You might also like
- LymphDocument9 pagesLymphAlyesha Maloney100% (1)
- (Methods in Molecular Biology 1323) Rémy Bosselut, Melanie S. Vacchio (Eds.) - T-Cell Development - Methods and Protocols (2016, Humana Press) PDFDocument295 pages(Methods in Molecular Biology 1323) Rémy Bosselut, Melanie S. Vacchio (Eds.) - T-Cell Development - Methods and Protocols (2016, Humana Press) PDFfrancisca100% (1)
- Blood Group in AnimalDocument15 pagesBlood Group in AnimalAashish Dhakal100% (3)
- Anti-TPO ARCDocument6 pagesAnti-TPO ARCMariaNo ratings yet
- LupusDocument28 pagesLupusRiin IrasustaNo ratings yet
- Wesnbhie45oz5jsb0nv5amut PDFDocument4 pagesWesnbhie45oz5jsb0nv5amut PDFKabir Dhankhar0% (4)
- Case StudyDocument17 pagesCase StudyLourd Andrew VillegasNo ratings yet
- Cephalexin (Drug Study)Document2 pagesCephalexin (Drug Study)Franz.thenurse688894% (17)
- 10 DOH ProgramsDocument28 pages10 DOH ProgramsDhonnalyn Amene Caballero100% (4)
- Simple Determining Charge Carried Virus: A Method For The Electrical BY ParticlesDocument4 pagesSimple Determining Charge Carried Virus: A Method For The Electrical BY ParticlesAldea VeganaNo ratings yet
- Tuberculosis of The Nasal Cavities About Four CasesDocument5 pagesTuberculosis of The Nasal Cavities About Four CasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
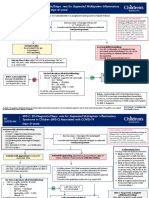
- MIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenDocument8 pagesMIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenJosselle Sempio CalientaNo ratings yet
- Glove Removal Method andDocument3 pagesGlove Removal Method andSofyan FauziNo ratings yet
- Case PresentationDocument19 pagesCase PresentationUndine TapangNo ratings yet
- Examlab 801380710 310520232344Document2 pagesExamlab 801380710 310520232344Francisco DelgadoNo ratings yet
- 3 - Sepsis Blood Culture Ss 20180505 DwsDocument26 pages3 - Sepsis Blood Culture Ss 20180505 DwsselaturNo ratings yet
- Widespread Livedoid VasculopathyDocument4 pagesWidespread Livedoid VasculopathyKata TölgyesiNo ratings yet
- Strongyloides Stercoralis Infection Causing Reversible Chronic Urticaria With Histologic Findings of Leukocytoclastic VasculitisDocument3 pagesStrongyloides Stercoralis Infection Causing Reversible Chronic Urticaria With Histologic Findings of Leukocytoclastic VasculitisGary Elvis TQNo ratings yet
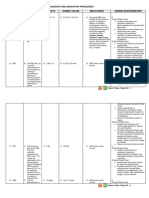
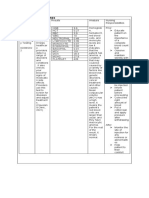
- 6 Diagnostic and Laboratory ProceduresDocument12 pages6 Diagnostic and Laboratory ProceduresJanah CalitNo ratings yet
- Clinical Microscopy - Other Body FluidsDocument93 pagesClinical Microscopy - Other Body FluidsTherese Ann Eve FlorenososNo ratings yet
- Histamine of Rectal: in Ulcerative ColitisDocument5 pagesHistamine of Rectal: in Ulcerative ColitisNejc KovačNo ratings yet
- Major Complication Cystogastrostomy: Pancreatic Abscess: A OFDocument8 pagesMajor Complication Cystogastrostomy: Pancreatic Abscess: A OFakish4uNo ratings yet
- DialysisDocument3 pagesDialysisHamed64No ratings yet
- Letter To The Editor: Comparison Between Automated and Microscopic Analysis in Body Fluids CytologyDocument3 pagesLetter To The Editor: Comparison Between Automated and Microscopic Analysis in Body Fluids CytologybalkisNo ratings yet
