You might also like
- Continuous Glucose MonitoringFrom EverandContinuous Glucose MonitoringWeiping JiaNo ratings yet
- Biomedical Signal Processing and Control: Iftikhar Ahmad, Faysal Munir, Muhammad Faizan MunirDocument8 pagesBiomedical Signal Processing and Control: Iftikhar Ahmad, Faysal Munir, Muhammad Faizan MunirBrasoveanu GheorghitaNo ratings yet
- Artificial Pancreas - RAEE 2017 PDFDocument6 pagesArtificial Pancreas - RAEE 2017 PDFZeeshanNo ratings yet
- Insulin Control System For Diabetic Patients by Using Adaptive ControllerDocument6 pagesInsulin Control System For Diabetic Patients by Using Adaptive ControllerPreda ManuelaNo ratings yet
- Artificial Pancreas Technology Offers Hope For Childhood DiabetesDocument11 pagesArtificial Pancreas Technology Offers Hope For Childhood DiabetesDiana PeñalozaNo ratings yet
- A Fuzzy Controller For Blood Glucose-Insulin SysteDocument7 pagesA Fuzzy Controller For Blood Glucose-Insulin SysteBrasoveanu Gheorghita100% (1)
- Advancement in Insulcagon Pump Simulating As An Artificial Pancreas For The Treatment of DiabetesDocument5 pagesAdvancement in Insulcagon Pump Simulating As An Artificial Pancreas For The Treatment of Diabetesmosca90No ratings yet
- Divya 13Document20 pagesDivya 13Divya NadarNo ratings yet
- Research Article: Continuous Drug Infusion For Diabetes Therapy: A Closed-Loop Control System DesignDocument10 pagesResearch Article: Continuous Drug Infusion For Diabetes Therapy: A Closed-Loop Control System DesignBrasoveanu GheorghitaNo ratings yet
- Arquivos Brasileiros de Endocrinologia & MetabologiaDocument6 pagesArquivos Brasileiros de Endocrinologia & MetabologiaThenmozhi KaranNo ratings yet
- Time-Delay Model-Based Control of The Glucose-Insulin System, by Means of A State ObserverDocument16 pagesTime-Delay Model-Based Control of The Glucose-Insulin System, by Means of A State ObserverChanachai PuckNo ratings yet
- Run-to-Run Control of Blood Glucose Concentrations For People With Type 1 Diabetes MellitusDocument10 pagesRun-to-Run Control of Blood Glucose Concentrations For People With Type 1 Diabetes MellitusKamila Nanda RezkyNo ratings yet
- Apd T1DMDocument11 pagesApd T1DMmuhammad syafiqNo ratings yet
- Artificial Pancreas System For Type 1 Diabetes-Challenges and AdvancementsDocument12 pagesArtificial Pancreas System For Type 1 Diabetes-Challenges and Advancementsmuhammad syafiqNo ratings yet
- Closed Loop System Design For Wireless ArtificialDocument6 pagesClosed Loop System Design For Wireless ArtificialAmmar KhanNo ratings yet
- NIH Public Access: Author ManuscriptDocument19 pagesNIH Public Access: Author ManuscriptmilaNo ratings yet
- Study Guide Blood Glucose MonitoringDocument4 pagesStudy Guide Blood Glucose Monitoringjon elleNo ratings yet
- Study Guide Blood Glucose MonitoringDocument4 pagesStudy Guide Blood Glucose MonitoringDan Dan ManaoisNo ratings yet
- Artificial PancreasDocument2 pagesArtificial PancreasrameshjeyNo ratings yet
- Blood Glucose Regulation in Diabetics Using Sliding Mode Control TechniquesDocument14 pagesBlood Glucose Regulation in Diabetics Using Sliding Mode Control TechniquesTri RachmadijantoNo ratings yet
- Continuous Glucose Monitoring 508Document4 pagesContinuous Glucose Monitoring 508Hadi jameel HadiNo ratings yet
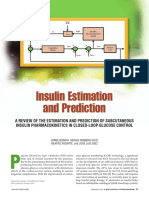
- Insulin Estimation and PredictionDocument20 pagesInsulin Estimation and PredictionLorenzo IraceNo ratings yet
