You might also like
- 1 s2.0 S235198942200169X MainDocument14 pages1 s2.0 S235198942200169X MainSUCUITANA CCAIHUARI ANGELI ESTHERNo ratings yet
- B BE Assignment1Document9 pagesB BE Assignment1Siddhartha AryaNo ratings yet
- IBE - Financing Strategy - FINAL - 30 AugDocument8 pagesIBE - Financing Strategy - FINAL - 30 AugtennyNo ratings yet
- CW 2019 Spring Phoenix WordDocument81 pagesCW 2019 Spring Phoenix Wordapi-614383069No ratings yet
- Rapid PublicationDocument3 pagesRapid Publicationseda selyamanNo ratings yet
- Pineapple Cheese (Really) - SippitySupDocument10 pagesPineapple Cheese (Really) - SippitySupMariana AvGzNo ratings yet
- 習題 Ch06 1 Anderson 13e StatisticsDocument2 pages習題 Ch06 1 Anderson 13e StatisticsThi Trang NguyenNo ratings yet
- STRT-431 Reading Notes 10-12-21Document5 pagesSTRT-431 Reading Notes 10-12-21Drew JohnsonNo ratings yet
- Java (2) Lectures (6)Document33 pagesJava (2) Lectures (6)Mojtaba AlrasheedNo ratings yet
- Ce Afaceri Vroia Sa Faca Hunter Biden Baiatul Lui Joe Biden in Romania - Din Articol Nyt!Document43 pagesCe Afaceri Vroia Sa Faca Hunter Biden Baiatul Lui Joe Biden in Romania - Din Articol Nyt!Abelard BonaventuraNo ratings yet
- Theory 3Document21 pagesTheory 3Luis EduardoNo ratings yet
- The Genetics and Typical Traits of Thoracic Aortic Aneurysm and DissectionDocument34 pagesThe Genetics and Typical Traits of Thoracic Aortic Aneurysm and DissectionTlally Itzel Zamora CastroNo ratings yet
- D Adshead 2020Document201 pagesD Adshead 2020IamHederNo ratings yet
- NACDEC4Document18 pagesNACDEC4poNo ratings yet
- Math &esp With Tos 1st QuarterDocument24 pagesMath &esp With Tos 1st QuarterCristitaPobreSanchezNo ratings yet
- Importation, Exportation and Transportation of Goods: After Studying This Chapter, You Would Be Able ToDocument78 pagesImportation, Exportation and Transportation of Goods: After Studying This Chapter, You Would Be Able ToAbhishek SrivastavaNo ratings yet
- PWF 1Document12 pagesPWF 1Martin EgozcueNo ratings yet
- Science and TechnologyDocument40 pagesScience and TechnologyDEEPAK GUPTANo ratings yet
- Suspensions: Dr. Rabeea KhanDocument14 pagesSuspensions: Dr. Rabeea KhanAneela ManzoorNo ratings yet
- HDFC Life IR22 040622Document492 pagesHDFC Life IR22 040622Javed KhanNo ratings yet
- Capstone Final Report - Natural Disaster App - FinalDocument32 pagesCapstone Final Report - Natural Disaster App - Finalapi-498485959No ratings yet
- Ecpg OrlapDocument258 pagesEcpg OrlapNoha Ibraheem HelmyNo ratings yet
- Pgi 2020Document50 pagesPgi 2020ShishirNo ratings yet
- Photovoltaic Agricultural Internet of Things TowarDocument14 pagesPhotovoltaic Agricultural Internet of Things TowarvvipmembersNo ratings yet
- Philippines in The 19th CenturyDocument63 pagesPhilippines in The 19th CenturyAdrem RabinoNo ratings yet
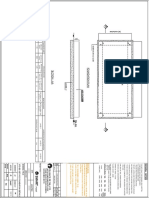
- SP STD - DG Set Foundation On Existing RCC Slab Details - r0 - GFC (100 MM A...Document1 pageSP STD - DG Set Foundation On Existing RCC Slab Details - r0 - GFC (100 MM A...ajay kumarNo ratings yet
- Love Verma Imt - SineflexDocument9 pagesLove Verma Imt - Sineflexlove vermaNo ratings yet
- 9531IIEDDocument50 pages9531IIEDAlex MuroNo ratings yet
- Mtech Cloud Computing BrochureDocument15 pagesMtech Cloud Computing BrochureMANISH KUMARNo ratings yet
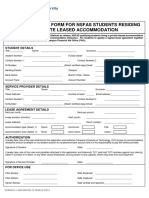
- NSFAS-Leased-applicationForm 2Document3 pagesNSFAS-Leased-applicationForm 2Alex SanchezNo ratings yet
- Objective 13Document7 pagesObjective 13Emmanuel ChichesterNo ratings yet
- 5 - Give It Up Social Marketing - 2022 PDFDocument22 pages5 - Give It Up Social Marketing - 2022 PDFSimran AgrawalNo ratings yet
- Preeclampsia 2022Document16 pagesPreeclampsia 2022Jose DuranNo ratings yet
