You might also like
- Handbook of Improving Performance in the Workplace, The Handbook of Selecting and Implementing Performance InterventionsFrom EverandHandbook of Improving Performance in the Workplace, The Handbook of Selecting and Implementing Performance InterventionsNo ratings yet
- The National Occupational Therapy PractiDocument8 pagesThe National Occupational Therapy Practir.alhaqbani2023No ratings yet
- Applying Client-Centred Guidelines to Pediatric OTDocument7 pagesApplying Client-Centred Guidelines to Pediatric OTRaphael AguiarNo ratings yet
- 569 PDFDocument7 pages569 PDFferas ahmedNo ratings yet
- Jurnal EBP SOPDocument6 pagesJurnal EBP SOPYusrina RahmaNo ratings yet
- 20240419T125234_oct3104_evaluation_and_assessmentDocument16 pages20240419T125234_oct3104_evaluation_and_assessmentanjasnellenburg5No ratings yet
- Client-Centered AssessmentDocument4 pagesClient-Centered AssessmentHon “Issac” KinHoNo ratings yet
- Occupation-Centered Assessment of Children: Wendy CosterDocument8 pagesOccupation-Centered Assessment of Children: Wendy CosterAna Claudia GomesNo ratings yet
- Introduction To Evaluation and InterviewingDocument19 pagesIntroduction To Evaluation and InterviewingMaria AiramNo ratings yet
- Development of the Satisfaction with Performance Scaled Questionnaire (SPSQDocument7 pagesDevelopment of the Satisfaction with Performance Scaled Questionnaire (SPSQlewamNo ratings yet
- AMEE Guide No. 18: Standard Setting in Student Assessment: Miriam Friedman Ben-DavidDocument11 pagesAMEE Guide No. 18: Standard Setting in Student Assessment: Miriam Friedman Ben-DaviddrtayzarNo ratings yet
- Quest WfotDocument50 pagesQuest WfotRaquel LimaNo ratings yet
- OT Process MapDocument2 pagesOT Process MapFrancesNo ratings yet
- 7 - Practice Skills in Social Work and Welfare More Th... - (Part III Assessment)Document15 pages7 - Practice Skills in Social Work and Welfare More Th... - (Part III Assessment)Ivy WangNo ratings yet
- Understanding Quantitative Research1Document6 pagesUnderstanding Quantitative Research1judyNo ratings yet
- Psych Assessment NotesDocument7 pagesPsych Assessment NotesJeann RegachoNo ratings yet
- PosterDocument1 pagePosterapi-525319529No ratings yet
- Flexible Instructional Delivery Plan First Quarter: Northwestern Agusan Collges Bayview Hill, Nasipit, Agusan Del NorteDocument4 pagesFlexible Instructional Delivery Plan First Quarter: Northwestern Agusan Collges Bayview Hill, Nasipit, Agusan Del NorteDante Jr. BitoonNo ratings yet
- HWE Reference GuideDocument84 pagesHWE Reference GuideMarta GonçalvesNo ratings yet
- Carr Et Al. (2013) Performance Diagnostic Checklist (PDC-HS)Document17 pagesCarr Et Al. (2013) Performance Diagnostic Checklist (PDC-HS)JohnNo ratings yet
- Better Data. Better Outcomes.: Expect More... ... Your Patients DoDocument5 pagesBetter Data. Better Outcomes.: Expect More... ... Your Patients DoDaniel BañuelosNo ratings yet
- Occupational Therapy Assessments and Interventions in Mental HealthDocument13 pagesOccupational Therapy Assessments and Interventions in Mental HealthWabo DimitriNo ratings yet
- Improving Quality Large Scale Public Radiology Practice Through Tele-UltrasoundDocument1 pageImproving Quality Large Scale Public Radiology Practice Through Tele-Ultrasoundnpr00No ratings yet
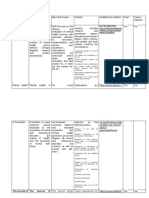
