014 US Loan Primerxen101No ratings yet
- Business Environment Case StudyDocument6 pagesBusiness Environment Case StudyBharathi KamathNo ratings yet
- Sr. X underwriting commission questions and answersDocument7 pagesSr. X underwriting commission questions and answersSneha GopalNo ratings yet
- Entrepreneurship and Business Funding True/False Quiz (30 questionsDocument25 pagesEntrepreneurship and Business Funding True/False Quiz (30 questionsSaAl-ismailNo ratings yet
- 12 E Manzana InsuranceDocument13 pages12 E Manzana InsuranceShubham ShuklaNo ratings yet
- Willis Energy Market Review 2013 PDFDocument92 pagesWillis Energy Market Review 2013 PDFsushilk28No ratings yet
- Bcom 241 Risk and Insurance NotesDocument73 pagesBcom 241 Risk and Insurance NotesvictorNo ratings yet
- Financial Markets and Institutions 6th Edition Saunders Solutions Manual 1Document9 pagesFinancial Markets and Institutions 6th Edition Saunders Solutions Manual 1jess100% (31)
- IMC 2019 01 PorriniDocument18 pagesIMC 2019 01 PorriniYomi BrainNo ratings yet
- Sampoorna Raksha Supreme SRS Brochure V2Document10 pagesSampoorna Raksha Supreme SRS Brochure V2Devashish SahasrabudheNo ratings yet