You might also like
- Wireless Public Safety Networks Volume 1: Overview and ChallengesFrom EverandWireless Public Safety Networks Volume 1: Overview and ChallengesNo ratings yet
- Disaster and Emergency ManagementDocument11 pagesDisaster and Emergency Managementsanket.visputeNo ratings yet
- Disaster ManagementDocument12 pagesDisaster ManagementharpreetNo ratings yet
- Topic: Disaster Management: Definitions 1. Disaster As "Any Occurrence That Causes DamageDocument16 pagesTopic: Disaster Management: Definitions 1. Disaster As "Any Occurrence That Causes DamageSharika sasiNo ratings yet
- Disaster - Mangt IVDocument15 pagesDisaster - Mangt IVDeepti KukretiNo ratings yet
- 14 - DR. S.K Haldar MAHC 3Document70 pages14 - DR. S.K Haldar MAHC 3Ashan SanNo ratings yet
- Telephone No. 333-2273/ 260-0543/ 260-5782 Email AddressDocument10 pagesTelephone No. 333-2273/ 260-0543/ 260-5782 Email AddressCHARIEMAE CA�AZARESNo ratings yet
- Disaster ManagementDocument12 pagesDisaster ManagementAnusha Verghese100% (5)
- Guidance Notes: Emergency and Disaster Preparedness For Health FacilitiesDocument56 pagesGuidance Notes: Emergency and Disaster Preparedness For Health FacilitiesMarky RoqueNo ratings yet
- Activity DisasterDocument3 pagesActivity DisasterElle MongeNo ratings yet
- Disaster Risk Reduction Management LectureDocument19 pagesDisaster Risk Reduction Management LectureJames Joseph ObispoNo ratings yet
- An Evaluation of Hospital Evacuation Strategies With An ExampleDocument14 pagesAn Evaluation of Hospital Evacuation Strategies With An ExamplezamriNo ratings yet
- Disaster MedicineDocument38 pagesDisaster MedicineFazil KfNo ratings yet
- 3-The Risk of Doing An Autopsy and High-Risk AutopsiesDocument8 pages3-The Risk of Doing An Autopsy and High-Risk Autopsiestherese_ticNo ratings yet
- Assignment On Disaster Management: School of Management Studies, Punjabi University, PatialaDocument13 pagesAssignment On Disaster Management: School of Management Studies, Punjabi University, PatialaKawalpreet Singh MakkarNo ratings yet
- NarrativeDocument4 pagesNarrativeCheryl GetongoNo ratings yet
- EMERGENCY AND DISASTER MANAGEMENT Unit 3Document12 pagesEMERGENCY AND DISASTER MANAGEMENT Unit 3Aparna KinginiNo ratings yet
- FL Proteksi Kebakaran & Simulasi Bencana RSDocument37 pagesFL Proteksi Kebakaran & Simulasi Bencana RSKartika SyantiqNo ratings yet
- DisasterDocument6 pagesDisasterSakthi DeviNo ratings yet
- Full Text 01Document11 pagesFull Text 01Badica PetreNo ratings yet
- Air Change - ASHRAEDocument5 pagesAir Change - ASHRAETeo Pei SanNo ratings yet
- Des 4 ResearchDocument8 pagesDes 4 ResearchMary Rose MinguilloNo ratings yet
- Edit Ur RSW in Design 7Document15 pagesEdit Ur RSW in Design 7Architect MamongNo ratings yet
- Disaster NursingDocument9 pagesDisaster NursingTwinkleNo ratings yet
- Massive Casualty ManagementDocument48 pagesMassive Casualty Managementsuleiman adamuNo ratings yet
- Clinical Casuality ManagementDocument6 pagesClinical Casuality ManagementswathiprasadNo ratings yet
- Disaster Management Planning1Document11 pagesDisaster Management Planning1amita chaudhari100% (1)
- 4 Safety and Precautions During Gas Leakage From Plant EventsDocument4 pages4 Safety and Precautions During Gas Leakage From Plant EventsMattupalli pardhuNo ratings yet
- UnitDP2018 RedactedDocument11 pagesUnitDP2018 Redactedcharas marabilloNo ratings yet
- Case Study2 (Fire Safety) OSHADocument18 pagesCase Study2 (Fire Safety) OSHAHazreen HazwanyNo ratings yet
- The Assessment of Fire Safety Evacuation Management at The General Hospital Pulau PinangDocument21 pagesThe Assessment of Fire Safety Evacuation Management at The General Hospital Pulau PinangIzzati ZohadiNo ratings yet
- University: Adama Science and TechnologyDocument23 pagesUniversity: Adama Science and TechnologyTesfuGebreslassieNo ratings yet
- Review of Fi Ve London Hospital Fi Res and Their Management: January 2008 - February 2009Document23 pagesReview of Fi Ve London Hospital Fi Res and Their Management: January 2008 - February 2009Herlina AlianasNo ratings yet
