You might also like
- OsteomylitisDocument48 pagesOsteomylitissamar yousif mohamed100% (1)
- Osteomyelitis: Deo Jake Lacpacan Jhunevyl MallorcaDocument36 pagesOsteomyelitis: Deo Jake Lacpacan Jhunevyl MallorcaDeo Jake Lacpacan100% (1)
- Osteomyelitis of JawsDocument28 pagesOsteomyelitis of JawsGujjar VishalNo ratings yet
- Osteomyelitis Oral SurgeryDocument17 pagesOsteomyelitis Oral SurgeryFourthMolar.comNo ratings yet
- Immunologic Diseases of Oral Cavity: - by Saurabh AhujaDocument34 pagesImmunologic Diseases of Oral Cavity: - by Saurabh AhujaSaurabh AhujaNo ratings yet
- Assoc. Prof. G. Tomov, PHD: Division of Oral Pathology, Faculty of Dental Medicine Mu - PlovdivDocument106 pagesAssoc. Prof. G. Tomov, PHD: Division of Oral Pathology, Faculty of Dental Medicine Mu - PlovdivAustine OsaweNo ratings yet
- Clinical and Morpho-Pathological Characteristic of Acute, Chronic and Exacherbate Stage of Apical Periodontitis. Positive and Differentiol DiagnosisDocument53 pagesClinical and Morpho-Pathological Characteristic of Acute, Chronic and Exacherbate Stage of Apical Periodontitis. Positive and Differentiol DiagnosisShany SchwarzwaldNo ratings yet
- Chronic Periodontitis: R Nael Almasri PeriodontistDocument29 pagesChronic Periodontitis: R Nael Almasri PeriodontistAssssssNo ratings yet
- Anatomy of Trigeminal Nerve & Trigeminal Neuralgia: Presented By: DR - Vansh Vardhan Madahar PG1 YearDocument47 pagesAnatomy of Trigeminal Nerve & Trigeminal Neuralgia: Presented By: DR - Vansh Vardhan Madahar PG1 YearVansh Vardhan MadaharNo ratings yet
- Chronic Apical Periodontitis.Document24 pagesChronic Apical Periodontitis.Alina EsanuNo ratings yet
- ENDO PerioDocument39 pagesENDO PerioapbhalodiNo ratings yet
- Periodontics Periodontal Instrumentation Presentation 1Document61 pagesPeriodontics Periodontal Instrumentation Presentation 1api-536835901No ratings yet
- Aggressive Periodontitis: Localized & Generalized Forms by SamDocument24 pagesAggressive Periodontitis: Localized & Generalized Forms by SamNaghman Zuberi100% (1)
- Traumatic Injuries of The TeethDocument99 pagesTraumatic Injuries of The TeethBheibie EndayaNo ratings yet
- How to Remove Plaque and Tartar From TeethDocument43 pagesHow to Remove Plaque and Tartar From TeethSecret OriginsNo ratings yet
- Principles and Management of Panfacial TraumaDocument43 pagesPrinciples and Management of Panfacial TraumaDR NASIMNo ratings yet
- Oral Candidiasis - ReviewDocument9 pagesOral Candidiasis - ReviewAdhelia Galuh PrmtsrNo ratings yet
- Periodontal Pocket: ClassificationDocument6 pagesPeriodontal Pocket: ClassificationMashal FatimaNo ratings yet
- ODONTOGENIC DISEASE of The MAXILLARY SINUS - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Document13 pagesODONTOGENIC DISEASE of The MAXILLARY SINUS - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Vinnie SinghNo ratings yet
- Inflammation SeminarDocument59 pagesInflammation SeminarVinod S Vinu100% (2)
- Oral PathologyDocument182 pagesOral PathologyPurnimaNo ratings yet
- EndodonticsDocument34 pagesEndodonticsAnggaHumalaBeltsazarNapitupuluNo ratings yet
- Actinic KeratosisDocument19 pagesActinic KeratosisDajour CollinsNo ratings yet
- Periodontitis: DR - Nael Almasri PeriodontistDocument55 pagesPeriodontitis: DR - Nael Almasri PeriodontistDentist AymanNo ratings yet
- Odontogenic CystDocument16 pagesOdontogenic CystMahsaNo ratings yet