- Title Author Name Published Date Objectives Research Methodolgy Analysis and Interpretation ConclusionDocument5 pagesTitle Author Name Published Date Objectives Research Methodolgy Analysis and Interpretation ConclusionDixith NagarajanNo ratings yet
- Standards Nursing of CareDocument7 pagesStandards Nursing of CareVin BitzNo ratings yet
- 4 Ways of Knowing (Reference Balita C. Et Al)Document5 pages4 Ways of Knowing (Reference Balita C. Et Al)JEREMY MAKALINTALNo ratings yet
- SupportPer Profile PDFDocument22 pagesSupportPer Profile PDFZulvikar UmasangadjiNo ratings yet
- BEME Guide No. 10 PDFDocument22 pagesBEME Guide No. 10 PDFarum cahyaning kartikaNo ratings yet
- Wa0028.Document6 pagesWa0028.Restika Putry Nurianti AkuntansiNo ratings yet
- Child-Report Measures of Occup PDFDocument25 pagesChild-Report Measures of Occup PDFVero MoldovanNo ratings yet
- Nursing Audit: 17 July 11Document4 pagesNursing Audit: 17 July 11sangmasweety22No ratings yet
- Aota Professional Development ToolDocument2 pagesAota Professional Development Toolapi-436821531100% (1)
- Critical Analysis Paper LD PDFDocument13 pagesCritical Analysis Paper LD PDFKenNo ratings yet
- Nihms 564241Document33 pagesNihms 564241Natalia BettancourtNo ratings yet
- Research Article: Integrating Occupational Therapy Specific Assessments in Practice: Exploring Practitioner ExperiencesDocument8 pagesResearch Article: Integrating Occupational Therapy Specific Assessments in Practice: Exploring Practitioner ExperiencesNataliaNo ratings yet
- Standards of Practice For OTDocument3 pagesStandards of Practice For OTGhea Mae Jukebox VillasNo ratings yet
- Psychometric Properties of the Functional Idiographic Assessment Template-Questionnaire (FIAT-QDocument12 pagesPsychometric Properties of the Functional Idiographic Assessment Template-Questionnaire (FIAT-Qdomingo jesus de la rosa diazNo ratings yet
- ch4 Criterion-MeasuresDocument4 pagesch4 Criterion-Measuresjgd65yw5j4No ratings yet
- Perspectives On Models of Job Performance: Chockalingam Viswesvaran and Deniz S. OnesDocument11 pagesPerspectives On Models of Job Performance: Chockalingam Viswesvaran and Deniz S. OnesanitaNo ratings yet
- Improving Customer Service in Sunpharma PharmaciesDocument7 pagesImproving Customer Service in Sunpharma PharmaciesSiddhant ShekharNo ratings yet
- Overall Approach To StrategyDocument1 pageOverall Approach To StrategytejuNo ratings yet
- An Introduction To Cognitive Behaviour Therapy (CBT)Document1 pageAn Introduction To Cognitive Behaviour Therapy (CBT)rpa41995No ratings yet
- Critical AppraisalDocument15 pagesCritical AppraisalZeus HunterNo ratings yet
- Workplace StressDocument10 pagesWorkplace Stresspinku13No ratings yet
- A Study of Employee Performance Appraisal Practices in Selected Hospitals of North IndiaDocument7 pagesA Study of Employee Performance Appraisal Practices in Selected Hospitals of North IndiaRakesh NayakNo ratings yet
- Week 6 Case Project Presentationtobe EditedDocument18 pagesWeek 6 Case Project Presentationtobe Editedmaryam sherazNo ratings yet
- Industrial RehabDocument54 pagesIndustrial RehabMiti ThakkarNo ratings yet