- Healthcare Facility Preparedness in DisasterDocument16 pagesHealthcare Facility Preparedness in DisasterydtrgnNo ratings yet
- Man MadeDocument10 pagesMan MadeRakesh KumarNo ratings yet
- Republic of Moldova Hospital Safety Assessment Report: National Center For Disaster MedicineDocument27 pagesRepublic of Moldova Hospital Safety Assessment Report: National Center For Disaster MedicinecoleaNo ratings yet
- Disaster Answer KeyDocument6 pagesDisaster Answer KeyjananipriyaNo ratings yet
- Hospital Emergency Management PlanDocument5 pagesHospital Emergency Management PlandedefreddyNo ratings yet
- Medical Devices Handling, Environmental SafetyDocument37 pagesMedical Devices Handling, Environmental SafetyGnanasaravanan 2508No ratings yet
- Project Study and Architectural ProgrammingDocument25 pagesProject Study and Architectural ProgrammingChelsea ManiponNo ratings yet
- The Basic Protocol Ic Guidelines For The Dental Service DH 2009Document40 pagesThe Basic Protocol Ic Guidelines For The Dental Service DH 2009MuthiaraPrazianditeNo ratings yet
- Part C Ali Hashemi OSHA Group AssignmentDocument29 pagesPart C Ali Hashemi OSHA Group AssignmentAli HashemiNo ratings yet
- 1 s2.0 S2352012415000417 MainDocument14 pages1 s2.0 S2352012415000417 MainCarl Hadrian LimNo ratings yet
- Emergency Procedure Manual: Kulhavi HallDocument41 pagesEmergency Procedure Manual: Kulhavi HallKatamba RogersNo ratings yet
- King Institute of Preventive Medicine and Research, Guindy, Chennai-600 032, Tamil Nadu, IndiaDocument5 pagesKing Institute of Preventive Medicine and Research, Guindy, Chennai-600 032, Tamil Nadu, IndiaJULIANINo ratings yet
- Hospital Impact Immediate IssuesDocument18 pagesHospital Impact Immediate IssuesydtrgnNo ratings yet
- Lunch Symposium Dr. Fanny Indarto, SPB - Multiple vs. Mass Casualties ManagementDocument17 pagesLunch Symposium Dr. Fanny Indarto, SPB - Multiple vs. Mass Casualties ManagementThomas Kwee100% (1)
- Earth Quake Risk AssessmentDocument11 pagesEarth Quake Risk Assessmentamdarrif3723No ratings yet
- Mass Casualty Incident Management Awareness Level Student Manual 1 EditionDocument253 pagesMass Casualty Incident Management Awareness Level Student Manual 1 EditionJO HN Scuba-rNo ratings yet
- Presentation 2024.4.11Document11 pagesPresentation 2024.4.11arch.anupNo ratings yet
- Mayur EstDocument12 pagesMayur EstRavindra SalunkheNo ratings yet
- SST HeehDocument12 pagesSST HeehSmamanNo ratings yet
- Post Disaster MitigationDocument8 pagesPost Disaster Mitigationadnan qadirNo ratings yet
- Emergency Planning and Preparedness - On-Site & Off-SiteDocument17 pagesEmergency Planning and Preparedness - On-Site & Off-SiteDebasis MishraNo ratings yet
- Manalo, Gio Aldrin O. Research For Design 5Document15 pagesManalo, Gio Aldrin O. Research For Design 5Ysha GlorianiNo ratings yet
- Guidelines & Main Requirements in The Planning and Design of Hospitals-Part IIDocument7 pagesGuidelines & Main Requirements in The Planning and Design of Hospitals-Part IIElie SalibaNo ratings yet
- Unit - 5 Disaster ManagementDocument46 pagesUnit - 5 Disaster ManagementAravind RajNo ratings yet
- ERP For Company Covering All SitesDocument7 pagesERP For Company Covering All SitesDarius DsouzaNo ratings yet
- Emergencypreparedness Unit - 5 PDFDocument39 pagesEmergencypreparedness Unit - 5 PDFDhruvKharbanda100% (1)
- An Unexpected Presentation of A Traumatic Wound On The Lower Lip: A CaseDocument5 pagesAn Unexpected Presentation of A Traumatic Wound On The Lower Lip: A CaseAnonymous jfqzCfcI4ENo ratings yet
- Midterm International Economics 2023Document4 pagesMidterm International Economics 2023Nhi Nguyễn YếnNo ratings yet
- frdA190220A1421665 PDFDocument2 pagesfrdA190220A1421665 PDFVeritaserumNo ratings yet
- 43-Assignment-Business Studies Class Xii WorksheetsDocument81 pages43-Assignment-Business Studies Class Xii WorksheetsvinayakkanchalNo ratings yet
- MCom - Accounts ch-13 Topic3Document19 pagesMCom - Accounts ch-13 Topic3Sameer GoyalNo ratings yet
