You might also like
- Glorified FastingDocument71 pagesGlorified FastingEugene Yeboah100% (18)
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- John PFTDocument231 pagesJohn PFTAlexander Santiago ParelNo ratings yet
- Cardiovascular System: Presented byDocument76 pagesCardiovascular System: Presented bySoma Al-mutairiNo ratings yet
- Nurse Healer Script PackageDocument20 pagesNurse Healer Script PackageLuca Baroni100% (1)
- Ventilator Wave Form and InterpretationDocument59 pagesVentilator Wave Form and InterpretationArnab SitNo ratings yet
- Animal Transport - IGCSE Biology Notes (2020)Document14 pagesAnimal Transport - IGCSE Biology Notes (2020)Zhi En LeeNo ratings yet
- Congestive Heart Failure PathophysiologyDocument16 pagesCongestive Heart Failure PathophysiologyDale LaurenteNo ratings yet
- A&P Cardiovascular System PowerPoint (Nursing)Document34 pagesA&P Cardiovascular System PowerPoint (Nursing)Linsey Bowen67% (6)
- Pulmonary EdemaDocument10 pagesPulmonary EdemaNader Smadi100% (6)
- Correct answers for Filipino VI ReviewerDocument22 pagesCorrect answers for Filipino VI ReviewerYamSiriOdarnohNo ratings yet
- Chapter 14 - Overview of The CirculationDocument26 pagesChapter 14 - Overview of The Circulationmuna sNo ratings yet
- Anatomy and Physiology Science Olympiad 2024 Cheat SheetDocument3 pagesAnatomy and Physiology Science Olympiad 2024 Cheat Sheetgfzmrtqj54No ratings yet
- Blood Circulation and TransportDocument15 pagesBlood Circulation and TransportSENSNo ratings yet
- Science 9 TG Draft 4.29.2014Document406 pagesScience 9 TG Draft 4.29.2014astherielleNo ratings yet
- Pulmonary Hypertension: Causes, Symptoms, Diagnosis & TreatmentDocument3 pagesPulmonary Hypertension: Causes, Symptoms, Diagnosis & TreatmentJiezl Abellano AfinidadNo ratings yet
- Therapeutic Dosing GuideDocument37 pagesTherapeutic Dosing GuideLuis Elijah De CastroNo ratings yet
- HY SystemsDocument720 pagesHY SystemsYassandra CalderónNo ratings yet
- Pulmonary Embolism Guide: Causes, Symptoms & DiagnosisDocument60 pagesPulmonary Embolism Guide: Causes, Symptoms & DiagnosisRafika RaraNo ratings yet
- Manage and Diagnose Acute and Chronic Cor PulmonaleDocument42 pagesManage and Diagnose Acute and Chronic Cor PulmonaleNym Angga SantosaNo ratings yet
- Nursing Care of CHF PatientsDocument25 pagesNursing Care of CHF PatientsIrwan100% (2)
- PedsnotesDocument18 pagesPedsnoteskp13oyNo ratings yet
- Kuliah 16 Cor PulmonaleDocument41 pagesKuliah 16 Cor PulmonalecaturwiraNo ratings yet
- Pulmonary Hypertension: Causes, Symptoms, Diagnosis and TreatmentDocument10 pagesPulmonary Hypertension: Causes, Symptoms, Diagnosis and TreatmentCkaye GansubinNo ratings yet
- Test Banks Gary PersingDocument35 pagesTest Banks Gary PersingAlexander Santiago ParelNo ratings yet
- WGA6-Ocular Blood Flow in GlaucomaDocument177 pagesWGA6-Ocular Blood Flow in Glaucomamdmmm100% (1)
- 1905 January 2018 ENCS - Corrected PDFDocument3 pages1905 January 2018 ENCS - Corrected PDFJoseph Jr TengayNo ratings yet
- Thesis Manuscript - UIGANDocument110 pagesThesis Manuscript - UIGANAlexander Santiago Parel100% (1)
- Thesis Manuscript - UIGANDocument110 pagesThesis Manuscript - UIGANAlexander Santiago Parel100% (1)
- Under Supervision DR/ Mariam Sabry: Ulmonary DemaDocument28 pagesUnder Supervision DR/ Mariam Sabry: Ulmonary DemaMohamed ElsyaedNo ratings yet
