You might also like
- Continuous Glucose MonitoringFrom EverandContinuous Glucose MonitoringWeiping JiaNo ratings yet
- Does Continuous Glucose Monitoring Really Improve Diabetes ManagementDocument3 pagesDoes Continuous Glucose Monitoring Really Improve Diabetes ManagementjohnNo ratings yet
- Artificial Pancreas - RAEE 2017 PDFDocument6 pagesArtificial Pancreas - RAEE 2017 PDFZeeshanNo ratings yet
- A Fuzzy Controller For Blood Glucose-Insulin SysteDocument7 pagesA Fuzzy Controller For Blood Glucose-Insulin SysteBrasoveanu Gheorghita100% (1)
- Research Article: Continuous Drug Infusion For Diabetes Therapy: A Closed-Loop Control System DesignDocument10 pagesResearch Article: Continuous Drug Infusion For Diabetes Therapy: A Closed-Loop Control System DesignBrasoveanu GheorghitaNo ratings yet
- NIH Public Access: Author ManuscriptDocument19 pagesNIH Public Access: Author ManuscriptmilaNo ratings yet
- Continuous Glucose Monitoring 508Document4 pagesContinuous Glucose Monitoring 508Hadi jameel HadiNo ratings yet
- Divya 13Document20 pagesDivya 13Divya NadarNo ratings yet
- Bhattacharjee 2018Document12 pagesBhattacharjee 2018Brasoveanu GheorghitaNo ratings yet
- Flash Glucose MonitoringDocument9 pagesFlash Glucose MonitoringAneed AnandNo ratings yet
- Biomedical Signal Processing and Control: Iftikhar Ahmad, Faysal Munir, Muhammad Faizan MunirDocument8 pagesBiomedical Signal Processing and Control: Iftikhar Ahmad, Faysal Munir, Muhammad Faizan MunirBrasoveanu GheorghitaNo ratings yet
- Standards of Medical Care in Diabetesd2018: 6. Glycemic TargetsDocument10 pagesStandards of Medical Care in Diabetesd2018: 6. Glycemic TargetsJimmy GrefaNo ratings yet
- Standards of Medical Care in Diabetesd2018: 6. Glycemic TargetsDocument2 pagesStandards of Medical Care in Diabetesd2018: 6. Glycemic TargetsJimmy GrefaNo ratings yet
- LibreView Guide - Italian PaperDocument12 pagesLibreView Guide - Italian PaperJesus MuñozNo ratings yet
- Comparative Analysis of PID Tuning Techniques For Blood Glucose Level of Diabetic PatientDocument6 pagesComparative Analysis of PID Tuning Techniques For Blood Glucose Level of Diabetic Patient015Maulana Malik IbrahimNo ratings yet
- Journal Pone 0248280 PDFDocument17 pagesJournal Pone 0248280 PDFHafis KafitNo ratings yet
- Dia 2017 2525 AbstractsDocument134 pagesDia 2017 2525 AbstractsPranav Kumar Prabhakar100% (1)
- Study Guide Blood Glucose MonitoringDocument4 pagesStudy Guide Blood Glucose MonitoringDan Dan ManaoisNo ratings yet
- Study Guide Blood Glucose MonitoringDocument4 pagesStudy Guide Blood Glucose Monitoringjon elleNo ratings yet
- Artificial PancreasDocument2 pagesArtificial PancreasrameshjeyNo ratings yet
- Glycemic Target ADA 2018Document10 pagesGlycemic Target ADA 2018Selly DamayantiNo ratings yet
- Run-to-Run Control of Blood Glucose Concentrations For People With Type 1 Diabetes MellitusDocument10 pagesRun-to-Run Control of Blood Glucose Concentrations For People With Type 1 Diabetes MellitusKamila Nanda RezkyNo ratings yet
- Digital Technology For DiabetesDocument11 pagesDigital Technology For Diabetesvvandv123No ratings yet
- Paper 2 HighlightedDocument9 pagesPaper 2 HighlightedVaishnavi YacheNo ratings yet
