You might also like
- 5t4bvrfke3xuqspihwrir0d1Document6 pages5t4bvrfke3xuqspihwrir0d1Vishesh Mahendru20% (5)
- Capstone Paper An Evaluation of The Bioterror ThreatDocument14 pagesCapstone Paper An Evaluation of The Bioterror Threatapi-395576671No ratings yet
- Biological DisastersDocument9 pagesBiological Disasterskisna120967% (3)
- Bioterrorism and Intelligence PDFDocument11 pagesBioterrorism and Intelligence PDFIbs Júnior100% (1)
- Medical Officer KPJ Pasir Gudang Specialist Hospital Jalan Persiaran Dahlia 2, 81700 Pasir GudangDocument1 pageMedical Officer KPJ Pasir Gudang Specialist Hospital Jalan Persiaran Dahlia 2, 81700 Pasir GudangNooh DinNo ratings yet
- Bioterrorism - A Public Health Perspective-DikonversiDocument9 pagesBioterrorism - A Public Health Perspective-DikonversiFira LasenaNo ratings yet
- Bioterrorism: A Public Health Perspective: Contemproary IssueDocument6 pagesBioterrorism: A Public Health Perspective: Contemproary IssueThenej EnabagNo ratings yet
- India's Preparedness Against Bioterrorism: Biodefence Strategies and Policy MeasuresDocument8 pagesIndia's Preparedness Against Bioterrorism: Biodefence Strategies and Policy Measuresshiva karnatiNo ratings yet
- Bioweapons-A Review: Karan Singh Negi Shivani Govt. Mohindra College, Patiala (Punjab) - 147001 November 2018Document13 pagesBioweapons-A Review: Karan Singh Negi Shivani Govt. Mohindra College, Patiala (Punjab) - 147001 November 2018Karan NegiNo ratings yet
- Presented By: Dr. Timiresh Kumar Das Moderator: Dr. Anita Verma Associate Professor Dept. of Community MedicineDocument87 pagesPresented By: Dr. Timiresh Kumar Das Moderator: Dr. Anita Verma Associate Professor Dept. of Community MedicinePrerit AggarwalNo ratings yet
- Bioterorism and Inteligence1Document8 pagesBioterorism and Inteligence1Moch Arief SetiawanNo ratings yet
- Bio TerrorismDocument202 pagesBio TerrorismJosé RamírezNo ratings yet
- 7bioterrorism Noah 2012Document4 pages7bioterrorism Noah 2012Aaron SolatorioNo ratings yet
- 1 s20 S1473309918302986 Main-2Document12 pages1 s20 S1473309918302986 Main-2Jorge aguilar francesNo ratings yet
- Disec 1Document17 pagesDisec 1Anastasia SopikiotiNo ratings yet
- What Are The Biological Agents That Can Be Utilized For Bioterrorism?Document30 pagesWhat Are The Biological Agents That Can Be Utilized For Bioterrorism?anukriti shrivastavaNo ratings yet
- b28113433 PDFDocument202 pagesb28113433 PDFJuthika GogoiNo ratings yet
- Overview On Mechanisms of Antibacterial Resistance: Alemayehu Toma, Serawit DeynoDocument10 pagesOverview On Mechanisms of Antibacterial Resistance: Alemayehu Toma, Serawit DeynowaelNo ratings yet
- On Farm BiosecurityDocument26 pagesOn Farm BiosecurityAvskilt MazidNo ratings yet
- Martens and Demain - , 2017 - The AntibiotiDocument7 pagesMartens and Demain - , 2017 - The AntibiotiJavier CastroNo ratings yet
- Disease or Bio-Warfare? The Usage of Various Pathogens in BioterrorismDocument4 pagesDisease or Bio-Warfare? The Usage of Various Pathogens in BioterrorisminventionjournalsNo ratings yet
- BioterrorismDocument26 pagesBioterrorismotherswork.000No ratings yet