- Sensors: Advanced Diabetes Management Using Artificial Intelligence and Continuous Glucose Monitoring SensorsDocument18 pagesSensors: Advanced Diabetes Management Using Artificial Intelligence and Continuous Glucose Monitoring SensorsShujian ZhaoNo ratings yet
- Novel Automatic Blood Glucose Level SensorDocument3 pagesNovel Automatic Blood Glucose Level Sensorsatishcoimbato12No ratings yet
- A VHDL Implementation of The Biostator IIDocument5 pagesA VHDL Implementation of The Biostator IImuhammad syafiqNo ratings yet
- Dia 2017 2525 AbstractsDocument134 pagesDia 2017 2525 AbstractsPranav Kumar Prabhakar100% (1)
- Robust PBPK/PD-Based Model PredictiveDocument13 pagesRobust PBPK/PD-Based Model PredictivenhatvpNo ratings yet
- Closed-Loop Insulin Delivery For Treatment of Type 1 DiabetesDocument9 pagesClosed-Loop Insulin Delivery For Treatment of Type 1 DiabetesPreda ManuelaNo ratings yet
- Thorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsDocument12 pagesThorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsgercampeNo ratings yet
- INS G Met InsulinDocument14 pagesINS G Met InsulinEndalk Berhanu AlemNo ratings yet
- Flash Glucose MonitoringDocument9 pagesFlash Glucose MonitoringAneed AnandNo ratings yet
- Journal Pone 0248280 PDFDocument17 pagesJournal Pone 0248280 PDFHafis KafitNo ratings yet
- Bomba de Infusión de Insulina 2017Document11 pagesBomba de Infusión de Insulina 2017Mijael HuarayoNo ratings yet
- Saint Paul University Philippines: Master of Science in NursingDocument15 pagesSaint Paul University Philippines: Master of Science in NursingGorgieNo ratings yet
- Saint Paul University Philippines: Master of Science in NursingDocument17 pagesSaint Paul University Philippines: Master of Science in NursingGorgieNo ratings yet
- Experience With The Continuous Glucose Monitoring System in A Medical Intensive Care UnitDocument10 pagesExperience With The Continuous Glucose Monitoring System in A Medical Intensive Care UnitjohnNo ratings yet
- ThesisChap1 3Document12 pagesThesisChap1 3Precious YasayNo ratings yet
- Automatic Blood Glucose RegulatorDocument5 pagesAutomatic Blood Glucose RegulatorIkekielNo ratings yet
- Artificial Pancreas Rpic2021Document4 pagesArtificial Pancreas Rpic2021guillermocochaNo ratings yet
- Irjet V7i6494 PDFDocument4 pagesIrjet V7i6494 PDFMohammed MuqsithNo ratings yet
- Jurnal Pemeriksaan Glukosa DarahDocument9 pagesJurnal Pemeriksaan Glukosa DarahIntan TafriNo ratings yet
- BMEN4110 Lab1 PartA Artificial Pancreas 2021Document15 pagesBMEN4110 Lab1 PartA Artificial Pancreas 2021William GoldbergNo ratings yet
- Protocolo YaleDocument7 pagesProtocolo Yalegiseladelarosa2006No ratings yet
- UNP-CN Do Not Reproduce: Learning Pocket DescriptionDocument14 pagesUNP-CN Do Not Reproduce: Learning Pocket DescriptionKathleen Joy PingenNo ratings yet
- Insulin Pump ProjectDocument15 pagesInsulin Pump ProjectAndrei Deac100% (1)
- LibreView Guide - Italian PaperDocument12 pagesLibreView Guide - Italian PaperJesus MuñozNo ratings yet
- Real Time Blood Sugar Monitoring: July 2017Document6 pagesReal Time Blood Sugar Monitoring: July 2017Khansa FadelseedNo ratings yet
- Digital Technology For DiabetesDocument11 pagesDigital Technology For Diabetesvvandv123No ratings yet
- Sensors: Current and Emerging Technology For Continuous Glucose MonitoringDocument19 pagesSensors: Current and Emerging Technology For Continuous Glucose MonitoringPulkit ShrivastavaNo ratings yet
- Marvin Et Al 2016 Minimization of Hypoglycemia As An Adverse Event During Insulin Infusion Further Refinement of TheDocument7 pagesMarvin Et Al 2016 Minimization of Hypoglycemia As An Adverse Event During Insulin Infusion Further Refinement of TheChanukya GvNo ratings yet
