You might also like
- Camp's Zoology by the Numbers: A comprehensive study guide in outline form for advanced biology courses, including AP, IB, DE, and college courses.From EverandCamp's Zoology by the Numbers: A comprehensive study guide in outline form for advanced biology courses, including AP, IB, DE, and college courses.No ratings yet
- 1.entamoeba Histolytica - Is The Major Pathogen in This GroupDocument14 pages1.entamoeba Histolytica - Is The Major Pathogen in This GroupJoseph De JoyaNo ratings yet
- Microbiology: a QuickStudy Laminated 6-Page Reference GuideFrom EverandMicrobiology: a QuickStudy Laminated 6-Page Reference GuideNo ratings yet
- The Intestinal ProtozoaDocument15 pagesThe Intestinal ProtozoaKHURT MICHAEL ANGELO TIUNo ratings yet
- Entamoeba SPPDocument21 pagesEntamoeba SPPragnabulletinNo ratings yet
- IntProt PDFDocument15 pagesIntProt PDFWasilla MahdaNo ratings yet
- Short Writing Assignment 3TDocument31 pagesShort Writing Assignment 3TTroi JeraoNo ratings yet
- Para Lec Lesson2Document9 pagesPara Lec Lesson2Tolentino, Edron E.No ratings yet
- Intestinal and Commensal AmoebaDocument9 pagesIntestinal and Commensal AmoebaFuture TrekingNo ratings yet
- Medical Parasitology Laboratory 1: EnrichmentDocument3 pagesMedical Parasitology Laboratory 1: EnrichmentVince RetutaNo ratings yet
- AmoebaDocument36 pagesAmoebaSarah BirechNo ratings yet
- (C-04) The AmoebasDocument24 pages(C-04) The AmoebasNick BatumbakalNo ratings yet
- XLSXDocument60 pagesXLSXLovely ReyesNo ratings yet
- Trichomonas VaginalisDocument2 pagesTrichomonas VaginalisAfnan ShaikhNo ratings yet
- (C-03) The FlagellatesDocument17 pages(C-03) The FlagellatesNick BatumbakalNo ratings yet
- Amoeba Notes 2015Document6 pagesAmoeba Notes 2015Ivy FlorentinoNo ratings yet
- Macabanding m5 Mt2h Subphylumsarcodina FlashcardsDocument56 pagesMacabanding m5 Mt2h Subphylumsarcodina FlashcardsNailah MacabandingNo ratings yet
- Genital, Intestinal, Oral FlagellaDocument7 pagesGenital, Intestinal, Oral Flagellaxofoh43003No ratings yet
- Medical ProtozoologyDocument6 pagesMedical ProtozoologyRaymund MontoyaNo ratings yet
- 2a - Macabanding, Princess - Mtclinpara Lec - Module 7 AssignmentDocument57 pages2a - Macabanding, Princess - Mtclinpara Lec - Module 7 AssignmentNailah MacabandingNo ratings yet
- Parasitology Chapter One Intestinal and Luminal ProtozoaDocument16 pagesParasitology Chapter One Intestinal and Luminal ProtozoajbfirthNo ratings yet
- محاضرة سادسة رابع نظريDocument7 pagesمحاضرة سادسة رابع نظريaust austNo ratings yet
- ProtozoaDocument28 pagesProtozoaFRANCESCA ALEXANDRIA PAREDESNo ratings yet
- EntamoebaDocument94 pagesEntamoebaAtlas AstreaNo ratings yet
- Unit 7 ActivityDocument5 pagesUnit 7 ActivityLeah SembranoNo ratings yet
- Lecture 5 6 - Microscopy AND LUMINAL PROTOZOANDocument54 pagesLecture 5 6 - Microscopy AND LUMINAL PROTOZOANNida RidzuanNo ratings yet
- Shifting Exams Reviewer For MEDTECH in ParasitologyDocument12 pagesShifting Exams Reviewer For MEDTECH in ParasitologyIwa RohasNo ratings yet
- CHAPTER 5 ParasitologyyDocument35 pagesCHAPTER 5 ParasitologyyMerlpa May AlcardeNo ratings yet