- Biological Toxins As The Potential Tools For Bioterrorism: Molecular SciencesDocument18 pagesBiological Toxins As The Potential Tools For Bioterrorism: Molecular SciencesGirgis CristianNo ratings yet
- Emerging and Reemerging Infectious DiseasesDocument13 pagesEmerging and Reemerging Infectious DiseasesSayu100% (1)
- Antifungal Drugs - The Current Armamentarium and Development of New AgentsDocument20 pagesAntifungal Drugs - The Current Armamentarium and Development of New AgentssovalaxNo ratings yet
- Disaster - Case StudyDocument5 pagesDisaster - Case StudyShyam DasNo ratings yet
- Bioterrorism: Law Enforcement, Public Health & Role of Oral and Maxillofacial Surgeon in Emergency PreparednessDocument7 pagesBioterrorism: Law Enforcement, Public Health & Role of Oral and Maxillofacial Surgeon in Emergency Preparednessnurul khoriahNo ratings yet
- LitreviewDocument7 pagesLitreviewapi-395576671No ratings yet
- 2004, Vol.22, Issues 3, BioterrorismDocument104 pages2004, Vol.22, Issues 3, BioterrorismRizweta DestinNo ratings yet
- Bio TerrorismDocument31 pagesBio TerrorismPallavi Shrivastava VedNo ratings yet
- The History of Biological WarfareDocument4 pagesThe History of Biological WarfareMaika Ysabelle RavaloNo ratings yet
- Biological HazardDocument15 pagesBiological HazardRoshan Ouseph100% (1)
- 1 Running Head: BIOTERRORISMDocument12 pages1 Running Head: BIOTERRORISMapi-348988299No ratings yet
- Bio 1 Lecture Sdjacinto Institute of Biology, University of The Philippines, DilimanDocument35 pagesBio 1 Lecture Sdjacinto Institute of Biology, University of The Philippines, DilimanfebrinarizkNo ratings yet
- Biological Warfare, Bioterrorism, Biodefence and The Biological and Toxin Weapons ConventionDocument31 pagesBiological Warfare, Bioterrorism, Biodefence and The Biological and Toxin Weapons ConventionMarco R PaguiriganNo ratings yet
- Infectious Disease and Bioterrorism: (George Johnson, Washington University, St. Louis)Document14 pagesInfectious Disease and Bioterrorism: (George Johnson, Washington University, St. Louis)namahNo ratings yet
- Biological Warfare: Learn What's at Risk, Protective Measures & Treatment of Casualties (Bacterial Agents; Anthrax, Brucellosis, Plague, Q Fever, Viral Agents; Smallpox, Venezuelan Equine Encephalitis, Toxins…)From EverandBiological Warfare: Learn What's at Risk, Protective Measures & Treatment of Casualties (Bacterial Agents; Anthrax, Brucellosis, Plague, Q Fever, Viral Agents; Smallpox, Venezuelan Equine Encephalitis, Toxins…)No ratings yet
- Chapter 6Document42 pagesChapter 6Murali AmirthalingamNo ratings yet
- The Weapon Potential of A Microbe: Arturo Casadevall and Liise-Anne PirofskiDocument5 pagesThe Weapon Potential of A Microbe: Arturo Casadevall and Liise-Anne PirofskiWenshan LuoNo ratings yet
- Advantages N Disadvantages Biological WeaponDocument13 pagesAdvantages N Disadvantages Biological Weaponpaspologen50% (2)
- Handout 13 Biotechnology in Promoting Law and Order PDFDocument36 pagesHandout 13 Biotechnology in Promoting Law and Order PDFMiccah Angela Parreño FraynaNo ratings yet
- Health and EnvironmentDocument7 pagesHealth and Environmentm-8992844No ratings yet
