You might also like
- Squirt! The Female Ejaculation Black BookDocument35 pagesSquirt! The Female Ejaculation Black BookAARON AYIKU50% (2)
- Female Pelvic Floor 2 Assessment and Rehabilitation PDFDocument4 pagesFemale Pelvic Floor 2 Assessment and Rehabilitation PDFVikiNo ratings yet
- OT Self Care Modified Barthel IndexDocument4 pagesOT Self Care Modified Barthel Indexlolocy LNo ratings yet
- Urinary IncontinenceDocument66 pagesUrinary Incontinencedr_asaleh100% (1)
- The Clean Kid Manual - ExcerptDocument20 pagesThe Clean Kid Manual - ExcerptGary DusterwinkleNo ratings yet
- Catheterization ChecklistDocument3 pagesCatheterization ChecklistAlthea Aubrey AgbayaniNo ratings yet
- Urodynamic Testing ReportDocument25 pagesUrodynamic Testing Reportzharah180% (1)
- Nursing Management of Patients With Urinary IncontinenceDocument45 pagesNursing Management of Patients With Urinary IncontinenceMheanne RomanoNo ratings yet
- Sterile Urethral Catheters For Single Use: British Standard Bs en 1616: 1997Document18 pagesSterile Urethral Catheters For Single Use: British Standard Bs en 1616: 1997JoannaJames75% (4)
- Presentation On Renal CalculiDocument16 pagesPresentation On Renal CalculiSangay CheshireNo ratings yet
- Comparison of Transcutaneous Electrical Tibial Nervestimulation For The Treatment of Overactive Bladder-A Multi-Arm Randomized Controlled Trial With BlindedassessmentDocument6 pagesComparison of Transcutaneous Electrical Tibial Nervestimulation For The Treatment of Overactive Bladder-A Multi-Arm Randomized Controlled Trial With BlindedassessmentMUHAMMMAD FAKHRINo ratings yet
- Adobe PDF Library 7.0 - Adobe InDesign CS2 (4.0.5) - 000027Document7 pagesAdobe PDF Library 7.0 - Adobe InDesign CS2 (4.0.5) - 000027Dr. Adel AlhusainiNo ratings yet
- Safety Pilot Study On DoctorsDocument4 pagesSafety Pilot Study On DoctorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Efficacy and Safety of Sacral Nerve Stimulation For Urinary Urge Incontinence - A Systematic ReviewDocument7 pagesEfficacy and Safety of Sacral Nerve Stimulation For Urinary Urge Incontinence - A Systematic ReviewMUHAMMMAD FAKHRINo ratings yet
- Dickson 2014Document7 pagesDickson 2014Sarra Bouslah Ep BouaouinaNo ratings yet
- Urinary Incontinence in Norwegian Nursing Home ResidentsDocument7 pagesUrinary Incontinence in Norwegian Nursing Home ResidentsKrisnawatiNo ratings yet
- Espino-Renal Replacement TherapyDocument5 pagesEspino-Renal Replacement TherapyEmi EspinoNo ratings yet
- Acnr Artical BelgeumDocument5 pagesAcnr Artical BelgeumAnna ApetriNo ratings yet
- Atuação em DisfagiaDocument4 pagesAtuação em DisfagiaconradNo ratings yet
- PIIS2405456922002619Document7 pagesPIIS2405456922002619Oriol Colet GuitertNo ratings yet
- LiteratureDocument5 pagesLiteratureBrightworld ProjectsNo ratings yet
- Role of Interferential Therapy Along With Pelvic Floor Exercises in The Management of Stress IncontinenceDocument4 pagesRole of Interferential Therapy Along With Pelvic Floor Exercises in The Management of Stress IncontinenceGlboy ManNo ratings yet
- The Effects of The ReWalk™ Robotic System On Walking Capability in Paraplegic Spinal Cord Injury PatientsDocument8 pagesThe Effects of The ReWalk™ Robotic System On Walking Capability in Paraplegic Spinal Cord Injury PatientsFrankChenNo ratings yet
