You might also like
- Continuous Glucose MonitoringFrom EverandContinuous Glucose MonitoringWeiping JiaNo ratings yet
- Divya 13Document20 pagesDivya 13Divya NadarNo ratings yet
- Paper 2 HighlightedDocument9 pagesPaper 2 HighlightedVaishnavi YacheNo ratings yet
- Apd T1DMDocument11 pagesApd T1DMmuhammad syafiqNo ratings yet
- Artificial Pancreas - RAEE 2017 PDFDocument6 pagesArtificial Pancreas - RAEE 2017 PDFZeeshanNo ratings yet
- Run-to-Run Control of Blood Glucose Concentrations For People With Type 1 Diabetes MellitusDocument10 pagesRun-to-Run Control of Blood Glucose Concentrations For People With Type 1 Diabetes MellitusKamila Nanda RezkyNo ratings yet
- Artificial Pancreas Technology Offers Hope For Childhood DiabetesDocument11 pagesArtificial Pancreas Technology Offers Hope For Childhood DiabetesDiana PeñalozaNo ratings yet
- NIH Public Access: Author ManuscriptDocument19 pagesNIH Public Access: Author ManuscriptmilaNo ratings yet
- RM ProtocolDocument4 pagesRM Protocolcifha diasNo ratings yet
- Simplified Mathematical Model of Glucose-Insulin SystemDocument12 pagesSimplified Mathematical Model of Glucose-Insulin SystemBrasoveanu GheorghitaNo ratings yet
- Time-Delay Model-Based Control of The Glucose-Insulin System, by Means of A State ObserverDocument16 pagesTime-Delay Model-Based Control of The Glucose-Insulin System, by Means of A State ObserverChanachai PuckNo ratings yet
- Closed-Loop Insulin Delivery For Treatment of Type 1 DiabetesDocument9 pagesClosed-Loop Insulin Delivery For Treatment of Type 1 DiabetesPreda ManuelaNo ratings yet
- tmp22D3 TMPDocument9 pagestmp22D3 TMPFrontiersNo ratings yet
- Thorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsDocument12 pagesThorough Testing of Predictive Functional Control On A Well Validated in Silico Model of Type I Diabetic PatientsgercampeNo ratings yet
- Insulin Control System For Diabetic Patients by Using Adaptive ControllerDocument6 pagesInsulin Control System For Diabetic Patients by Using Adaptive ControllerPreda ManuelaNo ratings yet
- Biomedical Signal Processing and Control: Iftikhar Ahmad, Faysal Munir, Muhammad Faizan MunirDocument8 pagesBiomedical Signal Processing and Control: Iftikhar Ahmad, Faysal Munir, Muhammad Faizan MunirBrasoveanu GheorghitaNo ratings yet
- A Fuzzy Controller For Blood Glucose-Insulin SysteDocument7 pagesA Fuzzy Controller For Blood Glucose-Insulin SysteBrasoveanu Gheorghita100% (1)
- ISPAD Clinical Practice Consensus Guidelines 2018: Exercise in Children and Adolescents With DiabetesDocument22 pagesISPAD Clinical Practice Consensus Guidelines 2018: Exercise in Children and Adolescents With Diabetesdesak indryNo ratings yet
- Theoretical Biology and Medical Modelling: A Discrete Single Delay Model For The Intra-Venous Glucose Tolerance TestDocument16 pagesTheoretical Biology and Medical Modelling: A Discrete Single Delay Model For The Intra-Venous Glucose Tolerance TestRocsana Teodora MăriuNo ratings yet
- Modeling of Pancreatic System And: Diabetes Mellitus Type 1Document3 pagesModeling of Pancreatic System And: Diabetes Mellitus Type 1Nelcytaa MuñozNo ratings yet
- Original ArticleDocument10 pagesOriginal ArticlegistaluvikaNo ratings yet
- Robust PBPK/PD-Based Model PredictiveDocument13 pagesRobust PBPK/PD-Based Model PredictivenhatvpNo ratings yet
- Research Article: Continuous Drug Infusion For Diabetes Therapy: A Closed-Loop Control System DesignDocument10 pagesResearch Article: Continuous Drug Infusion For Diabetes Therapy: A Closed-Loop Control System DesignBrasoveanu GheorghitaNo ratings yet
- Comparative Analysis of PID Tuning Techniques For Blood Glucose Level of Diabetic PatientDocument6 pagesComparative Analysis of PID Tuning Techniques For Blood Glucose Level of Diabetic Patient015Maulana Malik IbrahimNo ratings yet