- NSG 117 PerfusionDocument55 pagesNSG 117 PerfusionAnonymous UJEyEsNo ratings yet
- Pulmonary Hypertension: An Overview of Causes, Symptoms and DiagnosisDocument40 pagesPulmonary Hypertension: An Overview of Causes, Symptoms and DiagnosisAlexander Santiago ParelNo ratings yet
- Pulmonary HypertensionDocument9 pagesPulmonary HypertensionDesriani Anisa YakubNo ratings yet
- Case Study PPT Patho NLNGDocument36 pagesCase Study PPT Patho NLNGKate ChavezNo ratings yet
- Cor PulmonaleDocument3 pagesCor PulmonaleKhalid Mahmud ArifinNo ratings yet
- Pulmonary Heart Disease Causes Right Ventricle EnlargementDocument24 pagesPulmonary Heart Disease Causes Right Ventricle EnlargementGungdeprawira NegaraNo ratings yet
- Noncommunicable DiseasesDocument22 pagesNoncommunicable DiseasesChintiya PutriNo ratings yet
- Pulmonary Edema: Causes, Symptoms and Treatment of 'Water in the LungsDocument23 pagesPulmonary Edema: Causes, Symptoms and Treatment of 'Water in the LungsLouella RamosNo ratings yet
- Pulmonary Hypertension GuideDocument9 pagesPulmonary Hypertension GuideChryst Louise SaavedraNo ratings yet
- MedSurg 2Document69 pagesMedSurg 2Claire Maurice JuaneroNo ratings yet
- Pulmonary EdemaaDocument17 pagesPulmonary EdemaaSoma Al-mutairiNo ratings yet
- CHF Left SidedDocument21 pagesCHF Left SidedSandie Daniel GabalunosNo ratings yet
- Pulmonary Vascular DiseaseDocument4 pagesPulmonary Vascular DiseaseSaima JabbarNo ratings yet
- Cardiogenic ShockDocument32 pagesCardiogenic ShockDiksha dudiNo ratings yet
- LME SelfDocument5 pagesLME SelfJM Mizraime Gallo Dela-peñaNo ratings yet
- Cor Pulmonale: Right Heart Failure Due to Lung DiseaseDocument62 pagesCor Pulmonale: Right Heart Failure Due to Lung DiseaseAlbert NixonNo ratings yet
- MEDICAL PATHOLOGIES - CardiovascularDocument6 pagesMEDICAL PATHOLOGIES - Cardiovascularngachangong victorineNo ratings yet
- Cor PulmonaleDocument27 pagesCor PulmonaleumapathisivanNo ratings yet
- Heart Failure & Hypertension Clinical ImpressionDocument5 pagesHeart Failure & Hypertension Clinical ImpressionGwendolyn Talahiban LusaraNo ratings yet
- Myocardial InfarctionDocument15 pagesMyocardial InfarctionameerNo ratings yet
- Samara University: Collage of Biomedical and Health Science Department of Public Health OfficerDocument32 pagesSamara University: Collage of Biomedical and Health Science Department of Public Health Officergirma melakuNo ratings yet
- Val 25-6dec11p5 PDFDocument1 pageVal 25-6dec11p5 PDFAzura ZahraNo ratings yet
- Biologic Crisis: Pathophysiology of Cardiac, Respiratory, Renal FailuresDocument64 pagesBiologic Crisis: Pathophysiology of Cardiac, Respiratory, Renal FailuresDonna Solamo TalabocNo ratings yet
- HY SurgeryDocument283 pagesHY SurgerytejNo ratings yet
- Acute Interstitial Pulmonary Edema Power Point FixDocument29 pagesAcute Interstitial Pulmonary Edema Power Point FixnandablaguNo ratings yet
- Pulmonary Edema: Fluid in the LungsDocument15 pagesPulmonary Edema: Fluid in the LungsKevin PatelNo ratings yet
- Pulmonary EdemaDocument20 pagesPulmonary EdemaMohmmad Lateef GanieNo ratings yet
- Cardiovascular System Dr. Eman Badr 2020Document182 pagesCardiovascular System Dr. Eman Badr 2020Amina DinarNo ratings yet