- RESEARCH ARTICLEOpen AccessChallenges of Acute Peritoneal Dialysis Inextremely-Low-Birth-Weight Infants - Aretrospective Cohort StudyDocument9 pagesRESEARCH ARTICLEOpen AccessChallenges of Acute Peritoneal Dialysis Inextremely-Low-Birth-Weight Infants - Aretrospective Cohort StudysavitageraNo ratings yet
- CA.R.PE - DI.E.M. (Cardio - Renal Pediatric Dialysis Emergency Machine) : Evolution of Continuous Renal Replacement Therapies in Infants. A Personal JourneyDocument9 pagesCA.R.PE - DI.E.M. (Cardio - Renal Pediatric Dialysis Emergency Machine) : Evolution of Continuous Renal Replacement Therapies in Infants. A Personal JourneyTrang NguyenNo ratings yet
- Posterior Tibial Nerve Stimulation For Overactive Bladder-Techniques and EfficacyDocument6 pagesPosterior Tibial Nerve Stimulation For Overactive Bladder-Techniques and Efficacymarco romeroNo ratings yet
- A Novel Technique For Treatment of Distal Ureteral Calculi: Early ResultsDocument4 pagesA Novel Technique For Treatment of Distal Ureteral Calculi: Early ResultsTheQueensafa90No ratings yet
- AlAbdulwahab 2010Document9 pagesAlAbdulwahab 2010Nacho MicheloniNo ratings yet
- Original Research: Flexible Ureteroscopic Lithotripsy For The Treatment of Upper Urinary Tract Calculi in InfantsDocument7 pagesOriginal Research: Flexible Ureteroscopic Lithotripsy For The Treatment of Upper Urinary Tract Calculi in InfantsFusarina MumpuniNo ratings yet
- Bladder Training Stroke PDFDocument10 pagesBladder Training Stroke PDFLeony KhairunisaNo ratings yet
- Infected Meckels Diverticulum Masquerading As Spontaneous Rupture of Umbilical Granuloma - A Case Report in One Month Old InfantDocument4 pagesInfected Meckels Diverticulum Masquerading As Spontaneous Rupture of Umbilical Granuloma - A Case Report in One Month Old InfantIJAR JOURNALNo ratings yet
- Functional Outcome After Neonatal Pyeloplasty in Antenatally Diagnosed Uretero-Pelvic Junction ObstructionDocument5 pagesFunctional Outcome After Neonatal Pyeloplasty in Antenatally Diagnosed Uretero-Pelvic Junction ObstructionunpadurologyNo ratings yet
- Krav Chick 2005Document4 pagesKrav Chick 2005victorcborgesNo ratings yet
- Wrap Plication of Megaureter Around Normal-Sized Ureter For Complete Duplex System ReimplantationsDocument5 pagesWrap Plication of Megaureter Around Normal-Sized Ureter For Complete Duplex System ReimplantationsDirga Rasyidin LNo ratings yet
- Biomedicines 10 00675Document17 pagesBiomedicines 10 00675tasialalalaNo ratings yet
- Oral Rehydration Therapy For Preoperative Fluid and Electrolyte Man-AgementDocument9 pagesOral Rehydration Therapy For Preoperative Fluid and Electrolyte Man-AgementSasmira JamalNo ratings yet
- Ecr2012 C-1412Document10 pagesEcr2012 C-1412CentanarianNo ratings yet
- Terapia VibratoriaDocument4 pagesTerapia VibratoriaDanny QuezadaNo ratings yet
- Lang 2011Document14 pagesLang 2011aungmyintkyawdrNo ratings yet
- MVMJ - Volume 22 - Issue 4 - Pages 141-146Document7 pagesMVMJ - Volume 22 - Issue 4 - Pages 141-146HebaNo ratings yet
- Treatment of Acute Diarrhoea in Adults With Dioctahedral Smectite (Smecta) : A Prospective Randomised StudyDocument6 pagesTreatment of Acute Diarrhoea in Adults With Dioctahedral Smectite (Smecta) : A Prospective Randomised StudyJose Miguel TovarNo ratings yet
