You might also like
- New Microsoft Word DocumentDocument6 pagesNew Microsoft Word DocumentKawther El-FikyNo ratings yet
- Title: HypoglycemiaDocument13 pagesTitle: Hypoglycemia025 MUHAMAD HAZIQ BIN AHMAD AZMANNo ratings yet
- Proficiency Testbuilder 4th EditionDocument27 pagesProficiency Testbuilder 4th EditionNgan LeNo ratings yet
- Diabetic KetoacidosisDocument7 pagesDiabetic KetoacidosisetengNo ratings yet
- Diabetes MellitusDocument11 pagesDiabetes MellitusSallieNo ratings yet
- 4hyperosmolar Hyperglycemic State (HHS)Document121 pages4hyperosmolar Hyperglycemic State (HHS)desy f sarahNo ratings yet
- Diabetes OverviewDocument38 pagesDiabetes OverviewKye GarciaNo ratings yet
- Grp.10 DiabetesDocument15 pagesGrp.10 DiabetesVanessa JanneNo ratings yet
- Diabetes Case Study Fall 2016 1Document7 pagesDiabetes Case Study Fall 2016 1api-284823421No ratings yet
- Diabetic KetoacidosisDocument3 pagesDiabetic KetoacidosisJanna FavilaNo ratings yet
- Emergency Medicine EducationHyperglycemic Hyperosmolar State: ED PRDocument19 pagesEmergency Medicine EducationHyperglycemic Hyperosmolar State: ED PRSyed Shahrul Naz SyedNo ratings yet
- Definition of Diabetes Mellitus (DM)Document12 pagesDefinition of Diabetes Mellitus (DM)Romarc Owen CorpuzNo ratings yet
- Case Study On Diabetes MellitusDocument12 pagesCase Study On Diabetes Mellitusferdz02No ratings yet
- CHF Secondary To COPD and DM Type 2Document3 pagesCHF Secondary To COPD and DM Type 2Ma Regina Ocio PatanaNo ratings yet
- Diagnosis and Management HiperglikemiDocument13 pagesDiagnosis and Management HiperglikemiTasya SylviaNo ratings yet
- Diabetes Mellitus Is A Group of Metabolic Diseases Characterized byDocument67 pagesDiabetes Mellitus Is A Group of Metabolic Diseases Characterized byBivek TimalsinaNo ratings yet
- Complications of Diabetes MellitusDocument49 pagesComplications of Diabetes MellitusJennifer WootenNo ratings yet
- What Is A Subchorionic HemorrhageDocument4 pagesWhat Is A Subchorionic HemorrhageBudo LataquinNo ratings yet
- CC EP 126 Diabetes Mellitus and Disorders of Glucose Homeostasis Ch. 118 Rosens 9th Ed. 1Document13 pagesCC EP 126 Diabetes Mellitus and Disorders of Glucose Homeostasis Ch. 118 Rosens 9th Ed. 1Ikenna EzeiloNo ratings yet
- Anesthesia and Diabetes: Marwa Ahmad MahrousDocument79 pagesAnesthesia and Diabetes: Marwa Ahmad MahrousAjengNo ratings yet
- Case Pres 1Document7 pagesCase Pres 1Bright SunshinenNo ratings yet
- Cerebral Ischemic Damage in Diabetes: An Inflammatory PerspectiveDocument22 pagesCerebral Ischemic Damage in Diabetes: An Inflammatory PerspectiveAnonymous QPakSNNo ratings yet
- Acute Complications of Diabetes MellitusDocument13 pagesAcute Complications of Diabetes MellitusMark Christian M. GonzagaNo ratings yet
- ReadingsDocument24 pagesReadingsBryant Riego IIINo ratings yet
- Diabetes MellitusDocument21 pagesDiabetes MellitusJuri GallosNo ratings yet
- Clinical Review: Diabetic Ketoacidosis in AdultsDocument8 pagesClinical Review: Diabetic Ketoacidosis in AdultscitrahmahNo ratings yet