- Insulin Pumps and Sensors Cox PDFDocument42 pagesInsulin Pumps and Sensors Cox PDFDevang SNo ratings yet
- Measurement of Glucose Homeostasis in VivoDocument10 pagesMeasurement of Glucose Homeostasis in Vivo19400668No ratings yet
- A Bihormonal Closed-Loop Artificial Pancreas For Type 1 DiabetesDocument13 pagesA Bihormonal Closed-Loop Artificial Pancreas For Type 1 DiabetesMinhaz KhaledNo ratings yet
- Sampels IEEE Paper PDFDocument8 pagesSampels IEEE Paper PDFMiguel RebolloNo ratings yet
- Glucose Sensors CWDDocument83 pagesGlucose Sensors CWDJelenaNo ratings yet
- International Journal of Pharmaceutics: Lia Bally, Hood Thabit, Roman HovorkaDocument10 pagesInternational Journal of Pharmaceutics: Lia Bally, Hood Thabit, Roman HovorkaBrasoveanu GheorghitaNo ratings yet
- PosterDocument1 pagePosterSohel BaigNo ratings yet
- A Novel Needle-Injectable Millimeter Scale WirelesDocument12 pagesA Novel Needle-Injectable Millimeter Scale WirelesdiiinnaliinnnNo ratings yet
- Estimating The Cost-Effectiveness of Intermittently Scanned Continuous Glucose Monitoring in Adults With Type 1 Diabetes in EnglandDocument13 pagesEstimating The Cost-Effectiveness of Intermittently Scanned Continuous Glucose Monitoring in Adults With Type 1 Diabetes in EnglandlivtbuenoNo ratings yet
- CGM Comparison For People With Insulin Treated Research July 2023Document11 pagesCGM Comparison For People With Insulin Treated Research July 2023shahirahNo ratings yet
- Velocity Analysis of A DC Brushed Encoder MotorDocument8 pagesVelocity Analysis of A DC Brushed Encoder MotorBrasoveanu GheorghitaNo ratings yet
- Incremental Encoder Based Position and Speed Identification: Modeling and SimulationDocument13 pagesIncremental Encoder Based Position and Speed Identification: Modeling and SimulationmohdabdultalibNo ratings yet
- Implementing a simple PID controller without advanced mathDocument14 pagesImplementing a simple PID controller without advanced mathGiovanni Eliezer100% (2)
- DC Motor Speed Control SI PID Tuning PDFDocument4 pagesDC Motor Speed Control SI PID Tuning PDFvince kafuaNo ratings yet
- System Identification of A Hobby DC Motor Using A Low CostDocument6 pagesSystem Identification of A Hobby DC Motor Using A Low CostBrasoveanu GheorghitaNo ratings yet
- Control Practices Using Simulink With Arduino As Low Cost HardwareDocument6 pagesControl Practices Using Simulink With Arduino As Low Cost HardwareBrasoveanu GheorghitaNo ratings yet
- Petrella Et Al. - Speed Measurement Algorithms For Low-Resolution Incremental Encoder Equipped Drives - A Comparative Analysis PDFDocument8 pagesPetrella Et Al. - Speed Measurement Algorithms For Low-Resolution Incremental Encoder Equipped Drives - A Comparative Analysis PDFShahrin KamaruzamanNo ratings yet
- PI Controller For DC Motor Speed Realized With Arduino and SimulinkDocument6 pagesPI Controller For DC Motor Speed Realized With Arduino and SimulinkBrasoveanu GheorghitaNo ratings yet
- Realtime Parameter Estimation, Calibration and Simulation of A DC MotorDocument10 pagesRealtime Parameter Estimation, Calibration and Simulation of A DC MotorBrasoveanu GheorghitaNo ratings yet
- Design of PID Controller For DC Motor Speed Control Using Arduino MicrocontrollerDocument4 pagesDesign of PID Controller For DC Motor Speed Control Using Arduino MicrocontrollerBrasoveanu GheorghitaNo ratings yet