- Dental Plaque and CalculusDocument32 pagesDental Plaque and Calculus蔡長家No ratings yet
- Horia Traian: DumitriuDocument3 pagesHoria Traian: DumitriuClinci AlexandruNo ratings yet
- CANDIDIASISDocument32 pagesCANDIDIASISShraddha SuchakNo ratings yet
- Fractures of Middle Third of Facial SkeletonDocument36 pagesFractures of Middle Third of Facial SkeletonAmy GraceNo ratings yet
- Necrotising Fascitis: Recent Advances in Surgery 39Th EditionDocument36 pagesNecrotising Fascitis: Recent Advances in Surgery 39Th EditionPraveen CpNo ratings yet
- Basic Properties of Dental MaterialsDocument47 pagesBasic Properties of Dental MaterialsSwetha RajaNo ratings yet
- Histology of PulpDocument61 pagesHistology of PulpLom SimloteNo ratings yet
- Orphanet Journal of Rare Diseases: Jacobsen SyndromeDocument10 pagesOrphanet Journal of Rare Diseases: Jacobsen SyndromeMuhammad RezaNo ratings yet
- DIFFERENTIAL DIAGNOSIS OF FIBRO-OSSEOUS LESIONDocument66 pagesDIFFERENTIAL DIAGNOSIS OF FIBRO-OSSEOUS LESIONBhupinder KaushalNo ratings yet
- Benign and Malignant Tumors of Maxillary Sinus - AshishDocument28 pagesBenign and Malignant Tumors of Maxillary Sinus - AshishKaran KhuranaNo ratings yet
- Periodontal Pockets DefinedDocument23 pagesPeriodontal Pockets Definedperiodontics07No ratings yet
- Abnormalities of The PulpDocument3 pagesAbnormalities of The PulpCyril Almario Cunanan100% (1)
- Close the Gap: Managing Midline DiastemasDocument33 pagesClose the Gap: Managing Midline DiastemasNikola DerebanNo ratings yet
- Immunology Dental Caries-2015Document24 pagesImmunology Dental Caries-2015Bagus Rahmawan50% (2)
- Recurrent Aphthous StomatitisDocument50 pagesRecurrent Aphthous StomatitisRajkumari Sriraman100% (1)
- Hypomochlion Aided Reduction For Sub-Condylar FracturesDocument2 pagesHypomochlion Aided Reduction For Sub-Condylar FracturesshyamNo ratings yet
- AG C O L: Uide To Ommon RAL EsionsDocument46 pagesAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanNo ratings yet
- Introduction to Restorations, Luting and Pulp TherapyDocument11 pagesIntroduction to Restorations, Luting and Pulp TherapyArchanaNo ratings yet
- 2014 Evaluarea Comparativă A Stării de Sănătate Oro Dentară Prin Cao Și Egohid La TineriDocument5 pages2014 Evaluarea Comparativă A Stării de Sănătate Oro Dentară Prin Cao Și Egohid La TineriancaNo ratings yet
- Acute Periapical AbscessDocument12 pagesAcute Periapical AbscessDarshilNo ratings yet
- Oral Submucous FibrosisDocument5 pagesOral Submucous Fibrosiskunnuve5005100% (1)
- RADIOGRAPHIC INTERPRETATION OF PERIODONTAL DISEASESDocument25 pagesRADIOGRAPHIC INTERPRETATION OF PERIODONTAL DISEASESFahma AlfarizqyNo ratings yet
- Emdogain 1Document6 pagesEmdogain 1Nicco MarantsonNo ratings yet
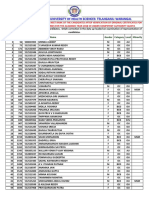
- 1430 Mbbsbdsfinalmeritlist201819 PDFDocument205 pages1430 Mbbsbdsfinalmeritlist201819 PDFVINEETH VinnuNo ratings yet
- Mosbys - Oral Diagnosis Oral Surgery and Radiology 2015Document6 pagesMosbys - Oral Diagnosis Oral Surgery and Radiology 2015LangNo ratings yet
- Histopathology of Dental Caries (39Document39 pagesHistopathology of Dental Caries (39Diana SuhartiNo ratings yet
- Facial Space InfectionsDocument76 pagesFacial Space InfectionsPrathusha UmakhanthNo ratings yet
- Deep margin elevation with DME techniqueDocument19 pagesDeep margin elevation with DME techniqueAlejandra Estrada RengelNo ratings yet