- Hypoglycemia in Diabetes: P E. C, S N. D, H SDocument11 pagesHypoglycemia in Diabetes: P E. C, S N. D, H SFabio FabbriNo ratings yet
- Metabolic Disturbance and EncephalopathyDocument33 pagesMetabolic Disturbance and EncephalopathyBayu Surya DanaNo ratings yet
- Approach To The Hypoglycemic PatientDocument13 pagesApproach To The Hypoglycemic PatientFiorella Peña Mora100% (2)
- Ijms 24 09357 v2Document14 pagesIjms 24 09357 v2MSNo ratings yet
- Signs and SymptDocument14 pagesSigns and SymptVealma sikaNo ratings yet
- A Review of The Hybrid Description of Diabetes MellitusDocument4 pagesA Review of The Hybrid Description of Diabetes MellitusIJRDPM JOURNALNo ratings yet
- Journal ReadingDocument7 pagesJournal Readingdr AnnisaNo ratings yet
- Acute and Chronic DM ComplicationsDocument29 pagesAcute and Chronic DM ComplicationsJennicaNo ratings yet
- Complications of D Iabetes M EllitusDocument49 pagesComplications of D Iabetes M EllitusJadika An GunaNo ratings yet
- Hyperosmolar Hyperglycemic State in Type 2 Diabetes Type 2 MellitusDocument3 pagesHyperosmolar Hyperglycemic State in Type 2 Diabetes Type 2 MellitusFrancis PeterosNo ratings yet
- Jurnal Hipoglikemia 1Document11 pagesJurnal Hipoglikemia 1dimas gilang prakosoNo ratings yet
- Sectio N Subjec T: Hormonal Disorders Diabetes Mellitus (DM)Document8 pagesSectio N Subjec T: Hormonal Disorders Diabetes Mellitus (DM)musimsemiNo ratings yet
- Classification: LiverDocument20 pagesClassification: LivertermskipopNo ratings yet
- UntitledDocument33 pagesUntitledMadhura BharathaNo ratings yet
- Case Report GeriatricDocument29 pagesCase Report Geriatricjoanna fitzmorrisNo ratings yet
- Diabetes MellitusDocument24 pagesDiabetes MellitusAnsh Gaurav KumarNo ratings yet
- W02 - Diabetic Emergencies in CCDocument36 pagesW02 - Diabetic Emergencies in CCHelene AlawamiNo ratings yet
- Diabetes Mellitus HospitalDocument29 pagesDiabetes Mellitus HospitalgegeNo ratings yet
- Diabetes Mellitus CommunityDocument23 pagesDiabetes Mellitus CommunityJoychukzNo ratings yet
- Diabetes Overview: Aerobic Exercise ClassDocument13 pagesDiabetes Overview: Aerobic Exercise Classpak3maNo ratings yet
- Pathophysiology of StrokeDocument7 pagesPathophysiology of StrokeCHANDAN RAINo ratings yet
- Diabetes Mellitus: Mark E - MolitchDocument3 pagesDiabetes Mellitus: Mark E - MolitchCakra Parindra GasmaraNo ratings yet
- Hyperosmolar Hyperglycemic State (HHS) : Rahayu Oktaliani Aywar ZamriDocument6 pagesHyperosmolar Hyperglycemic State (HHS) : Rahayu Oktaliani Aywar Zamrirsud curupNo ratings yet
- Correlation Between Diabetes and Coronary Artery DiseaseDocument18 pagesCorrelation Between Diabetes and Coronary Artery Diseaserahmat safryansyahNo ratings yet
- DiabetesDocument4 pagesDiabetesTuTitNo ratings yet
- Presentation On Diabetes Mellitus in Pharmacology LabDocument35 pagesPresentation On Diabetes Mellitus in Pharmacology Labpurwo yuhantoNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFAlejandro Guerrero LeónNo ratings yet