- RCR 30 3 07 - Cistitis - InglesDocument4 pagesRCR 30 3 07 - Cistitis - InglesAnida HasnaNo ratings yet
- Journal of Microbiological Methods: Avishai Ben-David, Charles E. DavidsonDocument8 pagesJournal of Microbiological Methods: Avishai Ben-David, Charles E. DavidsonAde RothmansNo ratings yet
- Laboratory Investigations in Uveitis: Dr. Sriniwas Atal 1 Year Resident OphthalmologyDocument39 pagesLaboratory Investigations in Uveitis: Dr. Sriniwas Atal 1 Year Resident OphthalmologySriniwasNo ratings yet
- Emphysematous Prostatitis in A Patient With DiabetesDocument3 pagesEmphysematous Prostatitis in A Patient With DiabetesChandrashekhar SohoniNo ratings yet
- ScrofulodermDocument4 pagesScrofulodermIzmi AzizahNo ratings yet
- 71 Da 03 B 8Document72 pages71 Da 03 B 8VergiliaCuflicNo ratings yet
- Normal Spontaneous Delivery Case StudyDocument8 pagesNormal Spontaneous Delivery Case Studykrystelle jade labineNo ratings yet
- Relationships Fibrosis Udder : Leucocytes Streptococci ToDocument9 pagesRelationships Fibrosis Udder : Leucocytes Streptococci ToSadam IrshadNo ratings yet
- E. Coli CellulitisDocument7 pagesE. Coli CellulitisBelajar KedokteranNo ratings yet
- BCR 2019 233131Document5 pagesBCR 2019 233131jhordyafsNo ratings yet
- A Specific Abnormal Scattergram of Peripheral Blood Leukocytes That May Suggest Hairy Cell LeukemiaDocument4 pagesA Specific Abnormal Scattergram of Peripheral Blood Leukocytes That May Suggest Hairy Cell Leukemiatufis02No ratings yet
- E in Thoven 1912Document9 pagesE in Thoven 1912ferballinaNo ratings yet
- IndianJPatholMicrobiol631140-1975569 052915 PDFDocument2 pagesIndianJPatholMicrobiol631140-1975569 052915 PDFAnita MarakNo ratings yet
- Weiland 1998Document5 pagesWeiland 1998Ottofianus Alvedo Hewick KalangiNo ratings yet
- CNS Micro ImpulseDocument44 pagesCNS Micro Impulsedineshvd75No ratings yet
- Medicina 58 00840 v2Document7 pagesMedicina 58 00840 v2elsy oktaviaNo ratings yet
- 1991 BaggishMDDocument7 pages1991 BaggishMDgiacomoNo ratings yet
- Case Report: Rapport de CasDocument3 pagesCase Report: Rapport de CasfadillahidsyamNo ratings yet
- Tuberculosis-Infected Giant Bulla Treated by PercuDocument4 pagesTuberculosis-Infected Giant Bulla Treated by Percureschita adityantiNo ratings yet
- CLSI Evaluation of CiprofloxacinDocument7 pagesCLSI Evaluation of CiprofloxacinBrainey tanjayNo ratings yet
- BBRC Vol 14 No 04 2021-03Document4 pagesBBRC Vol 14 No 04 2021-03Dr Sharique AliNo ratings yet
- Zoon's Plasma Cell Balanitis Associated With Male Genital Lichen SclerosusDocument4 pagesZoon's Plasma Cell Balanitis Associated With Male Genital Lichen SclerosusMircea-Dan Apopei-RusuNo ratings yet
- CC NotesDocument4 pagesCC NotesAgo General Hospital LaboratoryNo ratings yet
- Introduction:-: Journal HomepageDocument4 pagesIntroduction:-: Journal HomepageIJAR JOURNALNo ratings yet
- Micro AmperageDocument6 pagesMicro AmperagerameshmrsrNo ratings yet
- Use of Hydrogen Peroxide Vapor For Deactivation ofDocument7 pagesUse of Hydrogen Peroxide Vapor For Deactivation ofMd. Saddam HossainNo ratings yet
- Diagnostic ProceduresDocument1 pageDiagnostic ProceduresGladys Mae HernandezNo ratings yet
- Bacteriemies 2023Document59 pagesBacteriemies 2023Rafik BadisNo ratings yet