- Apd T1DMDocument11 pagesApd T1DMmuhammad syafiqNo ratings yet
- Jurnal Pemeriksaan Glukosa DarahDocument9 pagesJurnal Pemeriksaan Glukosa DarahIntan TafriNo ratings yet
- Robust PBPK/PD-Based Model PredictiveDocument13 pagesRobust PBPK/PD-Based Model PredictivenhatvpNo ratings yet
- International Journal Insulin DosingDocument12 pagesInternational Journal Insulin DosingMutia Ramadini91No ratings yet
- In Range StudyDocument11 pagesIn Range Studyhssdj2hfdmNo ratings yet
- Blood Glucose: Measurement in The Point-of-Care SettingDocument7 pagesBlood Glucose: Measurement in The Point-of-Care SettingSaritaJQMNo ratings yet
- Sensors: Advanced Diabetes Management Using Artificial Intelligence and Continuous Glucose Monitoring SensorsDocument18 pagesSensors: Advanced Diabetes Management Using Artificial Intelligence and Continuous Glucose Monitoring SensorsShujian ZhaoNo ratings yet
- Stepwise Approach To Continuous Glucose Monitoring Interpretation For Internists and Family PhysiciansDocument10 pagesStepwise Approach To Continuous Glucose Monitoring Interpretation For Internists and Family PhysiciansRafael Baybay100% (1)
- Advancement in Insulcagon Pump Simulating As An Artificial Pancreas For The Treatment of DiabetesDocument5 pagesAdvancement in Insulcagon Pump Simulating As An Artificial Pancreas For The Treatment of Diabetesmosca90No ratings yet
- Artificial Pancreas System For Type 1 Diabetes-Challenges and AdvancementsDocument12 pagesArtificial Pancreas System For Type 1 Diabetes-Challenges and Advancementsmuhammad syafiqNo ratings yet
- Closed-Loop Insulin Delivery For Treatment of Type 1 DiabetesDocument9 pagesClosed-Loop Insulin Delivery For Treatment of Type 1 DiabetesPreda ManuelaNo ratings yet
- Saint Paul University Philippines: Master of Science in NursingDocument15 pagesSaint Paul University Philippines: Master of Science in NursingGorgieNo ratings yet
- Saint Paul University Philippines: Master of Science in NursingDocument17 pagesSaint Paul University Philippines: Master of Science in NursingGorgieNo ratings yet
- Standards of Medical Care in Diabetesd2018: 6. Glycemic TargetsDocument10 pagesStandards of Medical Care in Diabetesd2018: 6. Glycemic TargetsjeanetteNo ratings yet
- Ajtr0014 4757Document20 pagesAjtr0014 4757Eyal RobinsonNo ratings yet
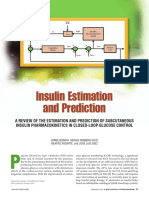
- Insulin Estimation and PredictionDocument20 pagesInsulin Estimation and PredictionLorenzo IraceNo ratings yet
- Automated Insulin Delivery Benefits, Challenges, and RecommendationDocument20 pagesAutomated Insulin Delivery Benefits, Challenges, and RecommendationpremamoyNo ratings yet
- Experience With The Continuous Glucose Monitoring System in A Medical Intensive Care UnitDocument10 pagesExperience With The Continuous Glucose Monitoring System in A Medical Intensive Care UnitjohnNo ratings yet
- Thorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsDocument12 pagesThorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsgercampeNo ratings yet
- Performance Evaluation of The GlunovoR ContinuousDocument13 pagesPerformance Evaluation of The GlunovoR ContinuousshahirahNo ratings yet
- Content ServerDocument7 pagesContent Serverdev darma karinggaNo ratings yet