- Zhou2019 Article InsulinDegludecANovelUltra-LonDocument18 pagesZhou2019 Article InsulinDegludecANovelUltra-LonmehakNo ratings yet
- Blood Glucose Regulation in Diabetics Using Sliding Mode Control TechniquesDocument14 pagesBlood Glucose Regulation in Diabetics Using Sliding Mode Control TechniquesTri RachmadijantoNo ratings yet
- A Mathematical Model of Glucose - Insulin Regulation Under The Influence of Externally Ingested Glucose (G-I-E Model)Document5 pagesA Mathematical Model of Glucose - Insulin Regulation Under The Influence of Externally Ingested Glucose (G-I-E Model)inventionjournalsNo ratings yet
- Diabetes Research and Clinical Practice Volume Issue 2018Document37 pagesDiabetes Research and Clinical Practice Volume Issue 2018yayan_adiutama98No ratings yet
- Changes of Insulin Sensitivity and Secretion After Bariatric Metabolic SurgeryDocument7 pagesChanges of Insulin Sensitivity and Secretion After Bariatric Metabolic SurgeryfrandellionNo ratings yet
- Closed Loop System Design For Wireless ArtificialDocument6 pagesClosed Loop System Design For Wireless ArtificialAmmar KhanNo ratings yet
- Study Guide Blood Glucose MonitoringDocument4 pagesStudy Guide Blood Glucose Monitoringjon elleNo ratings yet
- Study Guide Blood Glucose MonitoringDocument4 pagesStudy Guide Blood Glucose MonitoringDan Dan ManaoisNo ratings yet
- Pilot Study of A Model-Based Approach To Blood Glucose Control in Very-Low-Birthweight NeonatesDocument9 pagesPilot Study of A Model-Based Approach To Blood Glucose Control in Very-Low-Birthweight NeonatesMoch Rizki DestiantoroNo ratings yet
- Continuous Glucose Profiles in Healthy Subjects Under Everyday Life Conditions and After Different MealsDocument9 pagesContinuous Glucose Profiles in Healthy Subjects Under Everyday Life Conditions and After Different MealsAsose TuNo ratings yet
- Artificial Pancreas System For Type 1 Diabetes-Challenges and AdvancementsDocument12 pagesArtificial Pancreas System For Type 1 Diabetes-Challenges and Advancementsmuhammad syafiqNo ratings yet
- Protocolo YaleDocument7 pagesProtocolo Yalegiseladelarosa2006No ratings yet
- Medication-Free Management Oftype 2 Diabetesmellitus: Empirical and Modeling-Based Case StudyDocument25 pagesMedication-Free Management Oftype 2 Diabetesmellitus: Empirical and Modeling-Based Case StudyIJAR JOURNALNo ratings yet
- Artificial PancreasDocument2 pagesArtificial PancreasrameshjeyNo ratings yet
- 2018 Timing of Exercise Affects Glycemic Control in Type 2 DiabetesDocument9 pages2018 Timing of Exercise Affects Glycemic Control in Type 2 DiabetesdilloniarbzNo ratings yet
- Dosage Planning For Diabetes Patients Using Data Mining MethodsDocument7 pagesDosage Planning For Diabetes Patients Using Data Mining MethodsTajju TajammulNo ratings yet
- Paper 3Document7 pagesPaper 3Vaishnavi YacheNo ratings yet
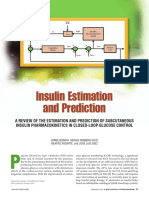
- Insulin Estimation and PredictionDocument20 pagesInsulin Estimation and PredictionLorenzo IraceNo ratings yet
- Research Article: Acute Whole Body Vibration Decreases The Glucose Levels in Elderly Diabetic WomenDocument8 pagesResearch Article: Acute Whole Body Vibration Decreases The Glucose Levels in Elderly Diabetic WomenStefanny AmahorsejaNo ratings yet
- iDECIDE: A Mobile Application For Insulin Dosing Using An Evidence Based Equation To Account For Patient PreferencesDocument1 pageiDECIDE: A Mobile Application For Insulin Dosing Using An Evidence Based Equation To Account For Patient PreferencesPedroMartinsNo ratings yet
- Exercise in Type 2 Diabetes: To Resist or To Endure?: CommentaryDocument5 pagesExercise in Type 2 Diabetes: To Resist or To Endure?: CommentarySabdiah Eka SariNo ratings yet
- Nejmoa 2111673Document11 pagesNejmoa 2111673Vincent OsorioNo ratings yet
- Dia 2017 2525 AbstractsDocument134 pagesDia 2017 2525 AbstractsPranav Kumar Prabhakar100% (1)
