You might also like
- ABGD Written Study Questions 2007Document291 pagesABGD Written Study Questions 2007velangni100% (1)
- Bone ReactionDocument9 pagesBone ReactionFourthMolar.comNo ratings yet
- The Effect of Dentures on Alveolar MucosaDocument8 pagesThe Effect of Dentures on Alveolar MucosaZachary DuongNo ratings yet
- ATWOODDocument15 pagesATWOODwaf51No ratings yet
- Isidor 1985Document9 pagesIsidor 1985Tania GonzálezNo ratings yet
- Relationships Between Dental Roots and Surrounding Tissues For Orthodontic Miniscrew InstallationDocument9 pagesRelationships Between Dental Roots and Surrounding Tissues For Orthodontic Miniscrew InstallationAbhay TandonNo ratings yet
- Goracci 1999Document7 pagesGoracci 1999Devin KwanNo ratings yet
- Osteoconductie PDFDocument5 pagesOsteoconductie PDFMoroianu MariusNo ratings yet
- The Effect of Zinc Oxide Based Sealer On Bone Defects HealingDocument8 pagesThe Effect of Zinc Oxide Based Sealer On Bone Defects HealingRadomir BaracNo ratings yet
- 10 1016@j TVJL 2019 105421Document27 pages10 1016@j TVJL 2019 105421Sergio Nieves MoranNo ratings yet
- Journal Pre-ProofDocument27 pagesJournal Pre-ProofSergio Nieves MoranNo ratings yet
- 4 Listgarten M. Electron Microscopic Study of The Gingivodental Junction of Man. Am J Anat 1966 119-147 (HWN)Document31 pages4 Listgarten M. Electron Microscopic Study of The Gingivodental Junction of Man. Am J Anat 1966 119-147 (HWN)Benjamin NgNo ratings yet
- Research and Education: Section EditorDocument12 pagesResearch and Education: Section EditorMayra Ortiz HerreraNo ratings yet
- Brane Mark 1983Document12 pagesBrane Mark 1983Alejandro MorenoNo ratings yet
- Boneceramic Graft Regenerates Alveolar Defects But Slows Orthodontic Tooth Movement With Less Root ResorptionDocument10 pagesBoneceramic Graft Regenerates Alveolar Defects But Slows Orthodontic Tooth Movement With Less Root Resorptionplayer osamaNo ratings yet
- Repair Processes of Experimental Root Fractures in Rat Molars Examined by Histopathological Techniques and 3D Micro-CT ImagingDocument8 pagesRepair Processes of Experimental Root Fractures in Rat Molars Examined by Histopathological Techniques and 3D Micro-CT ImagingAhmad Ulil AlbabNo ratings yet
- Oral Surg Oral Med Oral Pathol 1968 Seltzer-1Document13 pagesOral Surg Oral Med Oral Pathol 1968 Seltzer-1Zully Adanely Duron RobledoNo ratings yet
- Nasopalatine Duct Cyst - A Delayed Complication To Successful Dental Implant Placement - Diagnosis and Surgical Management - As Published in The JOIDocument6 pagesNasopalatine Duct Cyst - A Delayed Complication To Successful Dental Implant Placement - Diagnosis and Surgical Management - As Published in The JOIHashem Motahir Ali Al-ShamiriNo ratings yet
- Morphological Changes in the Denture Bearing Area After Tooth ExtractionDocument11 pagesMorphological Changes in the Denture Bearing Area After Tooth ExtractionEugenStanciuNo ratings yet
- Young2008 (1) - 1Document13 pagesYoung2008 (1) - 1dehaaNo ratings yet
- Pulp StoneDocument7 pagesPulp StoneWe BearsNo ratings yet
- Heterodonty and Tooth Replacement Patterns in Nile CrocodilesDocument7 pagesHeterodonty and Tooth Replacement Patterns in Nile CrocodilesJorge W. Moreno BernalNo ratings yet
- Prosthetic Dentistry: The Journal ofDocument3 pagesProsthetic Dentistry: The Journal ofNirav RathodNo ratings yet
- Ijomi 15 193 PDFDocument4 pagesIjomi 15 193 PDFBagis Emre GulNo ratings yet
- Microstructure of ImplantsDocument7 pagesMicrostructure of ImplantsghazyNo ratings yet
- The Relationship Between Dentin Microhardness and Tubule DensityDocument5 pagesThe Relationship Between Dentin Microhardness and Tubule DensitySitiKhadijahNo ratings yet
- Root Cementum Part 15Document10 pagesRoot Cementum Part 15Sumedha MalshetwarNo ratings yet