- Sensors 20 01705Document11 pagesSensors 20 01705QSilvaNo ratings yet
- 7 Diabetes Technology Standards Ofmedical Carein Diabetesd2020Document12 pages7 Diabetes Technology Standards Ofmedical Carein Diabetesd2020eberthhuarachNo ratings yet
- Does Minimed 780G Insulin Pump System Affect Energy and Nutrient Intake?: Long-Term Follow-Up StudyDocument7 pagesDoes Minimed 780G Insulin Pump System Affect Energy and Nutrient Intake?: Long-Term Follow-Up StudyDaniel VazquezNo ratings yet
- Insulin Control System For Diabetic Patients by Using Adaptive ControllerDocument6 pagesInsulin Control System For Diabetic Patients by Using Adaptive ControllerPreda ManuelaNo ratings yet
- Artificial Intelligence in Medicine: Virginie Felizardo, Nuno M. Garcia, Nuno Pombo, Imen MegdicheDocument15 pagesArtificial Intelligence in Medicine: Virginie Felizardo, Nuno M. Garcia, Nuno Pombo, Imen MegdicheShujian ZhaoNo ratings yet
- Glycemic Targets: American Diabetes AssociationDocument8 pagesGlycemic Targets: American Diabetes AssociationHelenaNo ratings yet
- Original ArticleDocument10 pagesOriginal ArticlegistaluvikaNo ratings yet
- Time-Delay Model-Based Control of The Glucose-Insulin System, by Means of A State ObserverDocument16 pagesTime-Delay Model-Based Control of The Glucose-Insulin System, by Means of A State ObserverChanachai PuckNo ratings yet
- Blood Glucose Regulation in Diabetics Using Sliding Mode Control TechniquesDocument14 pagesBlood Glucose Regulation in Diabetics Using Sliding Mode Control TechniquesTri RachmadijantoNo ratings yet
- Ethnicity of Participants Number of Times Monitor Is Scanned Per DayDocument1 pageEthnicity of Participants Number of Times Monitor Is Scanned Per DaysanajagraNo ratings yet
- 134 2021 Article 6526Document13 pages134 2021 Article 6526Eyal RobinsonNo ratings yet
- Pilot Study of A Model-Based Approach To Blood Glucose Control in Very-Low-Birthweight NeonatesDocument9 pagesPilot Study of A Model-Based Approach To Blood Glucose Control in Very-Low-Birthweight NeonatesMoch Rizki DestiantoroNo ratings yet
- Recent Advances in Endocrinology: Ambulatory Glucose Profile: Flash Glucose MonitoringDocument3 pagesRecent Advances in Endocrinology: Ambulatory Glucose Profile: Flash Glucose MonitoringShujian ZhaoNo ratings yet
- New Tech for Hypertension & Diabetes CareDocument3 pagesNew Tech for Hypertension & Diabetes CareLore Anne Mhae SantosNo ratings yet
- Canadian Journal of Diabetes: Special ArticleDocument8 pagesCanadian Journal of Diabetes: Special ArticleUsee TvNo ratings yet
- Zenopus ClassicDocument32 pagesZenopus Classicserenity42No ratings yet
- List of Students Allotted in Open Elective Subjects (B. Tech and M. Tech (Dual Degree) Integrated MSc. - 4th Semester - Regular - 2018 - 19) - 2 PDFDocument26 pagesList of Students Allotted in Open Elective Subjects (B. Tech and M. Tech (Dual Degree) Integrated MSc. - 4th Semester - Regular - 2018 - 19) - 2 PDFArpan JaiswalNo ratings yet
- Recycle ProgramDocument2 pagesRecycle ProgramKaps BlazeNo ratings yet