- Mandible FX Slides 040526Document62 pagesMandible FX Slides 040526azharNo ratings yet
- Benign Non Odontogenic Tumors: Ossifying FibromaDocument10 pagesBenign Non Odontogenic Tumors: Ossifying FibromaIsabelle TanNo ratings yet
- OSTEOMYELITIS OF JAW: PATHOGENESIS & MANAGEMENTDocument35 pagesOSTEOMYELITIS OF JAW: PATHOGENESIS & MANAGEMENTOded KantzukerNo ratings yet
- Osteomyelitis Of Jaws Causes, Types & TreatmentDocument11 pagesOsteomyelitis Of Jaws Causes, Types & TreatmentGujjar VishalNo ratings yet
- 2 5420394524511833795 PDFDocument232 pages2 5420394524511833795 PDFعبدالرحمن عبدالسلام ذنون المصريNo ratings yet
- 5 Inflammation of Bone NewDocument15 pages5 Inflammation of Bone Newnightfury200313No ratings yet
- 6 OsteomyelitisDocument29 pages6 OsteomyelitisMohammed AshrefNo ratings yet
- 1 Tooth ExtractionDocument27 pages1 Tooth ExtractionD YasIr MussaNo ratings yet
- 4 ImpactionDocument188 pages4 ImpactionD YasIr MussaNo ratings yet
- SuturingDocument89 pagesSuturingD YasIr Mussa100% (1)
- Local AnasthesiaDocument121 pagesLocal AnasthesiaD YasIr Mussa100% (1)
- Emergencies in Dental Practice: Instructor - DR - Jesus GeorgeDocument29 pagesEmergencies in Dental Practice: Instructor - DR - Jesus GeorgehazeemmegahedNo ratings yet
- Maxillary Injection TechniquesDocument127 pagesMaxillary Injection TechniquesD YasIr MussaNo ratings yet
- IJAA-K. K. Mubarak - Vol.2 No.2 (2015.) - 2321Document2 pagesIJAA-K. K. Mubarak - Vol.2 No.2 (2015.) - 2321D YasIr MussaNo ratings yet
- D435L09 Dental Trauma-2C Cracked Teeth - 26 Root FractureDocument73 pagesD435L09 Dental Trauma-2C Cracked Teeth - 26 Root FractureD YasIr MussaNo ratings yet
- Middle Superior Alveolar Nerve BlockDocument39 pagesMiddle Superior Alveolar Nerve Blockdaw022No ratings yet
- Parameters of CareDocument103 pagesParameters of CareAastha DuaNo ratings yet
- Adult Orthodontic TreatmentDocument9 pagesAdult Orthodontic TreatmentD YasIr MussaNo ratings yet
- Bimaxilary ProtrusionDocument7 pagesBimaxilary ProtrusionD YasIr MussaNo ratings yet
- Interdisciplinary Treatment of An Adult Patient UsDocument5 pagesInterdisciplinary Treatment of An Adult Patient UsD YasIr MussaNo ratings yet
- JIndianOrthodSoc512141-4902432 133704Document3 pagesJIndianOrthodSoc512141-4902432 133704D YasIr MussaNo ratings yet
- Examination, Diagnosis and Treatment Planning For Edentulous or Partially Edentulous PatientsDocument73 pagesExamination, Diagnosis and Treatment Planning For Edentulous or Partially Edentulous PatientsD YasIr MussaNo ratings yet
- A To Z Orthodontics. Volume 22: History Taking and ExaminationDocument39 pagesA To Z Orthodontics. Volume 22: History Taking and ExaminationD YasIr MussaNo ratings yet
- Cleft Lip and PalateDocument32 pagesCleft Lip and PalateD YasIr MussaNo ratings yet
- Educ 580 - Edpuzzle PD HandoutDocument3 pagesEduc 580 - Edpuzzle PD Handoutapi-548868233No ratings yet
- Student quiz answer sheetsDocument26 pagesStudent quiz answer sheetsSeverus S PotterNo ratings yet
- Ejc-M13 - FN953205Document203 pagesEjc-M13 - FN953205JoséNo ratings yet
- Bartending and Catering: Agenda: Basics of Bartending Bar Tools and EquipmentDocument146 pagesBartending and Catering: Agenda: Basics of Bartending Bar Tools and EquipmentMars Mar100% (1)