- Semen ToDocument4 pagesSemen ToyesikaichaaNo ratings yet
- Effect of Hyaluronic Acid On The Osseointegration of Dental ImplantsDocument5 pagesEffect of Hyaluronic Acid On The Osseointegration of Dental Implantsjaviers45No ratings yet
- 5.1963-X-Bjork-Variations in The Growth Pattern of The Human MandibleDocument12 pages5.1963-X-Bjork-Variations in The Growth Pattern of The Human MandibleAnaFlaviaMedinaNo ratings yet
- Alveolar Bone Preservation Subsequent To Miniscrew Implant Placement in A Canine ModelDocument9 pagesAlveolar Bone Preservation Subsequent To Miniscrew Implant Placement in A Canine ModelSamuel OtavioNo ratings yet
- Hermann COIR 2000 Biologic width around titanium implants a physiologically formed and stable dimension over time 拷貝Document11 pagesHermann COIR 2000 Biologic width around titanium implants a physiologically formed and stable dimension over time 拷貝歐亦焜No ratings yet
- Dimensions and Relations of The Dentogingival Junction in Humans. Gargiulo 1961Document7 pagesDimensions and Relations of The Dentogingival Junction in Humans. Gargiulo 1961Linda Garcia PNo ratings yet
- Estudio Histomorphometrico en InglesDocument5 pagesEstudio Histomorphometrico en InglesLauraNo ratings yet
- The Bio Degradation of HydroxyapatiteDocument7 pagesThe Bio Degradation of HydroxyapatiteAbhijit VargheseNo ratings yet
- CatalogoDocument7 pagesCatalogoIsabela Campos SánchezNo ratings yet
- The Ultrastructure of Spindles and Tufts in Human Dental EnamelDocument9 pagesThe Ultrastructure of Spindles and Tufts in Human Dental EnamelDr Urvashi SodvadiyaNo ratings yet
- Jzusb15 1064Document8 pagesJzusb15 1064Irfan Cahya PermanaNo ratings yet
- Safe Zone AjoDocument7 pagesSafe Zone AjojoeNo ratings yet
- Li ZhuDocument6 pagesLi ZhuM Faizal WinarisNo ratings yet
- The Butterfly Effect: An Investigation of Sectioned Roots: Basic Research - BiologyDocument3 pagesThe Butterfly Effect: An Investigation of Sectioned Roots: Basic Research - BiologyOmar TalibNo ratings yet
- Density of The Alveolar and Basal Bones of TheDocument8 pagesDensity of The Alveolar and Basal Bones of Theucsurortodoncia100% (1)
- Locating Broken NeedlesDocument3 pagesLocating Broken NeedlesmedicmayaNo ratings yet
- CO2 Laser Pulses Effectively Prevent Tooth DecayDocument5 pagesCO2 Laser Pulses Effectively Prevent Tooth DecaydigdouwNo ratings yet
- The Effects of Tooth Extraction On Alveolar Bone Biomechanics in The Miniature Pig, Sus ScrofaDocument7 pagesThe Effects of Tooth Extraction On Alveolar Bone Biomechanics in The Miniature Pig, Sus ScrofaSadullah TaşkınNo ratings yet
- Itsmo en Conducto Mesiobucal en Primera MolarDocument7 pagesItsmo en Conducto Mesiobucal en Primera MolarSaray ValerioNo ratings yet
- Pulpal changes following tooth reimplantation in dogsDocument5 pagesPulpal changes following tooth reimplantation in dogs謎超人No ratings yet
- 31 Ijss Nov cr02 - 2018Document4 pages31 Ijss Nov cr02 - 2018RAfii KerenNo ratings yet
- Lai 2012Document10 pagesLai 2012ARMADNo ratings yet
- Anemark 1969Document22 pagesAnemark 1969Carolina Dávila RamírezNo ratings yet
- 1 s2.0 S0022391315004990 Main PDFDocument4 pages1 s2.0 S0022391315004990 Main PDFFlori TabacaruNo ratings yet
- Art. 5 Analysis of The Internal Anatomy of Maxillary First Molars by Using Different MethodsDocument6 pagesArt. 5 Analysis of The Internal Anatomy of Maxillary First Molars by Using Different MethodsXime M.RNo ratings yet
- Methods For Stuoving Physical Growth:: Craniometr: yDocument16 pagesMethods For Stuoving Physical Growth:: Craniometr: yAhmed EleryanNo ratings yet
- Bodily Distalization of Molars With Absolute AnchorageDocument12 pagesBodily Distalization of Molars With Absolute AnchorageAnamika AttrishiNo ratings yet