- Computational Models For Trunk Trajectory Planning and Load Distribution: A Test-Bed For Studying Various Clinical Adaptation and Motor Control Strategies of Low Back Pain PatientsDocument13 pagesComputational Models For Trunk Trajectory Planning and Load Distribution: A Test-Bed For Studying Various Clinical Adaptation and Motor Control Strategies of Low Back Pain PatientsOTorresGonzalezNo ratings yet
- Preliminary Evaluation On Vegetative of Rambutan (Nephelium Lappaceum) in Sandy Tin-Tailing SoilDocument7 pagesPreliminary Evaluation On Vegetative of Rambutan (Nephelium Lappaceum) in Sandy Tin-Tailing SoilAJAST JournalNo ratings yet
- IGCSE Biology 4325 2H Mark SchemeDocument14 pagesIGCSE Biology 4325 2H Mark SchememuhajireenNo ratings yet
- Spesifikasi Siemens MRI AERA 1,5 TDocument2 pagesSpesifikasi Siemens MRI AERA 1,5 TDr.gendjutNo ratings yet
- B Ed 3 Sem Physics Teaching Group C Science 1 Paper 1 Summer 2018Document3 pagesB Ed 3 Sem Physics Teaching Group C Science 1 Paper 1 Summer 2018Rrr KkkNo ratings yet
- FT Aeroterme GEADocument15 pagesFT Aeroterme GEACrisTimNo ratings yet
- Musical Siren Project Report Under 40 CharactersDocument10 pagesMusical Siren Project Report Under 40 Charactersvinod kapateNo ratings yet
- Astm D2467-2013Document8 pagesAstm D2467-2013Renato CorrêaNo ratings yet
- Time Rates ExplainedDocument6 pagesTime Rates ExplainedAljohn Escalona100% (1)
- XR5 9 Element 5 Band Yagi 20-17-15-12-10MDocument16 pagesXR5 9 Element 5 Band Yagi 20-17-15-12-10Msboonuy331No ratings yet
- CaseStudy AmtrakDocument14 pagesCaseStudy Amtraksnob_kNo ratings yet
- Plasma ChemistryDocument6 pagesPlasma ChemistryArief RomadhonNo ratings yet
- 11 - FORAGERS by Sam BoyerDocument106 pages11 - FORAGERS by Sam BoyerMurtaza HussainNo ratings yet
- VSD Power Supply Connections and EarthingDocument4 pagesVSD Power Supply Connections and EarthingHumaid ShaikhNo ratings yet
- HydrotherapyDocument7 pagesHydrotherapyGialys MoretaNo ratings yet
- Unit 4 Early HumansDocument8 pagesUnit 4 Early HumansSepfira ReztikaNo ratings yet
- Rules For The CertificationDocument84 pagesRules For The CertificationhdelriovNo ratings yet
- PMR205 DR Shawn BakerDocument31 pagesPMR205 DR Shawn Bakerspiridon_andrei2011No ratings yet
- General ALT Model For Step Stress TestDocument12 pagesGeneral ALT Model For Step Stress TestAnshul NautiyalNo ratings yet
- Proximity Sensing and Warning Technology For Heavy Construction Equipment OperationDocument10 pagesProximity Sensing and Warning Technology For Heavy Construction Equipment OperationAnand ReddyNo ratings yet
- Lecture No.3 Part 1 (Fan)Document6 pagesLecture No.3 Part 1 (Fan)Mohsen HassanNo ratings yet
- Experiment# 3 Projectile Motion (Tasks 3 and 4)Document18 pagesExperiment# 3 Projectile Motion (Tasks 3 and 4)Hafiz MuhammadNo ratings yet
- Reles, Fuentes, Etc. Catalogo - ABBDocument452 pagesReles, Fuentes, Etc. Catalogo - ABBmpica100% (1)
- Common Mistakes in Dimensional Calibration MethodsDocument16 pagesCommon Mistakes in Dimensional Calibration MethodssujudNo ratings yet
- Terpin Hydrate Oral SolutionDocument1 pageTerpin Hydrate Oral SolutionAbelard Maria EscrivaNo ratings yet
- General Description: Effective Distance Depends On Antenna, Tag and EnvironmentDocument2 pagesGeneral Description: Effective Distance Depends On Antenna, Tag and EnvironmentSHASHANK BHUSHANNo ratings yet