- Medical/ Surgical Management: Cholecystectomy#download&from - EmbedDocument5 pagesMedical/ Surgical Management: Cholecystectomy#download&from - EmbedHashim JeburNo ratings yet
- Shehata 2016Document21 pagesShehata 2016pznrzjsttjNo ratings yet
- Post Operative FastingDocument7 pagesPost Operative FastingUsama SaeedNo ratings yet
- Jurnal Latihan Kegel ExcerciseDocument6 pagesJurnal Latihan Kegel ExcerciseIksan KhoironiNo ratings yet
- Art:10.1007/s00383 011 2913 5Document5 pagesArt:10.1007/s00383 011 2913 5Rajarshi KumarNo ratings yet
- Kidney Failure Research PaperDocument5 pagesKidney Failure Research Paperfvehwd96100% (1)
- Pedia TriDocument6 pagesPedia TriRIZHAN ATHAYANo ratings yet
- Cholecystectomy#download&from - Embed: Medical/ Surgical ManagementDocument5 pagesCholecystectomy#download&from - Embed: Medical/ Surgical ManagementHashim JeburNo ratings yet
- Treatment of Upper Urinary Tract Stones With Extracorporeal Shock Wave Lithotripsy (ESWL) Sonolith VisionDocument5 pagesTreatment of Upper Urinary Tract Stones With Extracorporeal Shock Wave Lithotripsy (ESWL) Sonolith VisionTatik HandayaniNo ratings yet
- Seminars in Pediatric Surgery: Short Bowel Syndrome in Children: Surgical and Medical PerspectivesDocument7 pagesSeminars in Pediatric Surgery: Short Bowel Syndrome in Children: Surgical and Medical PerspectivesrodyNo ratings yet
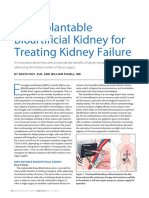
- An Implantable Bioartificial Kidney For Treating Kidney FailureDocument2 pagesAn Implantable Bioartificial Kidney For Treating Kidney FailureAnugrah Pangeran100% (1)
- Jor 20020Document9 pagesJor 20020Adi PopoviciNo ratings yet
- Atresia Duodenal y Atresia IntestinalDocument8 pagesAtresia Duodenal y Atresia IntestinalCrystal RamirezNo ratings yet
- Effect of Monopolar Capacitive Resistive RadiofreqDocument8 pagesEffect of Monopolar Capacitive Resistive RadiofreqNrusinghPrasadGoudaNo ratings yet
- Bischoff 2017Document6 pagesBischoff 2017Herpian NugrahadilNo ratings yet
- 6 Incontinencia PDFDocument6 pages6 Incontinencia PDFAngelica CoronaNo ratings yet
- Cell Proliferation - 2020 - Yan - Clinical Analysis of Human Umbilical Cord Mesenchymal Stem Cell Allotransplantation inDocument12 pagesCell Proliferation - 2020 - Yan - Clinical Analysis of Human Umbilical Cord Mesenchymal Stem Cell Allotransplantation inJuan FeivelNo ratings yet
- JCDR 10 QC17Document4 pagesJCDR 10 QC17H SHABANANo ratings yet
- Percutaneous Tibial Nerve Stimulation: The Urgent PC DeviceDocument6 pagesPercutaneous Tibial Nerve Stimulation: The Urgent PC Devicemoetaz gomaNo ratings yet
- How Much Do We Know About Constipation After Surgery For Anorectal Malformation?Document5 pagesHow Much Do We Know About Constipation After Surgery For Anorectal Malformation?Ade Triansyah EmsilNo ratings yet
- CA EndometriumDocument11 pagesCA EndometriumNajla IrbahNo ratings yet
- CT EnterographyDocument8 pagesCT EnterographyAbin VlNo ratings yet
- Wang 2018Document9 pagesWang 2018minh huy ThaiNo ratings yet
- Rajiv Gandhi University of Health Sciences: Proforma For Registration of Subject For DissertationDocument25 pagesRajiv Gandhi University of Health Sciences: Proforma For Registration of Subject For DissertationShivu ShivukumarNo ratings yet