- MagPi - Beginners Guide v1Document244 pagesMagPi - Beginners Guide v1Benjamin Dover100% (4)
- Design of PID Controller For DC Motor Speed Control Using Arduino MicrocontrollerDocument4 pagesDesign of PID Controller For DC Motor Speed Control Using Arduino MicrocontrollerBrasoveanu GheorghitaNo ratings yet
- PID Plus Second Order Derivative ControllerDocument13 pagesPID Plus Second Order Derivative ControllerBrasoveanu GheorghitaNo ratings yet
- Model Based Design of Pid Controller For BLDC Motor With Implementation ofDocument8 pagesModel Based Design of Pid Controller For BLDC Motor With Implementation ofBrasoveanu GheorghitaNo ratings yet
- Advanced Drug Delivery Models for Medical ApplicationsDocument18 pagesAdvanced Drug Delivery Models for Medical ApplicationsBrasoveanu GheorghitaNo ratings yet
- Bootloader Design Application For EmbeddDocument6 pagesBootloader Design Application For EmbeddBrasoveanu GheorghitaNo ratings yet
- DC Motor Position Control using PID Controller with Friction CompensationDocument7 pagesDC Motor Position Control using PID Controller with Friction CompensationVipul SharmaNo ratings yet
- Modeling Glucose-Insulin Metabolism with Coupled ModelsDocument124 pagesModeling Glucose-Insulin Metabolism with Coupled ModelsBrasoveanu GheorghitaNo ratings yet
- Physiologic Evaluation of Controlling Glucose Tolerance Man: FactorsDocument12 pagesPhysiologic Evaluation of Controlling Glucose Tolerance Man: FactorsBrasoveanu GheorghitaNo ratings yet
- A Minimal Model For Glycemia Control in Critically Ill PatientsDocument4 pagesA Minimal Model For Glycemia Control in Critically Ill PatientsBrasoveanu GheorghitaNo ratings yet
- Sorensen 1978Document557 pagesSorensen 1978Brasoveanu GheorghitaNo ratings yet
- Nath 2016Document11 pagesNath 2016Brasoveanu GheorghitaNo ratings yet
- Fuzzy Model-Based Controller For Blood Glucose Control in Type 1 Diabetes: An LMI ApproachDocument27 pagesFuzzy Model-Based Controller For Blood Glucose Control in Type 1 Diabetes: An LMI ApproachBrasoveanu GheorghitaNo ratings yet
- Cgmquantify Python and R Packages For ComprehensivDocument10 pagesCgmquantify Python and R Packages For ComprehensivBrasoveanu GheorghitaNo ratings yet
- Sveshnikova 2017 PDFDocument6 pagesSveshnikova 2017 PDFBrasoveanu GheorghitaNo ratings yet
- Design and Implementation of Ball and Plate Control System Using Pid ControllerDocument65 pagesDesign and Implementation of Ball and Plate Control System Using Pid ControllerRay Kevin CardenasNo ratings yet
- Modeling Glucose-Insulin Metabolism with Coupled ModelsDocument124 pagesModeling Glucose-Insulin Metabolism with Coupled ModelsBrasoveanu GheorghitaNo ratings yet
- Short Discussion/Essay - Automation, Autonomy, and Semi-Autonomy: A Brief Definition Relative To Robotics and Machine SystemsDocument4 pagesShort Discussion/Essay - Automation, Autonomy, and Semi-Autonomy: A Brief Definition Relative To Robotics and Machine SystemsBrasoveanu GheorghitaNo ratings yet
- Lac NL - Spring 2021Document8 pagesLac NL - Spring 2021Ghassan NajmNo ratings yet
- MAPEH Daily Lesson LogDocument11 pagesMAPEH Daily Lesson LogMARTIN YUI LOPEZNo ratings yet
- ItDocument4 pagesItNguyễn Duy HuânNo ratings yet
- The Relationship Between Lower Intelligence Crime and Custodial Outcomes A Brief Literary Review of A Vulnerable GroupDocument16 pagesThe Relationship Between Lower Intelligence Crime and Custodial Outcomes A Brief Literary Review of A Vulnerable GroupSteveNo ratings yet