- Chapter One 1.1 DefinitionDocument6 pagesChapter One 1.1 Definitiontsalawa globentNo ratings yet
- Diabetic Ketoacidosis: Claire P. SmithDocument6 pagesDiabetic Ketoacidosis: Claire P. SmithPaco OrtezNo ratings yet
- Pediatric Type 1 Diabetes MellitusDocument25 pagesPediatric Type 1 Diabetes MellitusmuhammadferhatNo ratings yet
- DIABETES CorrectedDocument16 pagesDIABETES CorrectedBlaise PascalNo ratings yet
- HypoglycemicDocument13 pagesHypoglycemicherberthdj22No ratings yet
- Hyperglycaemic EmergenciesDocument11 pagesHyperglycaemic EmergenciesdramaysinghNo ratings yet
- Discover Natural -Alternative Therapies for Managing Type 2 DiabetesFrom EverandDiscover Natural -Alternative Therapies for Managing Type 2 DiabetesNo ratings yet
- Uni CodeDocument4 pagesUni CodeElenaDiSavoiaNo ratings yet
- DementiaDocument6 pagesDementiaElenaDiSavoiaNo ratings yet
- Biography: Erdinand de Saussure (Document7 pagesBiography: Erdinand de Saussure (ElenaDiSavoiaNo ratings yet
- CovidDocument3 pagesCovidElenaDiSavoiaNo ratings yet
- Nešto 1Document3 pagesNešto 1ElenaDiSavoiaNo ratings yet
- Nešto 2Document5 pagesNešto 2ElenaDiSavoiaNo ratings yet
- Singapore: Jump To Navigation Jump To SearchDocument7 pagesSingapore: Jump To Navigation Jump To SearchElenaDiSavoiaNo ratings yet
- Small Molecule: Molecular Weight CutoffDocument3 pagesSmall Molecule: Molecular Weight CutoffElenaDiSavoiaNo ratings yet
- Poly - Mer: Cartoon Schematic of Polymer MoleculesDocument7 pagesPoly - Mer: Cartoon Schematic of Polymer MoleculesElenaDiSavoiaNo ratings yet
- Origin of TermDocument11 pagesOrigin of TermElenaDiSavoiaNo ratings yet
- LangDocument5 pagesLangElenaDiSavoiaNo ratings yet
- TankaDocument3 pagesTankaElenaDiSavoiaNo ratings yet
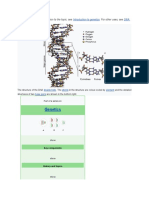
- Genetics: For A Non-Technical Introduction To The Topic, See - For Other Uses, SeeDocument8 pagesGenetics: For A Non-Technical Introduction To The Topic, See - For Other Uses, SeeElenaDiSavoiaNo ratings yet
- CineDocument9 pagesCineElenaDiSavoiaNo ratings yet
- Yokohama (: PronouncedDocument5 pagesYokohama (: PronouncedElenaDiSavoiaNo ratings yet
- Osaka: Osaka Prefecture Osaka (Disambiguation)Document19 pagesOsaka: Osaka Prefecture Osaka (Disambiguation)ElenaDiSavoiaNo ratings yet
- Shinobu Orikuchi: Inline CitationsDocument3 pagesShinobu Orikuchi: Inline CitationsElenaDiSavoiaNo ratings yet
- QigwbeandsDocument1 pageQigwbeandsElenaDiSavoiaNo ratings yet
- Lineage: Matthew Calbraith Perry (April 10, 1794 - March 4, 1858) Was ADocument4 pagesLineage: Matthew Calbraith Perry (April 10, 1794 - March 4, 1858) Was AElenaDiSavoiaNo ratings yet
- Endocrinology, Diabetes, and Metabolism - American Board of Internal Medicine - ABIMDocument3 pagesEndocrinology, Diabetes, and Metabolism - American Board of Internal Medicine - ABIMabimorgNo ratings yet
- Guía de HormonasDocument2 pagesGuía de HormonasMontserrat LandaNo ratings yet
- The Endocrine System: Did You KnowDocument40 pagesThe Endocrine System: Did You Knowmir-medicinaNo ratings yet
- Cushing's DiseaseDocument2 pagesCushing's DiseaseHari SaduNo ratings yet