- CHAPTER 5 ParasitologyDocument57 pagesCHAPTER 5 ParasitologyKreizel FajaNo ratings yet
- Protozoa: Protozoan Means "First Animal"Document17 pagesProtozoa: Protozoan Means "First Animal"Mudit MisraNo ratings yet
- Protozoa Usus 2Document15 pagesProtozoa Usus 2Yoga NuswantoroNo ratings yet
- Life Cycle, Pathogenicity and Prophylaxis of Entamoeba HistolyticaDocument30 pagesLife Cycle, Pathogenicity and Prophylaxis of Entamoeba Histolyticabhavana mNo ratings yet
- Life Cycle and Infection Mode From Entamoeba HistolyticaDocument30 pagesLife Cycle and Infection Mode From Entamoeba HistolyticaSynthesis is What MattersNo ratings yet
- ProtozoaDocument132 pagesProtozoaAb AbNo ratings yet
- 4.handout No 4.intestinal ProtozoansDocument8 pages4.handout No 4.intestinal Protozoansfireshuja007No ratings yet
- ProtozologyDocument53 pagesProtozologybekib7092No ratings yet
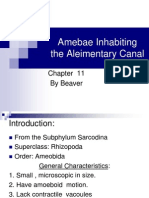
- Amebae Inhabiting The Aleimentary Canal: by BeaverDocument33 pagesAmebae Inhabiting The Aleimentary Canal: by BeaverDave OrlandoNo ratings yet
- Nonpathogenic Amoebae - FlagellatesDocument20 pagesNonpathogenic Amoebae - FlagellatesHend AtijaniNo ratings yet
- Chapter 3Document11 pagesChapter 3Mae CanlasNo ratings yet
- 2 Parasitology Parasitic AmoebasDocument8 pages2 Parasitology Parasitic AmoebasknkjnNo ratings yet
- CHAPTER 5 ParasitologyDocument35 pagesCHAPTER 5 ParasitologyMerlpa May AlcardeNo ratings yet
- Genus: Entamoeba Coli: Lecturer: Nerran K.F.AL-Rubaey Practical Parasites Lab - 2Document6 pagesGenus: Entamoeba Coli: Lecturer: Nerran K.F.AL-Rubaey Practical Parasites Lab - 2Chairut ChampoonoteNo ratings yet
- ProtozoansDocument20 pagesProtozoansRai AsdfghjklNo ratings yet
- Parasitic AmoebaDocument23 pagesParasitic AmoebaJethrö MallariNo ratings yet
- Amoebiasis ..ParasitologyDocument7 pagesAmoebiasis ..ParasitologyBenard NyaumaNo ratings yet
- Protozoology 1 - 06.11Document81 pagesProtozoology 1 - 06.11Manav VyasNo ratings yet
- Clinical Parasitology Lecture: The FlagellatesDocument18 pagesClinical Parasitology Lecture: The FlagellatesGyu KimNo ratings yet
- The Intestinal Protozoa: A. IntroductionDocument32 pagesThe Intestinal Protozoa: A. Introductionهاني عقيل حسين جوادNo ratings yet
- AmebaDocument53 pagesAmebaapi-19916399No ratings yet
- 7.0 FlagellatesDocument7 pages7.0 FlagellatesHenry KarokiNo ratings yet
- Para Protozoa Part2Document19 pagesPara Protozoa Part2BSMLS2AMERCADO ARJAYA.No ratings yet
- Parasitic Amoebas by Dr. C. J. Castro PDFDocument4 pagesParasitic Amoebas by Dr. C. J. Castro PDFMiguel CuevasNo ratings yet
- Protozoa: Protozoan Means "First Animal"Document6 pagesProtozoa: Protozoan Means "First Animal"Mudit MisraNo ratings yet
- BZ Lab 4.0Document7 pagesBZ Lab 4.0Alexa Jean D. HonrejasNo ratings yet
- ClinPara AmoebaDocument8 pagesClinPara AmoebaStephen YorNo ratings yet
- AmoebaDocument4 pagesAmoebaRichell VillacarlosNo ratings yet
- Entamoeba HistolyticaDocument10 pagesEntamoeba HistolyticamarkNo ratings yet
- Microbiology and Parasitology #2Document12 pagesMicrobiology and Parasitology #2Nurse TinNo ratings yet
- Reviewer in MicrobiologyDocument15 pagesReviewer in MicrobiologyRonel ResurricionNo ratings yet