- Methodsx: Warren D. Gray, Adam J. Mitchell, Charles D. SearlesDocument8 pagesMethodsx: Warren D. Gray, Adam J. Mitchell, Charles D. SearlesHaja DominikeNo ratings yet
- Stein 1986Document2 pagesStein 1986ThomasHeblingerNo ratings yet
- Jurnal LED Internasional PDFDocument1 pageJurnal LED Internasional PDFJamaludin Winarhadi KusumoNo ratings yet
- Isolation IDof StrepDocument13 pagesIsolation IDof Strepidris rabiluNo ratings yet
- Volume 36 Number 2 Article6 PDFDocument11 pagesVolume 36 Number 2 Article6 PDFWirjapratama PutraNo ratings yet
- Kawasaki - Lab&drug, NCPDocument18 pagesKawasaki - Lab&drug, NCPJayzee ServantesNo ratings yet
- Case Report: First Report of Orchitis in Man Caused by Brucella Abortus Biovar 1 in EcuadorDocument5 pagesCase Report: First Report of Orchitis in Man Caused by Brucella Abortus Biovar 1 in EcuadorChandra Gunawan SihombingNo ratings yet
- Acad Dermatol Venereol - 2023 - Riebenbauer - Detection of A Knockdown Mutation in The Voltage Sensitive Sodium ChannelDocument7 pagesAcad Dermatol Venereol - 2023 - Riebenbauer - Detection of A Knockdown Mutation in The Voltage Sensitive Sodium ChannelChayru nisaNo ratings yet
- LabsDocument3 pagesLabsJan DamesNo ratings yet
- KDHE Bureau of Epidemiology and Public Health Informatics Infectious Disease Epidemiology and Response Section Standard Infectious Disease ClassificationsDocument36 pagesKDHE Bureau of Epidemiology and Public Health Informatics Infectious Disease Epidemiology and Response Section Standard Infectious Disease ClassificationsHielmy Auliya HasyimNo ratings yet
- Tablas Complementarias Art CovidDocument6 pagesTablas Complementarias Art CovidAndrés Gaviria CNo ratings yet
- Oral Manifestation TuberculosisDocument4 pagesOral Manifestation TuberculosisPetronela Ekowati PraptiningsihNo ratings yet
- Tests For The Diagnosis of Clostridium Difficile Infection The Next GenerationDocument5 pagesTests For The Diagnosis of Clostridium Difficile Infection The Next GenerationClovis Moreira JrNo ratings yet
- (18414036 - ARS Medica Tomitana) Study of Biochemical and Hematological Markers in Patients Diagnosed With Basal Cell CarcinomaDocument5 pages(18414036 - ARS Medica Tomitana) Study of Biochemical and Hematological Markers in Patients Diagnosed With Basal Cell CarcinomalgNo ratings yet
- Juji 1972Document11 pagesJuji 1972MariaNo ratings yet
- Medi 96 E7139Document4 pagesMedi 96 E7139MariaNo ratings yet
- Popp 2011Document7 pagesPopp 2011MariaNo ratings yet
- Plapp 1984Document3 pagesPlapp 1984MariaNo ratings yet
- 6 Euro Virology Congress and Expo: March 10-12, 2016 Madrid, SpainDocument1 page6 Euro Virology Congress and Expo: March 10-12, 2016 Madrid, SpainMariaNo ratings yet
- Phenobarbital ARCDocument7 pagesPhenobarbital ARCMariaNo ratings yet
- Anti-TG ARCDocument7 pagesAnti-TG ARCMariaNo ratings yet
- 1 s2.0 S0753332216313294 MainDocument12 pages1 s2.0 S0753332216313294 MainMariaNo ratings yet
- Epigenetic Alterations in The Gastrointestinal Tract: Current and Emerging Use For Biomarkers of CancerDocument20 pagesEpigenetic Alterations in The Gastrointestinal Tract: Current and Emerging Use For Biomarkers of CancerMariaNo ratings yet
- Colorectal Cancer Alliance BRAF BiomarkerDocument2 pagesColorectal Cancer Alliance BRAF BiomarkerMariaNo ratings yet