- (Lecture 2) Skin TestDocument31 pages(Lecture 2) Skin TestShubham KadiwalaNo ratings yet
- Health Promoting Behaviour Among Secondary School Children With Respect To GenderDocument5 pagesHealth Promoting Behaviour Among Secondary School Children With Respect To GenderAnonymous CwJeBCAXpNo ratings yet
- This Study Determined The Effectiveness of Mnemonics in Improving Memory Among Nursing Students in GCON, BikanerDocument3 pagesThis Study Determined The Effectiveness of Mnemonics in Improving Memory Among Nursing Students in GCON, BikanerNaveen ShrivasNo ratings yet
- Vitamins Minerals: Composition & Therapeutic UseDocument2 pagesVitamins Minerals: Composition & Therapeutic UseNouman AbbasNo ratings yet
- Health and Environmental Impacts of Cleaning AgentsDocument8 pagesHealth and Environmental Impacts of Cleaning AgentsZafira Nurul FizaNo ratings yet
- Amit Surati 29Document3 pagesAmit Surati 29api-286592025No ratings yet
- Townsend 1979Document28 pagesTownsend 1979api-534238122No ratings yet
- Optometry SeniorDocument8 pagesOptometry Seniorapi-504989033No ratings yet
- Directory 18-08-21Document34 pagesDirectory 18-08-21api-309412486100% (1)
- Get Shredded PDFDocument40 pagesGet Shredded PDFLisandro Cacciatore100% (3)
- Biology 2 Macromolecules and NutrientsDocument16 pagesBiology 2 Macromolecules and NutrientsMwendalubi ChiholyongaNo ratings yet
- Yahoo News You Gov Health Poll 3.11.24Document13 pagesYahoo News You Gov Health Poll 3.11.24AndrewNo ratings yet
- Fatigue Management Report Template-CompletedDocument4 pagesFatigue Management Report Template-CompletedAbdullah100% (1)
- ADEC - Al Murooj Scientific Private School 2015 2016Document16 pagesADEC - Al Murooj Scientific Private School 2015 2016Edarabia.comNo ratings yet
- JR NeuroanestesiDocument11 pagesJR Neuroanestesiliashuban29No ratings yet
- Occlusal Plane Template TechniqueDocument39 pagesOcclusal Plane Template TechniqueREWA KAWADENo ratings yet
- Emotional Loneliness First Aid by SlidesgoDocument58 pagesEmotional Loneliness First Aid by SlidesgoKarin FauziahNo ratings yet
- Action Insulin Name Effective Considerations Onset Peak DurationDocument2 pagesAction Insulin Name Effective Considerations Onset Peak DurationDr. Ricardo R.V. de BritoNo ratings yet
- Consultant Schedule Artwork Updated For August 2023Document3 pagesConsultant Schedule Artwork Updated For August 2023RLV TRADINGNo ratings yet
- Teenage Pregnancy Refers To The Adolescent Girls, Usually With in The AgesDocument6 pagesTeenage Pregnancy Refers To The Adolescent Girls, Usually With in The Agesmarina abanNo ratings yet
- Immuno GlowDocument11 pagesImmuno GlowNoly ClaveringNo ratings yet
- Decision MakingDocument19 pagesDecision MakingJeph ToholNo ratings yet
- Re-Opening Plan For The 2020-2021 School YearDocument18 pagesRe-Opening Plan For The 2020-2021 School YearNews 8 WROCNo ratings yet
- Six Major Schools of Thought in PsychologyDocument2 pagesSix Major Schools of Thought in PsychologyAnonymous 4qEPpyx100% (1)
- A Quick Guide For Busy Parents: Connect and Re-Direct Name It To Tame ItDocument1 pageA Quick Guide For Busy Parents: Connect and Re-Direct Name It To Tame ItSanjeev Sharma100% (2)
- Long-Term Abstinence Following Holotropic Breathwork As Adjunctive Treatment of Substance Use Disorders and Related Psychiatric ComorbidityDocument7 pagesLong-Term Abstinence Following Holotropic Breathwork As Adjunctive Treatment of Substance Use Disorders and Related Psychiatric ComorbiditymghuesoNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)