- Maxillary Lateral Incisor with Four Root CanalsDocument5 pagesMaxillary Lateral Incisor with Four Root Canalsdentace1No ratings yet
- Missin Lateral ReplacementDocument6 pagesMissin Lateral ReplacementFourthMolar.comNo ratings yet
- Evaluation and New Classification of Alveolar BoneDocument8 pagesEvaluation and New Classification of Alveolar BonerizkaNo ratings yet
- Correlative Microscopy of Bone in Implant Osteointegration StudiesDocument9 pagesCorrelative Microscopy of Bone in Implant Osteointegration StudiesMarilisa QuarantaNo ratings yet
- Case ReportDocument4 pagesCase ReportAjeng Narita CaustinaNo ratings yet
- PIIS1098301518322721Document7 pagesPIIS1098301518322721Francelia Quiñonez RuvalcabaNo ratings yet
- Comparison of Two Survey Instruments Measuring Quality of Life in Pediatric Dentofacial PatientsDocument6 pagesComparison of Two Survey Instruments Measuring Quality of Life in Pediatric Dentofacial PatientsFrancelia Quiñonez RuvalcabaNo ratings yet
- Effects of Diabetes On Apoptosis and Mitosis in Rat HippocampusDocument9 pagesEffects of Diabetes On Apoptosis and Mitosis in Rat HippocampusFrancelia Quiñonez RuvalcabaNo ratings yet
- Ikarashi 1992Document18 pagesIkarashi 1992Francelia Quiñonez RuvalcabaNo ratings yet
- Complement and T Cell RegulationDocument41 pagesComplement and T Cell RegulationFrancelia Quiñonez RuvalcabaNo ratings yet
- Osseointegration of Zirconia Dental Implants in Animal Investigations - A Systematic Review and Meta-AnalysisDocument12 pagesOsseointegration of Zirconia Dental Implants in Animal Investigations - A Systematic Review and Meta-AnalysisFrancelia Quiñonez RuvalcabaNo ratings yet
- An Update of Gorlin-Goltz Syndrome: Aliya Hasan, Dapo AkintolaDocument4 pagesAn Update of Gorlin-Goltz Syndrome: Aliya Hasan, Dapo AkintolaFrancelia Quiñonez RuvalcabaNo ratings yet
- Cshperspect III A016303Document19 pagesCshperspect III A016303Francelia Quiñonez RuvalcabaNo ratings yet
- BiomedPap - Bio 202001 0002Document11 pagesBiomedPap - Bio 202001 0002Francelia Quiñonez RuvalcabaNo ratings yet
- Cancer BucalDocument6 pagesCancer BucalFrancelia Quiñonez RuvalcabaNo ratings yet
- Manejo Comportamiento Pediatrico PDFDocument27 pagesManejo Comportamiento Pediatrico PDFSARA VICTORIA HERNANDEZ ESPINELNo ratings yet
- Manzano 2014Document10 pagesManzano 2014Francelia Quiñonez RuvalcabaNo ratings yet
- Heineman Complete Test OneDocument24 pagesHeineman Complete Test OneGerardo Bahena33% (3)
- Review Article: Periodontal Diseases and Dental Caries in Children With Type 1 Diabetes MellitusDocument9 pagesReview Article: Periodontal Diseases and Dental Caries in Children With Type 1 Diabetes MellitusFrancelia Quiñonez RuvalcabaNo ratings yet
- Heineman Complete Test OneDocument24 pagesHeineman Complete Test OneGerardo Bahena33% (3)
- Prenatal Exposure To Gestational Diabetes Mellitus Increases Developmental Defects in The Enamel of OffspringDocument16 pagesPrenatal Exposure To Gestational Diabetes Mellitus Increases Developmental Defects in The Enamel of OffspringFrancelia Quiñonez RuvalcabaNo ratings yet
- Heineman Complete Test OneDocument24 pagesHeineman Complete Test OneGerardo Bahena33% (3)
- Anaphylaxis ArticuloDocument12 pagesAnaphylaxis ArticuloFrancelia Quiñonez RuvalcabaNo ratings yet
- Anaphylaxis Articulo CompletoDocument6 pagesAnaphylaxis Articulo CompletoFrancelia Quiñonez RuvalcabaNo ratings yet
- TOEFL PBT BookDocument93 pagesTOEFL PBT Bookaqua_6978% (9)
- Anaphylaxis Articulo CompletoDocument6 pagesAnaphylaxis Articulo CompletoFrancelia Quiñonez RuvalcabaNo ratings yet
- D475a-5gen00051 Fa-03Document240 pagesD475a-5gen00051 Fa-03Gabo GaboNo ratings yet