- Epiforce: Protecting Personal InformationDocument4 pagesEpiforce: Protecting Personal InformationLuke TerringtonNo ratings yet
- Slip Gaji (3)Document2 pagesSlip Gaji (3)Olele Olala50% (2)
- Certificado EGT 20000 MAX G2Document4 pagesCertificado EGT 20000 MAX G2Diego PionaNo ratings yet
- LEGAL ETHICS. Canon 2Document27 pagesLEGAL ETHICS. Canon 25h1tfac3No ratings yet
- Working With Words Language at WorkDocument2 pagesWorking With Words Language at WorkercabamaNo ratings yet
- CBSE Class 7 Social Science Sample Paper SET - 1: Time: 3 Hours Max. Marks: 80Document4 pagesCBSE Class 7 Social Science Sample Paper SET - 1: Time: 3 Hours Max. Marks: 80Gopi SNo ratings yet
- Use Case: From Wikipedia, The Free EncyclopediaDocument6 pagesUse Case: From Wikipedia, The Free EncyclopediaLisset Garcia PerezNo ratings yet
- SM SX 52 SpecificatonDocument2 pagesSM SX 52 SpecificatonAli HussnainNo ratings yet
- Cambridge IGCSE™: Business Studies 0450/11Document23 pagesCambridge IGCSE™: Business Studies 0450/11eulalialamNo ratings yet
- MQ1 1Document1 pageMQ1 1shaira alliah de castroNo ratings yet
- Formate of Business LetterDocument14 pagesFormate of Business LetterMuhammad Hamdan AfridiNo ratings yet
- PKGS Shipping BillDocument2 pagesPKGS Shipping BillAjay DarlingNo ratings yet
- Lahore School of Economics Financial Management I Time Value of Money - 3 Assignment 4Document2 pagesLahore School of Economics Financial Management I Time Value of Money - 3 Assignment 4Ahmed ZafarNo ratings yet
- This Study Resource WasDocument2 pagesThis Study Resource WasAron Rabino ManaloNo ratings yet
- DIVYA VISHWAKARMA Construction IndustryDocument87 pagesDIVYA VISHWAKARMA Construction IndustryNITISH CHANDRA PANDEYNo ratings yet
- Global Marketing DjarumDocument20 pagesGlobal Marketing DjarumcindyoclNo ratings yet
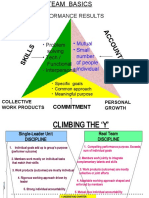
- Team BasicsDocument3 pagesTeam BasicsSoumya Jyoti BhattacharyaNo ratings yet
- Practice Question (Accounting Cycle) With Solution v2Document17 pagesPractice Question (Accounting Cycle) With Solution v2Laiba ManzoorNo ratings yet
- CSEC POB June 2017 P2 PDFDocument16 pagesCSEC POB June 2017 P2 PDFDarcel Brown100% (1)
- Assignment of Contract (Correct Version)Document2 pagesAssignment of Contract (Correct Version)Heru Atiba El - BeyNo ratings yet
- A Project On Marketing Mix Coca ColaDocument67 pagesA Project On Marketing Mix Coca ColaShagun VermaNo ratings yet
- Tax Invoice: Invoice Issued For FlightDocument2 pagesTax Invoice: Invoice Issued For FlightManab HalderNo ratings yet
- The Star SydneyDocument12 pagesThe Star SydneyKLIOMARIE ANNE CURUGANNo ratings yet
- Guide To SQL 9th Edition by Pratt Last Solution ManualDocument13 pagesGuide To SQL 9th Edition by Pratt Last Solution Manualcatherinebergtjkxfanwod100% (25)
- Part 2-Essential Management Functions Chapter V. Organizing Business ActivitiesDocument13 pagesPart 2-Essential Management Functions Chapter V. Organizing Business ActivitiesEunice CatubayNo ratings yet
- Senville CertificateDocument1 pageSenville Certificateha6127176No ratings yet
- How to Lead: Wisdom from the World's Greatest CEOs, Founders, and Game ChangersFrom EverandHow to Lead: Wisdom from the World's Greatest CEOs, Founders, and Game ChangersRating: 4.5 out of 5 stars4.5/5 (95)
- The First Minute: How to start conversations that get resultsFrom EverandThe First Minute: How to start conversations that get resultsRating: 4.5 out of 5 stars4.5/5 (57)
- The Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverFrom EverandThe Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverRating: 4.5 out of 5 stars4.5/5 (186)
- How to Talk to Anyone at Work: 72 Little Tricks for Big Success Communicating on the JobFrom EverandHow to Talk to Anyone at Work: 72 Little Tricks for Big Success Communicating on the JobRating: 4.5 out of 5 stars4.5/5 (36)
- Scaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0From EverandScaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0Rating: 5 out of 5 stars5/5 (1)