- Anatomy and PhysiologyDocument3 pagesAnatomy and PhysiologyKobe ManuelNo ratings yet
- COPD and Pulmonary Hypertension Cause Right Heart FailureDocument19 pagesCOPD and Pulmonary Hypertension Cause Right Heart FailureIka Lukita SariNo ratings yet
- Pulmonary Hypertension GuideDocument8 pagesPulmonary Hypertension Guidemerin sunilNo ratings yet
- Sclerodactyly, and Telangiectasis) Syndrome Accompany-: Cor PulmonaleDocument2 pagesSclerodactyly, and Telangiectasis) Syndrome Accompany-: Cor PulmonaledivinaNo ratings yet
- CARDIAC FAILURE NewDocument60 pagesCARDIAC FAILURE NewJake MillerNo ratings yet
- NCM 118 - Emphsyema Pulmonary Embolism ARDS ALI VAP and Respiratory FailureDocument30 pagesNCM 118 - Emphsyema Pulmonary Embolism ARDS ALI VAP and Respiratory Failurecabelin randy amenNo ratings yet
- CHFSP 2005Document36 pagesCHFSP 2005Andy F MonroeNo ratings yet
- Clinical Symptoms Due To Fluid CongestionDocument6 pagesClinical Symptoms Due To Fluid CongestionedenpearlcastilloNo ratings yet
- Introduction to Cor Pulmonale: Causes, Symptoms, and DiagnosisDocument15 pagesIntroduction to Cor Pulmonale: Causes, Symptoms, and DiagnosisRizky Zulfa Afrida100% (1)
- CorpulmonalefinalDocument37 pagesCorpulmonalefinalRay ReyesNo ratings yet
- GCS neuro scale and heart failure symptomsDocument7 pagesGCS neuro scale and heart failure symptomsGirlie TeruelNo ratings yet
- Understanding Corpulmonale: Causes, Symptoms and TreatmentDocument17 pagesUnderstanding Corpulmonale: Causes, Symptoms and TreatmentSurya ArhNo ratings yet
- Respiratory System DiseasesDocument6 pagesRespiratory System DiseasesWheya OliverosNo ratings yet
- Cardio Lecture Notes: Congestive Heart FailureDocument7 pagesCardio Lecture Notes: Congestive Heart Failurecolek22100% (5)
- Cor Pulmonal and CHDDocument44 pagesCor Pulmonal and CHDamir iksanNo ratings yet
- CHF Case Study (Document35 pagesCHF Case Study (EzraManzanoNo ratings yet
- Ratheesh R.LDocument23 pagesRatheesh R.LvaishnaviNo ratings yet
- Congenital Heart DiseaseDocument38 pagesCongenital Heart DiseaseSnIP StandredNo ratings yet
- Cor Pulmonale PresentationDocument17 pagesCor Pulmonale Presentationandi reskifaisNo ratings yet
- Shortness of Breath #2 NotesDocument4 pagesShortness of Breath #2 NotesChananNo ratings yet
- Printable Water Color Quote BookmarksDocument1 pagePrintable Water Color Quote BookmarksAlexander Santiago ParelNo ratings yet
- I. Matching Type (15 PTS.)Document3 pagesI. Matching Type (15 PTS.)Alexander Santiago ParelNo ratings yet
- Leads Electrodes Placement Views FunctionDocument1 pageLeads Electrodes Placement Views FunctionAlexander Santiago ParelNo ratings yet
- Post Internship Version 1Document4 pagesPost Internship Version 1Alexander Santiago ParelNo ratings yet
- I. Matching Type (15 PTS.)Document3 pagesI. Matching Type (15 PTS.)Alexander Santiago ParelNo ratings yet
- Mcheel Boarding House: This Certifies ThatDocument1 pageMcheel Boarding House: This Certifies ThatAlexander Santiago ParelNo ratings yet
- Enrico L. CaccamDocument2 pagesEnrico L. CaccamAlexander Santiago ParelNo ratings yet
- A Genealogical Analysis of PassivityDocument145 pagesA Genealogical Analysis of PassivityAlexander Santiago ParelNo ratings yet
- Final Informal-Settler-Families FINALDocument3 pagesFinal Informal-Settler-Families FINALAlexander Santiago ParelNo ratings yet