- Jilla B. Alvarado P.E. 3 Answer SheetsDocument4 pagesJilla B. Alvarado P.E. 3 Answer SheetsWhencell Ann RomblonNo ratings yet
- 2.calculating Marginal Revenue From A Linear Deman...Document5 pages2.calculating Marginal Revenue From A Linear Deman...BLESSEDNo ratings yet
- SGPT SgotDocument1 pageSGPT SgotSumit AgrawalNo ratings yet
- May-22 CA Consolidated (A4 Format) - 8262457 - 2022 - 10 - 18 - 13 - 20Document161 pagesMay-22 CA Consolidated (A4 Format) - 8262457 - 2022 - 10 - 18 - 13 - 20Qazws QazwsNo ratings yet
- Supply Chain Risk Assessment: A Content Analysis-Based Literature ReviewDocument31 pagesSupply Chain Risk Assessment: A Content Analysis-Based Literature ReviewPAKIONo ratings yet
- Important Instructions To Examiners:: (Autonomous)Document25 pagesImportant Instructions To Examiners:: (Autonomous)Vaibhav BhagwatNo ratings yet
- LogDocument6 pagesLogHabil AbilNo ratings yet
- E-Admit Card: Please Read The Following Important Instructions CarefullyDocument3 pagesE-Admit Card: Please Read The Following Important Instructions CarefullyHARIKEERTHI NALLELLANo ratings yet
- Brills Express 25Document4 pagesBrills Express 25Jatin SoniNo ratings yet
- Electrical Water Heater - NewDocument12 pagesElectrical Water Heater - NewMotaz H OthmanNo ratings yet
- Mist LinuxDocument64 pagesMist LinuxMohammed Babar AhmedNo ratings yet
- A Level Biogeography NotesDocument35 pagesA Level Biogeography NotesBlessmore Chitanha100% (1)
- Idoc - Pub - Indian Company Listxls 2Document50 pagesIdoc - Pub - Indian Company Listxls 2pritthisNo ratings yet
- UntitledDocument26 pagesUntitledPratham 5hettyNo ratings yet
- World Wide Epidemiologt of FibromyalgiaDocument6 pagesWorld Wide Epidemiologt of FibromyalgiashanzaNo ratings yet
- Fichas en ColorDocument24 pagesFichas en ColorDavid Moure FernándezNo ratings yet
- Challan AxisDocument3 pagesChallan AxisSumit Darak50% (2)
- Kiri Mi 2016Document10 pagesKiri Mi 2016Eulalio Arámbul MuñozNo ratings yet
- Draft CWD Response and Management Plan 2023 2027Document79 pagesDraft CWD Response and Management Plan 2023 2027Dan LehrNo ratings yet
- Amchem Products Private LimitedDocument19 pagesAmchem Products Private LimitedAtika malikNo ratings yet
- G3550 Deviation ReportDocument1 pageG3550 Deviation ReportAWFAShop NajwahNo ratings yet
- Section25 Companies 6nov2008-17-19Document3 pagesSection25 Companies 6nov2008-17-19GSMPNo ratings yet
- Toxicological Profiles of Poisonous Edible and Medicinal MushroomsDocument7 pagesToxicological Profiles of Poisonous Edible and Medicinal MushroomsGion MurdochNo ratings yet
- Profibus DP Pressure Transmitter User Manual - 20121112 PDFDocument42 pagesProfibus DP Pressure Transmitter User Manual - 20121112 PDFLuis CristóbalNo ratings yet
- Tribal-Based Environmental Awareness For Contextualizing Indigenous People Education (IPED) Learners' Grade 10 Science LessonsDocument12 pagesTribal-Based Environmental Awareness For Contextualizing Indigenous People Education (IPED) Learners' Grade 10 Science LessonsPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Investigation of de Novo Variation in Pediatric CardiomyopathyDocument8 pagesInvestigation of de Novo Variation in Pediatric CardiomyopathyIsabella-Diana ChelbanNo ratings yet
- Obsessive-Compulsive Disorder: Retrospective Study On Clinical Characteristics and Family History in Outpatients CareDocument8 pagesObsessive-Compulsive Disorder: Retrospective Study On Clinical Characteristics and Family History in Outpatients CareTJPRC PublicationsNo ratings yet
- Relationship of ADHD, Depression, and Non-Tobacco Substance Use Disorders To Nicotine Dependence in Substance-Dependent DelinquentsDocument11 pagesRelationship of ADHD, Depression, and Non-Tobacco Substance Use Disorders To Nicotine Dependence in Substance-Dependent DelinquentsNaruto UzumakiNo ratings yet