- The Effectiveness of Self-Assessment On The Identification of Learner Needs, Learner Activity, and Impact On Clinical Practice: BEME Guide No. 10Document23 pagesThe Effectiveness of Self-Assessment On The Identification of Learner Needs, Learner Activity, and Impact On Clinical Practice: BEME Guide No. 10Ariza Cisnero DelacruzNo ratings yet
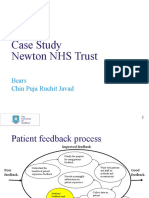
- NHS Case Study - 1023Document5 pagesNHS Case Study - 1023Javad ThasimNo ratings yet
- Psychological Assessment Chapter 7: Utility of TestsDocument7 pagesPsychological Assessment Chapter 7: Utility of TestsSam CruzNo ratings yet
- 1.1. Core Competencies Diagram - 1Document1 page1.1. Core Competencies Diagram - 1Kusrini Kadar SyamsalamNo ratings yet
- MHR Unit4 2014Document46 pagesMHR Unit4 2014Ivan BongNo ratings yet
- At DefDocument9 pagesAt DefDilraj Singh BalNo ratings yet
- Mental Health & Prevention Journal guidelines, scope, and indexingDocument4 pagesMental Health & Prevention Journal guidelines, scope, and indexingTeofilo Palsimon Jr.No ratings yet
- Nur 332 Ebp PosterDocument1 pageNur 332 Ebp Posterapi-419091662No ratings yet
- ch5 Performance-AppraisalDocument5 pagesch5 Performance-Appraisaljgd65yw5j4No ratings yet
- Advancing The Assessment of Professional Learning, Self-Care, and CompetenceDocument11 pagesAdvancing The Assessment of Professional Learning, Self-Care, and CompetenceJulio César Cristancho GarcíaNo ratings yet
- Bioethics A Nursing Perspective - (CHAPTER 1 Professional Standards and The Requirement To Be Ethical)Document8 pagesBioethics A Nursing Perspective - (CHAPTER 1 Professional Standards and The Requirement To Be Ethical)Vicente MercaderNo ratings yet
- Reliability and Validity of The Turkish Version of The Job Performance Scale InstrumentDocument9 pagesReliability and Validity of The Turkish Version of The Job Performance Scale InstrumentsatmayaniNo ratings yet
- Procedure-Based Assessments in Trauma and Orthopaedic Training - The Trainees' PerspectiveDocument6 pagesProcedure-Based Assessments in Trauma and Orthopaedic Training - The Trainees' PerspectiveSaleh MuzaniNo ratings yet
- Pedi-Cat PCDocument7 pagesPedi-Cat PCLetícia AndradeNo ratings yet
- Establishing Minimal Clinically Important Differences For Scores 2003Document11 pagesEstablishing Minimal Clinically Important Differences For Scores 2003Letícia AndradeNo ratings yet
- PEDI-CAT BR Tradução e Adaptação CulturalDocument10 pagesPEDI-CAT BR Tradução e Adaptação CulturalLetícia AndradeNo ratings yet
- ValidadeConcorrenteConfiabilidadePEDI CATDocument6 pagesValidadeConcorrenteConfiabilidadePEDI CATLetícia AndradeNo ratings yet
- Diamantis 2006Document7 pagesDiamantis 2006Letícia AndradeNo ratings yet
- The COSMIN Study Reached International CDocument9 pagesThe COSMIN Study Reached International CThilo ReinhardNo ratings yet
- Aplicabilidade PEDI-CAT TEADocument22 pagesAplicabilidade PEDI-CAT TEALetícia AndradeNo ratings yet
- CommentaryPEDI CAT&CIFDocument1 pageCommentaryPEDI CAT&CIFLetícia AndradeNo ratings yet
- Accuracy and precision of the Pediatric Evaluation of Disability Inventory computer-adaptive tests (PEDI-CATDocument7 pagesAccuracy and precision of the Pediatric Evaluation of Disability Inventory computer-adaptive tests (PEDI-CATLetícia AndradeNo ratings yet
- Nigeria Regulatory Market ProfileDocument15 pagesNigeria Regulatory Market ProfilevikramchotsNo ratings yet
- Foodborne IllnessDocument18 pagesFoodborne IllnesspaanarNo ratings yet