- Artificial Intelligence in Medicine: Virginie Felizardo, Nuno M. Garcia, Nuno Pombo, Imen MegdicheDocument15 pagesArtificial Intelligence in Medicine: Virginie Felizardo, Nuno M. Garcia, Nuno Pombo, Imen MegdicheShujian ZhaoNo ratings yet
- Paper 1 HighlightedDocument7 pagesPaper 1 HighlightedVaishnavi YacheNo ratings yet
- Sensors 20 01705Document11 pagesSensors 20 01705QSilvaNo ratings yet
- Defining Insulin Resistance From Hyperinsulinemic-Euglycemic ClampsDocument6 pagesDefining Insulin Resistance From Hyperinsulinemic-Euglycemic ClampsNanda Rizky FathiyaNo ratings yet
- Low-Volume High-Intensity Interval Training Reduces Hyperglycemia and Increases Muscle Mitochondrial Capacity in Patients With Type 2 DiabetesDocument7 pagesLow-Volume High-Intensity Interval Training Reduces Hyperglycemia and Increases Muscle Mitochondrial Capacity in Patients With Type 2 DiabetesSafira Ridha UlyaNo ratings yet
- BMC Endocrine DisordersDocument8 pagesBMC Endocrine DisordersJose Luis JaimeNo ratings yet
- Journal of Diabetes and Its ComplicationsDocument7 pagesJournal of Diabetes and Its ComplicationsSinta AgustinaNo ratings yet
- Acute and 2 Week Exposure To PrednisolonDocument7 pagesAcute and 2 Week Exposure To PrednisolonRamadhan Yudha PratamaNo ratings yet
- Continuous Glucose Monitoring Devices For Patients With Diabeles Mellitus On InsulinDocument25 pagesContinuous Glucose Monitoring Devices For Patients With Diabeles Mellitus On InsulinCalifornia Technology Assessment ForumNo ratings yet
- Pediatric DiabeticDocument9 pagesPediatric Diabeticperla islasNo ratings yet
- A Bihormonal Closed-Loop Artificial Pancreas For Type 1 DiabetesDocument13 pagesA Bihormonal Closed-Loop Artificial Pancreas For Type 1 DiabetesMinhaz KhaledNo ratings yet
- Artigo 1Document7 pagesArtigo 1Maria LeonorNo ratings yet
- Palumbo 13Document13 pagesPalumbo 13Margarete Ap SantosNo ratings yet
- (EAAP Scientific Series) Lapierre, Hélène - Skomiał, Jacek - Energy and Protein Metabolism and Nutrition 2016-Wageningen Academic Publishers (2016)Document385 pages(EAAP Scientific Series) Lapierre, Hélène - Skomiał, Jacek - Energy and Protein Metabolism and Nutrition 2016-Wageningen Academic Publishers (2016)Juni ClaudiaNo ratings yet
- BSL Carbohydrates Lab ManualDocument9 pagesBSL Carbohydrates Lab ManualHera VictrixNo ratings yet
- Nutrition and diabetes information for studentDocument2 pagesNutrition and diabetes information for studentNova Novitarini100% (1)
- Diabetes Mellitus: David B. Sacks, M.B., CH.B., F.R.C.PathDocument42 pagesDiabetes Mellitus: David B. Sacks, M.B., CH.B., F.R.C.PathAdhia DekaNo ratings yet
- Insulin Injection PDFDocument6 pagesInsulin Injection PDFAulia mulidaNo ratings yet
- The 6 Stages of Diabetes Control & ReversalDocument7 pagesThe 6 Stages of Diabetes Control & ReversalHaleelu Abdul JaleelNo ratings yet
- Pancreas Anatomy & Physiology ExplainedDocument35 pagesPancreas Anatomy & Physiology Explainedpedros43No ratings yet
- Literature Review On Diabetes Mellitus Type 2Document4 pagesLiterature Review On Diabetes Mellitus Type 2qtbghsbnd100% (1)
- CarbohydratesDocument41 pagesCarbohydratesStrange Me100% (3)
- Diabetes Case StudyDocument9 pagesDiabetes Case Studyapi-346620455No ratings yet
- Insulin and IncretinsDocument6 pagesInsulin and IncretinspykkoNo ratings yet
- Diabetes Mellitus Surgical PatientDocument33 pagesDiabetes Mellitus Surgical PatientGerald AndersonNo ratings yet
- The Effect of Cinnamon On Glucose of Type II Diabetes PatientsDocument7 pagesThe Effect of Cinnamon On Glucose of Type II Diabetes PatientsMelinda Fila BethaNo ratings yet
- H H H H H M M M M M: Ormone Ormone Ormone Ormone Ormone ET ET ET ET Etabolism Abolism Abolism Abolism AbolismDocument28 pagesH H H H H M M M M M: Ormone Ormone Ormone Ormone Ormone ET ET ET ET Etabolism Abolism Abolism Abolism AbolismHoth HothNo ratings yet
- Pharma For StudentsDocument23 pagesPharma For StudentsDominic Reambonanza0% (1)