- Pagano 2016Document29 pagesPagano 2016Naruto UzumakiNo ratings yet
- Huot 2011Document50 pagesHuot 2011Naruto UzumakiNo ratings yet
- Davis 2011Document5 pagesDavis 2011Naruto UzumakiNo ratings yet
- 10 1098@rsta 2019 0029Document13 pages10 1098@rsta 2019 0029Naruto UzumakiNo ratings yet
- Kish 2007Document12 pagesKish 2007Naruto UzumakiNo ratings yet
- Corkin 1983Document3 pagesCorkin 1983Naruto UzumakiNo ratings yet
- Ehrenkrantz 1999Document5 pagesEhrenkrantz 1999Naruto UzumakiNo ratings yet
- Searchinger Et Al Nature 2018Document4 pagesSearchinger Et Al Nature 2018Bjart HoltsmarkNo ratings yet
- Market AnalysisDocument143 pagesMarket AnalysisArivalagan VeluNo ratings yet
- Deed of Donation BicycleDocument2 pagesDeed of Donation BicycleCharlemagne PapioNo ratings yet
- Shahid Change ManagementDocument1 pageShahid Change Managementtanveer azamNo ratings yet
- 6A E21 Addendum 1 PDFDocument9 pages6A E21 Addendum 1 PDFAndres FCTNo ratings yet
- Polaris Ranger 500 ManualDocument105 pagesPolaris Ranger 500 ManualDennis aNo ratings yet
- Reflection of The Movie Informant - RevisedDocument3 pagesReflection of The Movie Informant - RevisedBhavika BhatiaNo ratings yet
- Bahasa InggrisDocument11 pagesBahasa InggrisrivanidurratulhikmahNo ratings yet
- Oracle E-Business Suite TechnicalDocument7 pagesOracle E-Business Suite Technicalmadhugover123No ratings yet
- Mark Magazine#64Document197 pagesMark Magazine#64Андрей КанищевNo ratings yet
- ASVAB Core ReviewDocument208 pagesASVAB Core Reviewstanley100% (1)
- C.V FinalDocument4 pagesC.V Finalcastillo_leoNo ratings yet
- Tatanka Oyate 2 EngDocument3 pagesTatanka Oyate 2 EngdesiNo ratings yet
- How To Write SpecificationsDocument9 pagesHow To Write SpecificationsLeilani ManalaysayNo ratings yet
- Camping Checklist: Essentials / Survival Sleep GearDocument2 pagesCamping Checklist: Essentials / Survival Sleep GearRomi Roberto100% (1)
- Axie Infinity Reviewer - by MhonDocument29 pagesAxie Infinity Reviewer - by MhonGodisGood AlltheTime100% (2)
- scs502 Module Three Observational Study WorksheetDocument2 pagesscs502 Module Three Observational Study Worksheetharshit.prajapati74No ratings yet
- Week - 14, Methods To Control Trade CycleDocument15 pagesWeek - 14, Methods To Control Trade CycleMuhammad TayyabNo ratings yet
- Intacc 1 NotesDocument19 pagesIntacc 1 NotesLouiseNo ratings yet
- Light Waves: Edexcel Igcse / Certificate in PhysicsDocument34 pagesLight Waves: Edexcel Igcse / Certificate in PhysicsertugozNo ratings yet
- BYD Case StudyDocument12 pagesBYD Case StudyELIZANo ratings yet
- John Stossel - Myths, Lies and Downright Stupidity - Get Out The Shovel - Why Everything You Know Is Wrong-Hyperion (2007) PDFDocument321 pagesJohn Stossel - Myths, Lies and Downright Stupidity - Get Out The Shovel - Why Everything You Know Is Wrong-Hyperion (2007) PDFdiegohrey239No ratings yet
- YCT 4 Vocabulary ListDocument14 pagesYCT 4 Vocabulary Listhauulty100% (1)
- 01-14 STP RSTP ConfigurationDocument67 pages01-14 STP RSTP ConfigurationKiKi MaNo ratings yet
- Poultry: Professional Products For The Poultry IndustryDocument1 pagePoultry: Professional Products For The Poultry IndustryzoilaNo ratings yet
- Zalando SE Q3 2023 Financials PDFDocument7 pagesZalando SE Q3 2023 Financials PDFHjraNo ratings yet
- Lesson 5 - 8ae AbsorptionDocument12 pagesLesson 5 - 8ae AbsorptionarnavprajeetNo ratings yet
- "Yfa - R : Keyboard Percussion RangesDocument2 pages"Yfa - R : Keyboard Percussion RangesmadroalNo ratings yet
- Sample Annotated BibliographyDocument1 pageSample Annotated Bibliographyfcrocco100% (1)
- Gender Inequality in Bangladesh PDFDocument20 pagesGender Inequality in Bangladesh PDFshakilnaimaNo ratings yet