- INDITA, Sherlyn Joy G - Activity 2Document3 pagesINDITA, Sherlyn Joy G - Activity 2Sherlyn Giban InditaNo ratings yet
- HistoPath (Lect #5) TransDocument5 pagesHistoPath (Lect #5) TransSherlyn Giban InditaNo ratings yet
- Parasitology (Lect #2) TransDocument2 pagesParasitology (Lect #2) TransSherlyn Giban InditaNo ratings yet
- Parasitology (Lect #4) TransDocument4 pagesParasitology (Lect #4) TransSherlyn Giban InditaNo ratings yet
- Parasitology (Lect #1) TransDocument2 pagesParasitology (Lect #1) TransSherlyn Giban InditaNo ratings yet
- HistoPath (Lect #4) TransDocument2 pagesHistoPath (Lect #4) TransSherlyn Giban InditaNo ratings yet
- Midterms in CEMDocument28 pagesMidterms in CEMSherlyn Giban InditaNo ratings yet
- Parasitology (Lect #5) TransDocument3 pagesParasitology (Lect #5) TransSherlyn Giban InditaNo ratings yet
- Assignment - Indita, Shaira Marie G.-Bsmt-1aDocument2 pagesAssignment - Indita, Shaira Marie G.-Bsmt-1aSherlyn Giban InditaNo ratings yet
- 12 STEM B Indita, Shaira Marie G. PEDocument1 page12 STEM B Indita, Shaira Marie G. PESherlyn Giban InditaNo ratings yet
- Assignment - Indita, Shaira Marie G.-Bsmt-1aDocument2 pagesAssignment - Indita, Shaira Marie G.-Bsmt-1aSherlyn Giban InditaNo ratings yet
- Shaira Marie Indita - ACTIVITY 2-THE SEXUAL SELFDocument4 pagesShaira Marie Indita - ACTIVITY 2-THE SEXUAL SELFSherlyn Giban InditaNo ratings yet
- DocumentDocument4 pagesDocumentSherlyn Giban InditaNo ratings yet
- La Consolacion University PhilippinesDocument1 pageLa Consolacion University PhilippinesSherlyn Giban InditaNo ratings yet
- Shaira Marie Indita - ACTIVITY 3 - MATERIAL SELFDocument4 pagesShaira Marie Indita - ACTIVITY 3 - MATERIAL SELFSherlyn Giban InditaNo ratings yet
- Shaira Marie Indita - ACTIVITY 3 - MATERIAL SELFDocument4 pagesShaira Marie Indita - ACTIVITY 3 - MATERIAL SELFSherlyn Giban InditaNo ratings yet
- As A Profession and Organize in A Scholarly Manner. Be Creative and ContemporaryDocument1 pageAs A Profession and Organize in A Scholarly Manner. Be Creative and ContemporarySherlyn Giban InditaNo ratings yet
- LongitudinalDocument1 pageLongitudinalSherlyn Giban InditaNo ratings yet
- Exercise #1 (Prelim)Document4 pagesExercise #1 (Prelim)Sherlyn Giban InditaNo ratings yet
- Background of The StudyDocument1 pageBackground of The StudySherlyn Giban InditaNo ratings yet
- 12 STEM B Indita, Shaira Marie G. (PERDEV, Module 7)Document5 pages12 STEM B Indita, Shaira Marie G. (PERDEV, Module 7)Sherlyn Giban InditaNo ratings yet
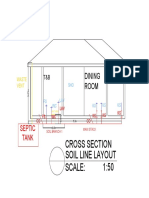
- Cross SectionDocument1 pageCross SectionSherlyn Giban InditaNo ratings yet
- Floor Plan Soil Line Layout Scale: 1:100: Dining Room Master'S BedroomDocument1 pageFloor Plan Soil Line Layout Scale: 1:100: Dining Room Master'S BedroomSherlyn Giban InditaNo ratings yet
- CH50Document88 pagesCH50ABIGAILNo ratings yet
- Immunology ModuleDocument42 pagesImmunology ModuleAhmed KerAtyNo ratings yet
- DocumentDocument15 pagesDocumentJennifer BanteNo ratings yet
- MC3 Microbiology and Parasitology NotesDocument15 pagesMC3 Microbiology and Parasitology NotesKim Erida QuezonNo ratings yet