- Article+0202 368 379Document12 pagesArticle+0202 368 379Muhammad Alif Nur FaizinNo ratings yet
- 273 Health Science 6 12Document47 pages273 Health Science 6 12المعتزبالله جاب اللهNo ratings yet
- The Tao of Bipolar PDFDocument195 pagesThe Tao of Bipolar PDFSSS100% (1)
- Mental health effects of distance learningDocument7 pagesMental health effects of distance learningJohn Patrick GarciaNo ratings yet
- THE ETHICS OF PUBLIC HEALTH SURVEILLANCE MCQsDocument2 pagesTHE ETHICS OF PUBLIC HEALTH SURVEILLANCE MCQsChaman Lal Karotia100% (1)
- 681 FullDocument6 pages681 FullKurnia AnharNo ratings yet
- Inadequate Living Space - NCPDocument2 pagesInadequate Living Space - NCPissaiahnicolleNo ratings yet
- Q1 TLE 10-12 Wellness Massage NCII Module 4Document21 pagesQ1 TLE 10-12 Wellness Massage NCII Module 4Kim Caguioa100% (2)
- CaseDocument5 pagesCaseFejlean Angelica AntineoNo ratings yet
- Harry Guess, Linda Engel, Arthur Kleinman, John Kusek Science of The Placebo Toward An Interdisciplinanary Research Agenda Evidence-Based Medicine Workbks. 2002Document345 pagesHarry Guess, Linda Engel, Arthur Kleinman, John Kusek Science of The Placebo Toward An Interdisciplinanary Research Agenda Evidence-Based Medicine Workbks. 2002rockspirit02No ratings yet
- Teens Your Brain Needs Real FoodDocument4 pagesTeens Your Brain Needs Real FoodGiovana NavaNo ratings yet
- Volunteer Handbook 2019Document12 pagesVolunteer Handbook 2019Katharine Tondra100% (1)
- Drug Related ProblemDocument34 pagesDrug Related ProblemERONADIAULFAH SUGITONo ratings yet
- Managing Discomforts During PregnancyDocument3 pagesManaging Discomforts During PregnancyMariana Mikaela AlagarNo ratings yet
- Makabuhay (Tinospora RumphiiDocument4 pagesMakabuhay (Tinospora RumphiiErica Ritz TrainNo ratings yet
- IQVIA CH - November 14th 2023Document75 pagesIQVIA CH - November 14th 2023alina.rxa.tdrNo ratings yet
- The Human Microbiome and Infectious Diseases: Beyond KochDocument151 pagesThe Human Microbiome and Infectious Diseases: Beyond KochRamesh ShahNo ratings yet
- Scalp Acupuncture BasicsDocument27 pagesScalp Acupuncture BasicsGanga SinghNo ratings yet
- Emocional Health: Emotiona L Health Activities at HomeDocument1 pageEmocional Health: Emotiona L Health Activities at HomeMarianne Herzfeld FajardoNo ratings yet
- Rheotorical Analysis - Sel 107 45Document3 pagesRheotorical Analysis - Sel 107 45api-607584974No ratings yet
- MSCDFSM Prog. GuideDocument108 pagesMSCDFSM Prog. Guidesamraju1No ratings yet
- Nursing ResponsibilitiesDocument4 pagesNursing ResponsibilitiesMaureen Joy Cascayan EspirituNo ratings yet
- Letter To SenatorDocument2 pagesLetter To Senatorapi-285779835No ratings yet
- Preparing For Face-To-Face Classes: Better DaysDocument3 pagesPreparing For Face-To-Face Classes: Better DaysMaria Cristina LolosNo ratings yet
- Hipertensi KebidananDocument77 pagesHipertensi KebidananNINING ALKOMAHNo ratings yet
- CAP Test 1 - For Pm101Document3 pagesCAP Test 1 - For Pm101NizNo ratings yet
- Mood Disorder GuideDocument18 pagesMood Disorder GuideDwi SeptaNo ratings yet
- Baking Soda Cures Cancer, Fungus and InflammationDocument6 pagesBaking Soda Cures Cancer, Fungus and Inflammationsheriff77080% (5)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (24)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)