You might also like
- Email 101: Learn the BasicsDocument84 pagesEmail 101: Learn the BasicsCazan StelianNo ratings yet
- Modelling The Developing Mind PDFDocument77 pagesModelling The Developing Mind PDFAnca Mihaela VlasNo ratings yet
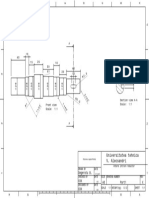
- Universitatea Tehnica V. Alecsandri: XXX X A3 Degeratu BDocument1 pageUniversitatea Tehnica V. Alecsandri: XXX X A3 Degeratu BCazan StelianNo ratings yet
- Universitatea Tehnica "Vasile Alecsandri": XXX A3 X Degeratu B. Roata DintataDocument1 pageUniversitatea Tehnica "Vasile Alecsandri": XXX A3 X Degeratu B. Roata DintataCazan StelianNo ratings yet
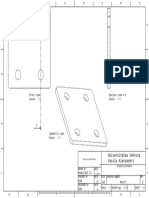
- Universitatea Tehnica Vasile Alecsandri: XXX X A3 Asavinei SDocument1 pageUniversitatea Tehnica Vasile Alecsandri: XXX X A3 Asavinei SCazan StelianNo ratings yet
- Universitatea Tehnica Vasile Alecsandri: XXX X A3 Asavinei SDocument1 pageUniversitatea Tehnica Vasile Alecsandri: XXX X A3 Asavinei SCazan StelianNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Prescribing Benzodiazepines GuidelineDocument4 pagesPrescribing Benzodiazepines GuidelineEfdio Manuel Joshiro SiagianNo ratings yet
- 00012244-201812000-00010 (Cog Anl The)Document19 pages00012244-201812000-00010 (Cog Anl The)mrt jchavarriaNo ratings yet
- HistrionicDocument13 pagesHistrionicAda FaurNo ratings yet
- Trauma-Sensitive Mindfulness: Practices For Safe and Transformative Healing - David A. TreleavenDocument5 pagesTrauma-Sensitive Mindfulness: Practices For Safe and Transformative Healing - David A. Treleavenryxeduzo0% (1)
- Zunkel Final Winter 21Document30 pagesZunkel Final Winter 21Raghabendra ShahNo ratings yet
- DOT PART 1 Criminology 3Document3 pagesDOT PART 1 Criminology 3WATI KAKINo ratings yet
- Extrapyramidal Symptoms Guide: Dystonia, Akathisia, Parkinsonism & Tardive DyskinesiaDocument35 pagesExtrapyramidal Symptoms Guide: Dystonia, Akathisia, Parkinsonism & Tardive DyskinesiaLucas PhiNo ratings yet
- Adult Needs and Strengths Assessment: ANSA ManualDocument39 pagesAdult Needs and Strengths Assessment: ANSA ManualAimee BethNo ratings yet
- Asian Journal of Psychiatry: Bharath Holla, Jagadisha ThirthalliDocument10 pagesAsian Journal of Psychiatry: Bharath Holla, Jagadisha ThirthalliFalon PapalangiNo ratings yet
- The Power of Music - Musical Therapy To Treat AutismDocument1 pageThe Power of Music - Musical Therapy To Treat AutismMuh EminNo ratings yet
- Patterns of BehaviorDocument8 pagesPatterns of BehaviorKeith AquinoNo ratings yet
- 1.7 Somatoform DisorderDocument6 pages1.7 Somatoform DisorderMark Christian CuiNo ratings yet
- Module 6 Facilitating Learner Centered TeachingDocument5 pagesModule 6 Facilitating Learner Centered TeachingTAMBAN VANESSANo ratings yet
- Case StudyDocument5 pagesCase StudyDerby Febriani SultanyNo ratings yet
- PsikopatologiDocument25 pagesPsikopatologiShella Thea WibawaNo ratings yet
- Welcome To Trucare Trust A Premium Alcohol & Drug Rehab CentreDocument5 pagesWelcome To Trucare Trust A Premium Alcohol & Drug Rehab CentreTrucare TrustNo ratings yet
- Personality Disorders Powerpoint MMCDocument220 pagesPersonality Disorders Powerpoint MMCEmilee Joice Rochelle Maluto100% (1)
- 384-File Utama Naskah-928-2-10-20210630Document19 pages384-File Utama Naskah-928-2-10-20210630Jeremia TogatoropNo ratings yet
- Drug AwarenessDocument3 pagesDrug AwarenessJay cool swaggerNo ratings yet
- Clinical Psychology ReportDocument8 pagesClinical Psychology ReportJoe SoulageNo ratings yet
- IJCM-Psychoses in MangaloreDocument2 pagesIJCM-Psychoses in MangaloreANKUR BARUANo ratings yet
- What Is Suicide?: National Institute of Mental Health (NIMH)Document4 pagesWhat Is Suicide?: National Institute of Mental Health (NIMH)Raissa DeaNo ratings yet
- DSM-5 and Neurocognitive DisordersDocument6 pagesDSM-5 and Neurocognitive DisordersluishelNo ratings yet
- Treatment Manuals For Cognitive Behavioural Therapy and Applied Relaxation Msword 136335277Document3 pagesTreatment Manuals For Cognitive Behavioural Therapy and Applied Relaxation Msword 136335277anasonicNo ratings yet
- Stress vs Anxiety: What's the Key DifferenceDocument1 pageStress vs Anxiety: What's the Key Differencerahma watiNo ratings yet
- Suicidal Ideation Risk Assessment: Steps and Resources For Exploring Thoughts of SuicideDocument12 pagesSuicidal Ideation Risk Assessment: Steps and Resources For Exploring Thoughts of SuicideShreeya GhagNo ratings yet
- MSE DepressionDocument3 pagesMSE DepressionSam Raven AndresNo ratings yet
- What Are Amphetamines?Document4 pagesWhat Are Amphetamines?Asmaa LabibNo ratings yet
- Schizophrenia BiopsihosocialDocument401 pagesSchizophrenia BiopsihosocialPetzyMarian100% (1)
- DSM-IV-TR Somatoform and Factitious Disorders OverviewDocument33 pagesDSM-IV-TR Somatoform and Factitious Disorders OverviewNoelle Grace Ulep Baroman100% (1)