- Diabetes Mellitus Case StudyDocument5 pagesDiabetes Mellitus Case StudyRainier Rhett Concha86% (7)
- EXPOSITORY ESSAY DiabetesDocument1 pageEXPOSITORY ESSAY DiabetesSaida BallesteroNo ratings yet
- Criteria For Diagnosing PCOS Diagnosing HA Over PCOS: No Period. Now What?Document1 pageCriteria For Diagnosing PCOS Diagnosing HA Over PCOS: No Period. Now What?Andra SpatarNo ratings yet
- Thyroid GlandDocument10 pagesThyroid GlandSheena Mae Atienza100% (2)
- Primary HyperparathyroidismDocument50 pagesPrimary HyperparathyroidismKate ClarksonNo ratings yet
- Endocrine SystemDocument27 pagesEndocrine Systemcardos cherry100% (1)
- Butler Et Al, 2021.Document22 pagesButler Et Al, 2021.Jeje MystearicaNo ratings yet
- Endocrine Part 2 DRAFTDocument6 pagesEndocrine Part 2 DRAFTPreeti Joan BuxaniNo ratings yet
- Sample Case: EndocrinologyDocument42 pagesSample Case: EndocrinologyCoy NuñezNo ratings yet
- Tabel GlucoseDocument1 pageTabel GlucoseOscar Dwn YapNo ratings yet
- Zoology HonsDocument80 pagesZoology HonsSantosh MahathaNo ratings yet
- Physio Ex Act 4Document4 pagesPhysio Ex Act 4alifia azzahraNo ratings yet
- Blood TSH ReportDocument1 pageBlood TSH Reportshilpishukla1191No ratings yet
- 3 Orris PcosDocument65 pages3 Orris PcosxtineNo ratings yet
- Diseases of The Endocrine SystemDocument2 pagesDiseases of The Endocrine SystemAlexs VillafloresNo ratings yet
- The Endocrine System: BIO 201, Dr. Colette Kabrita-Bou Serhal, Adapted From John Wiley & Sons, Inc.Document19 pagesThe Endocrine System: BIO 201, Dr. Colette Kabrita-Bou Serhal, Adapted From John Wiley & Sons, Inc.Melissa ChehwaneNo ratings yet
- Laboratory Activity Endocrinology: Table 1: Different Classes of HormonesDocument6 pagesLaboratory Activity Endocrinology: Table 1: Different Classes of HormonesJohn Fritz Gerald BascoNo ratings yet
- Endocrinology SlidesDocument344 pagesEndocrinology SlidesleanNo ratings yet
- 1 Adrenal CortexDocument15 pages1 Adrenal CortexMarion Lawrence LaraNo ratings yet
- FLGX213 Glucose Practical Assignment 1Document5 pagesFLGX213 Glucose Practical Assignment 1Martha FormalNo ratings yet
- Insulin Sliding ScaleDocument2 pagesInsulin Sliding Scaleberman fernandoNo ratings yet
- Artificial Pancreas Technology Offers Hope For Childhood DiabetesDocument11 pagesArtificial Pancreas Technology Offers Hope For Childhood DiabetesDiana PeñalozaNo ratings yet
- Glucocorticoid Therapy and Adrenal SuppressionDocument8 pagesGlucocorticoid Therapy and Adrenal SuppressionFan AccountNo ratings yet
- The Basics of Diabetes: Phar 811 Peyton Teets Pharmd Candidate School of Pharmacy - West Virginia UniversityDocument39 pagesThe Basics of Diabetes: Phar 811 Peyton Teets Pharmd Candidate School of Pharmacy - West Virginia UniversityMa'rifatulAuliaNo ratings yet
- CBG MonitoringDocument15 pagesCBG MonitoringIvette RiveraNo ratings yet
- Histology of The Endocrine System: Ma. Minda Luz M. Manuguid, M.DDocument27 pagesHistology of The Endocrine System: Ma. Minda Luz M. Manuguid, M.Dchocoholic potchiNo ratings yet