- Hypersensitivity ReactionsDocument35 pagesHypersensitivity ReactionsFarlogy100% (1)
- Virus InfluenzaDocument6 pagesVirus InfluenzatiaNo ratings yet
- A Guide To The Application of The WHO Multimodal Hand Hygiene. OMS PDFDocument73 pagesA Guide To The Application of The WHO Multimodal Hand Hygiene. OMS PDFanon_157163700100% (1)
- Assignment 3: Stella ModelDocument9 pagesAssignment 3: Stella Modeld066915No ratings yet
- FCM Reviewer2Document6 pagesFCM Reviewer2Kim RamosNo ratings yet
- Laboratory #2 Pipetting Technique and Micropipette Calibration SkillsDocument151 pagesLaboratory #2 Pipetting Technique and Micropipette Calibration SkillsshimiNo ratings yet
- Title Perioperative Antibiotic Prophylaxis in Orthognathic SurgeryDocument80 pagesTitle Perioperative Antibiotic Prophylaxis in Orthognathic SurgeryKuriyan ArimboorNo ratings yet
- Heilsusálfræði GlósurDocument21 pagesHeilsusálfræði GlósurGuðrún Alma EinarsdóttirNo ratings yet
- (INS-SA-EN) Ichroma H.pylori SA - Rev02 - 180710Document3 pages(INS-SA-EN) Ichroma H.pylori SA - Rev02 - 180710nam7124119No ratings yet
- Course Syllabus Exam Micro paraDocument18 pagesCourse Syllabus Exam Micro paralanie_jecielNo ratings yet
- Disseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractDocument3 pagesDisseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractAmelia Fitria DewiNo ratings yet
- Main PDFDocument4 pagesMain PDFNadya Dwi PuspitasariNo ratings yet
- Cervical CancerDocument16 pagesCervical CancerChoi Gong JuNo ratings yet
- MastoiditisDocument5 pagesMastoiditisJessica Fredelina0% (1)
- Antibiotic Guidelines C Diff & PID Amended 05.08.11Document26 pagesAntibiotic Guidelines C Diff & PID Amended 05.08.11mikike13No ratings yet
- Garlic As QSI Capsule ProposalDocument5 pagesGarlic As QSI Capsule ProposalZerElie DavidNo ratings yet
- NDDB DMPDocument124 pagesNDDB DMPelanthamizhmaran100% (1)
- Ds Pedia WardDocument2 pagesDs Pedia WardRhea Mae Valles - ReyesNo ratings yet
- 2015 Proceeding - Management of The Patient With Canine Parvovirus EnteritisDocument7 pages2015 Proceeding - Management of The Patient With Canine Parvovirus EnteritisJHack2No ratings yet
- Guillian-Barre Syndrome: Renalyn Galache Gladys Gegare BSN-3BDocument18 pagesGuillian-Barre Syndrome: Renalyn Galache Gladys Gegare BSN-3BGLadys GegareNo ratings yet
- Nephrotic SyndromeDocument24 pagesNephrotic SyndromeSamah KhanNo ratings yet
- Continue: Sharma Mohan Textbook of Tuberculosis PDFDocument2 pagesContinue: Sharma Mohan Textbook of Tuberculosis PDFAbdul JalilNo ratings yet
- ACFrOgAonKUz7M07ncVvwi0s36nmp29y1ZhR F4h26u50OG7Z5 874dbSGQocVrZgk7OwxH7xBq1Y2LTn1odBH CbKFzhe8IzjrjTX0tUDLlp EyBEhjbxRLvuIQu3PvifBj9RRkpaZqCfLASbFLDocument1 pageACFrOgAonKUz7M07ncVvwi0s36nmp29y1ZhR F4h26u50OG7Z5 874dbSGQocVrZgk7OwxH7xBq1Y2LTn1odBH CbKFzhe8IzjrjTX0tUDLlp EyBEhjbxRLvuIQu3PvifBj9RRkpaZqCfLASbFLsagarnr gowdaNo ratings yet
- Celulitis PDFDocument9 pagesCelulitis PDFGazade GarciaNo ratings yet
- Naegleria FowleriDocument18 pagesNaegleria Fowlerij100% (1)
- BVSC & AH - SyllabusDocument36 pagesBVSC & AH - SyllabusAnomalous suriya addictzNo ratings yet