- ch05 PDFDocument11 pagesch05 PDFKaren PedrazaNo ratings yet
- Thermodynamics SolutionDocument15 pagesThermodynamics SolutionSureshbabu0% (1)
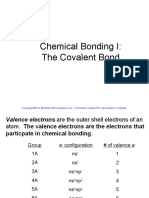
- Chemical Bonding I The Covalent Bond Copyright © The McGraw-Hill CompaniesDocument87 pagesChemical Bonding I The Covalent Bond Copyright © The McGraw-Hill CompaniesRoll OutNo ratings yet
- ARV-WT112 (U) : Wafer Type Butterfly Valve Universal FlangedDocument2 pagesARV-WT112 (U) : Wafer Type Butterfly Valve Universal FlangedmalNo ratings yet
- Balancing Equations: Practice ProblemsDocument10 pagesBalancing Equations: Practice ProblemsJesse Jhei LedesmaNo ratings yet
- Glenmark Unveils Its Strategic Blueprint For Transition Into An Innovation ) Led Global Pharmaceutical Organization in The Next Decade (Company Update)Document31 pagesGlenmark Unveils Its Strategic Blueprint For Transition Into An Innovation ) Led Global Pharmaceutical Organization in The Next Decade (Company Update)Shyam SunderNo ratings yet
- Visionaire 2 3 Service Manual English PDFDocument47 pagesVisionaire 2 3 Service Manual English PDFQuarmina HesseNo ratings yet
- CHE026L Lab Activity Sheet #5: Ionic and Covalent BondsDocument7 pagesCHE026L Lab Activity Sheet #5: Ionic and Covalent BondsZeian Jacob BaylaNo ratings yet
- Biological FarmingDocument60 pagesBiological Farmingnated854834100% (1)
- Eaton HosesDocument17 pagesEaton HosesHesham HusseinNo ratings yet
- Insam - Recycling of Biomass Ashes PDFDocument173 pagesInsam - Recycling of Biomass Ashes PDFingjorgeveraNo ratings yet
- PERIZYM AFW TDS enDocument3 pagesPERIZYM AFW TDS enDesyree VeraNo ratings yet
- STP0194-3 Iridescence Paper222 - IOM Conf March 2007Document9 pagesSTP0194-3 Iridescence Paper222 - IOM Conf March 2007George MaNo ratings yet
- NMR Spectroscopy: The TheoryDocument4 pagesNMR Spectroscopy: The Theoryoliv1aNo ratings yet
- In-Line Coagulation With Low-Pressure Membrane Filtration: Kevin Young-June Choi, Brian A. DempseyDocument11 pagesIn-Line Coagulation With Low-Pressure Membrane Filtration: Kevin Young-June Choi, Brian A. DempseyM TNo ratings yet
- Ionic Equilibrium WSDocument20 pagesIonic Equilibrium WSVishal MNo ratings yet
- Chapter18 CarbohydratesDocument68 pagesChapter18 CarbohydratesMaria Francesca Tiongson0% (1)
- Protective Coatings: Product CatalogueDocument40 pagesProtective Coatings: Product Cataloguegns1234567890No ratings yet
- Turbine Efficiency CalculationDocument5 pagesTurbine Efficiency CalculationĐồng Hoàng TrungNo ratings yet
- Coordination Chemistry Reviews Volume 249 Issue 17-18 2005 (Doi 10.1016/j.ccr.2005.02.002) Remy Van Gorkum Elisabeth Bouwman - The Oxidative Drying of Alkyd Paint Catalysed by Metal ComplexesDocument20 pagesCoordination Chemistry Reviews Volume 249 Issue 17-18 2005 (Doi 10.1016/j.ccr.2005.02.002) Remy Van Gorkum Elisabeth Bouwman - The Oxidative Drying of Alkyd Paint Catalysed by Metal ComplexesSarah SandsNo ratings yet
- Biochemistry-UNIT 4Document38 pagesBiochemistry-UNIT 4Kezia RobinNo ratings yet
- Bulking of SandDocument2 pagesBulking of SandEngr Sarang KhanNo ratings yet
- Performance Coatings - Greenheck FansDocument12 pagesPerformance Coatings - Greenheck Fansprsum_572100% (1)
- Astm A 424 - 00 - QtqynaDocument2 pagesAstm A 424 - 00 - QtqynaEjat ISNo ratings yet
- Bioline Pricing 2020Document4 pagesBioline Pricing 2020Asrul M FuadNo ratings yet
- 7 Segment DatasheetDocument10 pages7 Segment DatasheetAndrea MifsudNo ratings yet
- Model QuestionsDocument1 pageModel QuestionsSurya GowdaNo ratings yet
- Hydrogen Fuel of The FutureDocument184 pagesHydrogen Fuel of The FutureDefEntNo ratings yet
- Understanding Air Quality Index (AQIDocument2 pagesUnderstanding Air Quality Index (AQIPuvan66No ratings yet