- Acupressure. CKDDocument5 pagesAcupressure. CKDskmayasariNo ratings yet
- The Effectiveness and Durability of Ureteral TumorDocument4 pagesThe Effectiveness and Durability of Ureteral TumorAli SlimaniNo ratings yet
- ESWL For Pancreatic StonesDocument7 pagesESWL For Pancreatic StonesOana TimofteNo ratings yet
- Foetuses Abnormalities Caused Bytegretoldrug On Their Parents of The Albino RatDocument21 pagesFoetuses Abnormalities Caused Bytegretoldrug On Their Parents of The Albino RatIJAR JOURNALNo ratings yet
- Interpretation of Urodynamic Studies: A Case Study-Based GuideFrom EverandInterpretation of Urodynamic Studies: A Case Study-Based GuideNo ratings yet
- NCP Urinary RetentionDocument3 pagesNCP Urinary RetentionKingJayson Pacman06No ratings yet
- Chapter - 036 Urinay DisordersDocument8 pagesChapter - 036 Urinay DisordersClaudina CariasoNo ratings yet
- Full Paper - PUBLIC HEALTH CHALLENGES DUE TO INSUFFICIENT PUBLIC TOILET IN DHAKA CITY OF BANGLADESHDocument19 pagesFull Paper - PUBLIC HEALTH CHALLENGES DUE TO INSUFFICIENT PUBLIC TOILET IN DHAKA CITY OF BANGLADESHTanvir RezaNo ratings yet
- ICS Standards 2019Document936 pagesICS Standards 2019Gleiciane AguiarNo ratings yet
- Modified Manchester de BoerDocument7 pagesModified Manchester de BoerGustavo flores quispeNo ratings yet
- 20 Early Signs of Pelvic Floor DysfunctionDocument8 pages20 Early Signs of Pelvic Floor DysfunctionChechilenitaNo ratings yet
- Physical Therapy For A Child With Encopresis: A Case ReportDocument8 pagesPhysical Therapy For A Child With Encopresis: A Case ReportChiara GaleazziNo ratings yet
- Bladder Capacity ABC & Koff Formula and Daily Fluid IntakeDocument2 pagesBladder Capacity ABC & Koff Formula and Daily Fluid IntakeHeru Sutanto KNo ratings yet
- Enuresis in ChildrenDocument42 pagesEnuresis in ChildrenJood AL AbriNo ratings yet
- Pelvic Floor Exercises RV2-1Document2 pagesPelvic Floor Exercises RV2-1Ayantika SahaNo ratings yet
- Urinary Elimination: Lesson 5eDocument33 pagesUrinary Elimination: Lesson 5eMikhaela Andree MarianoNo ratings yet
- TDC001 TENA Direct Catalogue 0621 Final VDocument28 pagesTDC001 TENA Direct Catalogue 0621 Final VKidz to Adultz ExhibitionsNo ratings yet
- Warren Barr South LoopDocument7 pagesWarren Barr South LoopBeth LawrenceNo ratings yet
- Chapter 66 Care of Patients With Urinary ProblemsDocument11 pagesChapter 66 Care of Patients With Urinary ProblemsGina GiammalvoNo ratings yet
- Urinary EliminationDocument50 pagesUrinary EliminationAime MvuyekureNo ratings yet
- Script: Urinary Retention in Patient With S1-S2 LesionDocument10 pagesScript: Urinary Retention in Patient With S1-S2 LesionFrancisco PuenteNo ratings yet
- UroflowmetryDocument4 pagesUroflowmetryGolam MasudNo ratings yet
- Adventist University of The Philippines: Urinary Cathetirization P RIS RemarksDocument2 pagesAdventist University of The Philippines: Urinary Cathetirization P RIS RemarksAnnie AlbertoNo ratings yet
- 4 - CatheterizationDocument20 pages4 - Catheterizationkirstenfrancine28No ratings yet
- Elvic Floor Muscle Activity in Different Sitting Postures in Continent and Incontinent Women - Sa - 0Document7 pagesElvic Floor Muscle Activity in Different Sitting Postures in Continent and Incontinent Women - Sa - 0Pollyana Furtado JunqueiraNo ratings yet