- Lesson 2 - Procedures in Cleaning Utensils and EquipmentDocument26 pagesLesson 2 - Procedures in Cleaning Utensils and EquipmentReizel TulauanNo ratings yet
- Linkstar RCST Installation Guide: Version DDocument56 pagesLinkstar RCST Installation Guide: Version Djorge_chavez01No ratings yet
- Mercedes Vario 1996 2003 PDF Service ManualDocument22 pagesMercedes Vario 1996 2003 PDF Service Manualveronicamurphy070288aqwNo ratings yet
- Asme B18.24-2020Document190 pagesAsme B18.24-2020윤규섭0% (1)
- Korean Enthusiasm and PatriotismDocument68 pagesKorean Enthusiasm and PatriotismYukino Hera100% (1)
- Number SystemDocument4 pagesNumber SystemGlenn ThomasNo ratings yet
- Complete Tds CourseDocument32 pagesComplete Tds CourseAMLANNo ratings yet
- KPW FSO Yetagun Presentation 250713Document36 pagesKPW FSO Yetagun Presentation 250713muhamadrafie1975No ratings yet
- Water TreatmentDocument6 pagesWater TreatmentSantiago LarrazNo ratings yet
- 178 - 7 - Fun For Flyers. Progress Tests - 2017, 4th - 91p.pdf Foods NatureDocument1 page178 - 7 - Fun For Flyers. Progress Tests - 2017, 4th - 91p.pdf Foods NatureYu KoNo ratings yet
- Report-Teaching English Ministery of EduDocument21 pagesReport-Teaching English Ministery of EduSohrab KhanNo ratings yet
- Philippine Christian University Graduate School of Business and Management Integrated Syllabi ModuleDocument5 pagesPhilippine Christian University Graduate School of Business and Management Integrated Syllabi ModuleRoselle Anne Luna GuatatoNo ratings yet
- Radiographic Examination Procedure For Asme CodeDocument33 pagesRadiographic Examination Procedure For Asme CodeEdAlmNo ratings yet
- BITS ZG628T Dissertation (For Students of M. Tech. Software Systems)Document21 pagesBITS ZG628T Dissertation (For Students of M. Tech. Software Systems)Shiva Beduduri100% (1)
- Beef Steaks: MethodDocument2 pagesBeef Steaks: MethodGoshigoshi AkhtarNo ratings yet
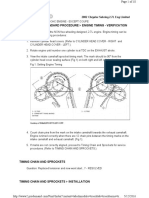
- 02+sebring+2.7+timing+chainDocument10 pages02+sebring+2.7+timing+chainMaushil Salman MarkNo ratings yet
- Apparent Dip PDFDocument2 pagesApparent Dip PDFanon_114803412No ratings yet
- 1605 HOBAS Jacking Pipes WebDocument16 pages1605 HOBAS Jacking Pipes Weballouche_abdNo ratings yet
- Dispersion of Carbon Nanotubes in Water and Non-Aqueous SolventsDocument41 pagesDispersion of Carbon Nanotubes in Water and Non-Aqueous SolventsSantiago OrtizNo ratings yet
- Cash and Cash EquivalentsDocument2 pagesCash and Cash EquivalentsMary Jullianne Caile SalcedoNo ratings yet
- MSDS Slideway Oil Iso VG 68 - 031115Document6 pagesMSDS Slideway Oil Iso VG 68 - 031115Rini SiskayantiNo ratings yet
- CEO Corner New Products Powerful Pocket SimulatorDocument23 pagesCEO Corner New Products Powerful Pocket SimulatorMOHAMMA MUSANo ratings yet
- ID Strategi Integrated Marketing Communication Imc Untuk Meningkatkan Loyalitas AngDocument17 pagesID Strategi Integrated Marketing Communication Imc Untuk Meningkatkan Loyalitas AngAiman AzhariNo ratings yet
- CV Jubilee Bubala Environmental SpecialistDocument4 pagesCV Jubilee Bubala Environmental SpecialistNomayi100% (2)
- Kristine Jane T. Zipagan Assignment: 1. Parts of InfographicsDocument2 pagesKristine Jane T. Zipagan Assignment: 1. Parts of InfographicsChristyNo ratings yet
- Australian Institute For Teaching and School Leadership - AITSLDocument5 pagesAustralian Institute For Teaching and School Leadership - AITSLYu LiNo ratings yet