- DesiderataDocument1 pageDesiderataAlexander Santiago ParelNo ratings yet
- Cardiac ArrestDocument4 pagesCardiac ArrestAlexander Santiago Parel0% (1)
- MountaiNut Back LabelDocument1 pageMountaiNut Back LabelAlexander Santiago ParelNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument45 pagesChronic Obstructive Pulmonary DiseaseAlexander Santiago ParelNo ratings yet
- ABG and Oximetry StudentDocument86 pagesABG and Oximetry StudentAlexander Santiago ParelNo ratings yet
- Sleep ApneaDocument14 pagesSleep ApneaAlexander Santiago ParelNo ratings yet
- Pulmo ThromboembolismDocument34 pagesPulmo ThromboembolismAlexander Santiago ParelNo ratings yet
- Pleural EffDocument30 pagesPleural EffAlexander Santiago ParelNo ratings yet
- Lung CaDocument38 pagesLung CaAlexander Santiago ParelNo ratings yet
- ABG Terms To Know (Merged JPG Files)Document11 pagesABG Terms To Know (Merged JPG Files)Alexander Santiago ParelNo ratings yet
- Lung CaDocument38 pagesLung CaAlexander Santiago ParelNo ratings yet
- Pediatric and Neonatal Respiratory Care DevelopmentDocument205 pagesPediatric and Neonatal Respiratory Care DevelopmentAlexander Santiago ParelNo ratings yet
- Pediatric and Neonatal Respiratory Care DevelopmentDocument205 pagesPediatric and Neonatal Respiratory Care DevelopmentAlexander Santiago ParelNo ratings yet
- The Cardiovascular System ExplainedDocument11 pagesThe Cardiovascular System ExplainedBlack QueenNo ratings yet
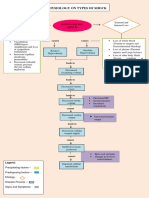
- Pathophysiology On Types of ShockDocument4 pagesPathophysiology On Types of ShockJessa Mae Alforque AsentistaNo ratings yet
- ClinicalfeaturesDocument11 pagesClinicalfeaturesapi-526590140No ratings yet
- Patient FinalDocument51 pagesPatient FinalCharmmaine Yu-AcmanNo ratings yet
- CirculatorySystemSE - Anthony HernandezDocument5 pagesCirculatorySystemSE - Anthony HernandezAnthony Hernandez100% (1)
- Final ProgrammeDocument204 pagesFinal ProgrammeimagigatoNo ratings yet
- ELSO Interim Guidelines For Venoarterial.2Document18 pagesELSO Interim Guidelines For Venoarterial.2BiancaPancuNo ratings yet
- Wa0022Document147 pagesWa0022Rajesh KumarNo ratings yet
- Англ тести фармDocument138 pagesАнгл тести фармRodriguez Vivanco Kevin DanielNo ratings yet
- Bjon 2020 29 21 1248Document5 pagesBjon 2020 29 21 1248PAULA SORAIA CHENNo ratings yet
- Anph111 FinalsDocument50 pagesAnph111 FinalsxeanNo ratings yet
- Haemorrhage & ShockDocument22 pagesHaemorrhage & ShockAmiNo ratings yet
- Science 9Document29 pagesScience 9HanessyNo ratings yet
- Peripheral Vascular DiseaseDocument32 pagesPeripheral Vascular DiseaseShy PatelNo ratings yet
- Review in Causes of Viscosity in FluidsDocument7 pagesReview in Causes of Viscosity in FluidsSaryth Darianna Cardenas FNo ratings yet
- Regulation of Coronary Blood Flow PDFDocument330 pagesRegulation of Coronary Blood Flow PDFAlin-Octavian BorinaNo ratings yet
- The Cardiovascular System: Heart Blood VesselsDocument23 pagesThe Cardiovascular System: Heart Blood VesselsPipsNo ratings yet
- Case Report Buerger DiseaseDocument35 pagesCase Report Buerger DiseaseIsyfaun NisaNo ratings yet
- Veterinary Wounds Examination for Legal CasesDocument26 pagesVeterinary Wounds Examination for Legal CasesAhmadx Hassan100% (4)