- The Power of People Skills: How to Eliminate 90% of Your HR Problems and Dramatically Increase Team and Company Morale and PerformanceFrom EverandThe Power of People Skills: How to Eliminate 90% of Your HR Problems and Dramatically Increase Team and Company Morale and PerformanceRating: 5 out of 5 stars5/5 (22)
- The 7 Habits of Highly Effective PeopleFrom EverandThe 7 Habits of Highly Effective PeopleRating: 4 out of 5 stars4/5 (2564)
- Spark: How to Lead Yourself and Others to Greater SuccessFrom EverandSpark: How to Lead Yourself and Others to Greater SuccessRating: 4.5 out of 5 stars4.5/5 (131)
- Billion Dollar Lessons: What You Can Learn from the Most Inexcusable Business Failures of the Last Twenty-five YearsFrom EverandBillion Dollar Lessons: What You Can Learn from the Most Inexcusable Business Failures of the Last Twenty-five YearsRating: 4.5 out of 5 stars4.5/5 (52)
- Transformed: Moving to the Product Operating ModelFrom EverandTransformed: Moving to the Product Operating ModelRating: 4 out of 5 stars4/5 (1)
- Transformed: Moving to the Product Operating ModelFrom EverandTransformed: Moving to the Product Operating ModelRating: 4 out of 5 stars4/5 (1)
- 25 Ways to Win with People: How to Make Others Feel Like a Million BucksFrom Everand25 Ways to Win with People: How to Make Others Feel Like a Million BucksRating: 5 out of 5 stars5/5 (36)
- Work the System: The Simple Mechanics of Making More and Working Less (4th Edition)From EverandWork the System: The Simple Mechanics of Making More and Working Less (4th Edition)Rating: 4.5 out of 5 stars4.5/5 (23)
- Only the Paranoid Survive: How to Exploit the Crisis Points That Challenge Every CompanyFrom EverandOnly the Paranoid Survive: How to Exploit the Crisis Points That Challenge Every CompanyRating: 3.5 out of 5 stars3.5/5 (122)
- The 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsFrom EverandThe 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsRating: 4.5 out of 5 stars4.5/5 (411)
- Trillion Dollar Coach: The Leadership Playbook of Silicon Valley's Bill CampbellFrom EverandTrillion Dollar Coach: The Leadership Playbook of Silicon Valley's Bill CampbellRating: 4.5 out of 5 stars4.5/5 (626)
- The 7 Habits of Highly Effective People: 30th Anniversary EditionFrom EverandThe 7 Habits of Highly Effective People: 30th Anniversary EditionRating: 5 out of 5 stars5/5 (337)
- Unlocking Potential: 7 Coaching Skills That Transform Individuals, Teams, & OrganizationsFrom EverandUnlocking Potential: 7 Coaching Skills That Transform Individuals, Teams, & OrganizationsRating: 4.5 out of 5 stars4.5/5 (28)
- Work Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkFrom EverandWork Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkRating: 4.5 out of 5 stars4.5/5 (12)
- The Introverted Leader: Building on Your Quiet StrengthFrom EverandThe Introverted Leader: Building on Your Quiet StrengthRating: 4.5 out of 5 stars4.5/5 (35)
- The Lean Product Playbook: How to Innovate with Minimum Viable Products and Rapid Customer FeedbackFrom EverandThe Lean Product Playbook: How to Innovate with Minimum Viable Products and Rapid Customer FeedbackRating: 4.5 out of 5 stars4.5/5 (81)
- Radical Candor by Kim Scott - Book Summary: Be A Kickass Boss Without Losing Your HumanityFrom EverandRadical Candor by Kim Scott - Book Summary: Be A Kickass Boss Without Losing Your HumanityRating: 4.5 out of 5 stars4.5/5 (40)
- The Friction Project: How Smart Leaders Make the Right Things Easier and the Wrong Things HarderFrom EverandThe Friction Project: How Smart Leaders Make the Right Things Easier and the Wrong Things HarderNo ratings yet
- The 4 Disciplines of Execution: Revised and Updated: Achieving Your Wildly Important GoalsFrom EverandThe 4 Disciplines of Execution: Revised and Updated: Achieving Your Wildly Important GoalsRating: 4.5 out of 5 stars4.5/5 (48)
- The E-Myth Revisited: Why Most Small Businesses Don't Work andFrom EverandThe E-Myth Revisited: Why Most Small Businesses Don't Work andRating: 4.5 out of 5 stars4.5/5 (709)