- Lethargic Weakness Decreased Performance: Nursing Care PlanDocument2 pagesLethargic Weakness Decreased Performance: Nursing Care PlanZhayree R.No ratings yet
- Case Study DiabetesDocument15 pagesCase Study DiabetessamanNo ratings yet
- Cactus (Opuntia Ficus-Indica) : A Review On Its Antioxidants Properties and Potential Pharmacological Use in Chronic DiseasesDocument9 pagesCactus (Opuntia Ficus-Indica) : A Review On Its Antioxidants Properties and Potential Pharmacological Use in Chronic DiseasesAidNo ratings yet
- Chapter - 011 - PressmannDocument46 pagesChapter - 011 - Pressmannrohan pandyaNo ratings yet
- Diabetes AACE 2016Document30 pagesDiabetes AACE 2016Μιχάλης ΤερζάκηςNo ratings yet
- Xu 2018Document12 pagesXu 2018adNo ratings yet
- Carbohydrate's Role in Fat Loss: by Cameron L. Martz, ACSM H/FIDocument5 pagesCarbohydrate's Role in Fat Loss: by Cameron L. Martz, ACSM H/FIAnonymous 5mSMeP2jNo ratings yet
- Benefits of Yoga From HEAD To TOE (Based On Scientific Research)Document38 pagesBenefits of Yoga From HEAD To TOE (Based On Scientific Research)Ajay LochunNo ratings yet
- MS EndoDocument22 pagesMS EndoFrechel Ann Landingin PedrozoNo ratings yet
- ChankoDocument9 pagesChankoPauloCarvalhoNo ratings yet
- Lesson Preview: Checking For UnderstandingDocument2 pagesLesson Preview: Checking For UnderstandingKristinelou Marie N. ReynaNo ratings yet
- Method Development and Validation For The Simultaneous Estimation of Sitagliptin and Metformin by HPLC and Uv-Spectroscopy MethodsDocument116 pagesMethod Development and Validation For The Simultaneous Estimation of Sitagliptin and Metformin by HPLC and Uv-Spectroscopy MethodsNaveen MadirajuNo ratings yet
- JBDS RenalGuideAbbreviated 2016Document26 pagesJBDS RenalGuideAbbreviated 2016Majid KhanNo ratings yet
- Hypoglycemia in Diabetes: P E. C, S N. D, H SDocument11 pagesHypoglycemia in Diabetes: P E. C, S N. D, H SFabio FabbriNo ratings yet
- GlycogenDocument25 pagesGlycogencandysunNo ratings yet
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 5 out of 5 stars5/5 (1)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingFrom EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingRating: 5 out of 5 stars5/5 (59)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Hungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthFrom EverandHungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthRating: 4 out of 5 stars4/5 (7)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthFrom EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthRating: 5 out of 5 stars5/5 (37)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainFrom EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainRating: 3.5 out of 5 stars3.5/5 (6)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- The Complete Beck Diet for Life: The 5-Stage Program for Permanent Weight LossFrom EverandThe Complete Beck Diet for Life: The 5-Stage Program for Permanent Weight LossRating: 3.5 out of 5 stars3.5/5 (6)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItFrom EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItRating: 4.5 out of 5 stars4.5/5 (19)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- Foods That Cause You to Lose Weight: The Negative Calorie EffectFrom EverandFoods That Cause You to Lose Weight: The Negative Calorie EffectRating: 3 out of 5 stars3/5 (5)
- The Ultimate Volumetrics Diet: Smart, Simple, Science-Based Strategies for Losing Weight and Keeping It OffFrom EverandThe Ultimate Volumetrics Diet: Smart, Simple, Science-Based Strategies for Losing Weight and Keeping It OffNo ratings yet
- The Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondFrom EverandThe Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondRating: 4.5 out of 5 stars4.5/5 (28)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)