- Format For Manuscript Submission: ReviewDocument26 pagesFormat For Manuscript Submission: ReviewMariaNo ratings yet
- Colorectal Cancer Alliance NRAS BiomarkerDocument2 pagesColorectal Cancer Alliance NRAS BiomarkerMariaNo ratings yet
- Guidelines For AuthorsDocument15 pagesGuidelines For AuthorsMariaNo ratings yet
- TOEFLPracticeTest Pages 7 25.Document19 pagesTOEFLPracticeTest Pages 7 25.Camilo RomeroNo ratings yet
- Summary of Communicable DiseaseDocument13 pagesSummary of Communicable DiseaseLyka PiqueroNo ratings yet
- Handout Medical Surgical Nursing Lyme DiseaseDocument4 pagesHandout Medical Surgical Nursing Lyme DiseasePaul Christian P. Santos, RNNo ratings yet
- CD Summer Review 1Document157 pagesCD Summer Review 1Nikko MelencionNo ratings yet
- Morphology of Acute InflammationDocument16 pagesMorphology of Acute InflammationPradeepNo ratings yet
- Human Immunodeficiency Virus: Presented by Rughoobur Chitra Group 2 (A) Faculty of Foreign StudentsDocument51 pagesHuman Immunodeficiency Virus: Presented by Rughoobur Chitra Group 2 (A) Faculty of Foreign StudentskrughooburNo ratings yet
- Kuby Immunology TransplantationDocument21 pagesKuby Immunology TransplantationMalki kawtarNo ratings yet
- Lymphatic System-3 PDFDocument93 pagesLymphatic System-3 PDFDesmond BwalyaNo ratings yet
- Phadiatop Rev 051605Document1 pagePhadiatop Rev 051605Kat Chique BNo ratings yet
- Weekly Writing Assignment #10: Public Health and Individual RightsDocument2 pagesWeekly Writing Assignment #10: Public Health and Individual RightsMusfiqur RahmanNo ratings yet
- Sepsis-Syok Septik 5-12-15Document36 pagesSepsis-Syok Septik 5-12-15Titi Nur IndrawatiNo ratings yet
- CRP-Latex: Clinical SignificanceDocument3 pagesCRP-Latex: Clinical Significancedanasultan244No ratings yet
- 277 2010 Article 908Document11 pages277 2010 Article 908Mochamad HuseinNo ratings yet
- Https Kansalainen - Kanta.fi PDF Koronarokotustodistus Tmp1629635023801149Document1 pageHttps Kansalainen - Kanta.fi PDF Koronarokotustodistus Tmp1629635023801149kattosepatNo ratings yet
- COVID-19 Response - Living With COVID-19Document63 pagesCOVID-19 Response - Living With COVID-19eman mamdohNo ratings yet
- Febrile Antigens Package InsertDocument2 pagesFebrile Antigens Package InsertAhmed AliNo ratings yet
- Dr. Nanang PB 00 Autoimmune Disease Planary KONAS Bandung 2014Document60 pagesDr. Nanang PB 00 Autoimmune Disease Planary KONAS Bandung 2014Anton HilmanNo ratings yet
- Dengu Fever-Simple by DR SarmaDocument35 pagesDengu Fever-Simple by DR SarmaSanjay NavaleNo ratings yet
- Visceral Leishmaniasis in IndiaDocument27 pagesVisceral Leishmaniasis in IndiaNishant SrivastavaNo ratings yet
- Temperature Sensitivity of Vaccines: March 2014Document12 pagesTemperature Sensitivity of Vaccines: March 2014Sergio de Jesús Jaime RodríguezNo ratings yet
- GIT Viral Hepatitis in Children - PPT 93Document22 pagesGIT Viral Hepatitis in Children - PPT 93Dr.P.NatarajanNo ratings yet
- Erythrodermic Paraneoplastic Dermatomyositis: Practice - Clinical ImagesDocument1 pageErythrodermic Paraneoplastic Dermatomyositis: Practice - Clinical ImagesM.DalaniNo ratings yet
- The Value of Tzanck SmearDocument7 pagesThe Value of Tzanck SmearpramodjaliNo ratings yet
- Basic of AutoimmunityDocument13 pagesBasic of Autoimmunitymahadevabhu07100% (1)