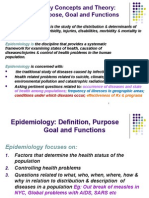
- Concepts Theory EpidemiologyDocument48 pagesConcepts Theory EpidemiologyStephanie Wong100% (1)
- Coco MarvinDocument3 pagesCoco MarvinssucbotNo ratings yet
- Bioterrorism in Latin AmericaDocument4 pagesBioterrorism in Latin AmericaErick InsuastiNo ratings yet
- Biological Warfare Agents: AnthraxDocument4 pagesBiological Warfare Agents: AnthraxVevin MozaNo ratings yet
- Animals Causing Infectious Disease - A Brief Review Vijayasankari A, Kalpana SDocument4 pagesAnimals Causing Infectious Disease - A Brief Review Vijayasankari A, Kalpana Snithish krishnaNo ratings yet
- Bioterrorism PP TDocument153 pagesBioterrorism PP TIvkoNo ratings yet
- Emerging Antibiotic Resistance in Bacteria With Special Reference To IndiaDocument11 pagesEmerging Antibiotic Resistance in Bacteria With Special Reference To IndiaDrSagar GrNo ratings yet
- Microbial Bioterrorism ProofDocument8 pagesMicrobial Bioterrorism Proofdr.umar shareefNo ratings yet
- Biological ArmsDocument27 pagesBiological ArmsadolfoarreolaNo ratings yet
- Microbial Forensics: Application To Bioterrorism Preparedness and ResponseDocument19 pagesMicrobial Forensics: Application To Bioterrorism Preparedness and ResponseMajedalNo ratings yet
- Essay Antibiotics FinalDocument6 pagesEssay Antibiotics FinalAmber TeacherNo ratings yet
- (Hans Zinsser, 1934 Quoted in Murphy 1994)Document43 pages(Hans Zinsser, 1934 Quoted in Murphy 1994)Saad MotawéaNo ratings yet
- Current Medicine Research and Practice: Tulsi ChughDocument2 pagesCurrent Medicine Research and Practice: Tulsi ChughhadrilkaNo ratings yet
- Biological Terrorism For RJDocument30 pagesBiological Terrorism For RJRoberto FortuNo ratings yet
- Pahomi Article BSA2023Document11 pagesPahomi Article BSA2023Madalina Ionela PahomiNo ratings yet
- Part 9: Terrorism and Clinical Medicine: Microbial BioterrorismDocument27 pagesPart 9: Terrorism and Clinical Medicine: Microbial Bioterrorismjonas100% (1)
- Preparacion Hospitalaria para Evento QBRN IRANDocument5 pagesPreparacion Hospitalaria para Evento QBRN IRANCVOED Nivel CentralNo ratings yet
- Okumura1998 PDFDocument7 pagesOkumura1998 PDFTriveniNo ratings yet
- Rodgers 1998Document5 pagesRodgers 1998CVOED Nivel CentralNo ratings yet
- Okumura1998 Experiencia de TokyoDocument5 pagesOkumura1998 Experiencia de TokyoCVOED Nivel CentralNo ratings yet
- Liberacion de SustanciasDocument22 pagesLiberacion de SustanciasCVOED Nivel CentralNo ratings yet
- Preparacion Hospitalaria JAMADocument8 pagesPreparacion Hospitalaria JAMACVOED Nivel CentralNo ratings yet
- GuideDocument296 pagesGuideCVOED Nivel CentralNo ratings yet
- Food Borne Diseases - 0Document131 pagesFood Borne Diseases - 0Nur FithriahNo ratings yet
- (PDF) Influence of TORCH Infections in First Trimester Miscarriage in The Malabar Region of KeralaDocument16 pages(PDF) Influence of TORCH Infections in First Trimester Miscarriage in The Malabar Region of KeralaleartaNo ratings yet
- HEALTH EDUCATION - GroupB - 2BDocument3 pagesHEALTH EDUCATION - GroupB - 2BKyle FernandezNo ratings yet
- Mda Palakkad 2016 NewDocument33 pagesMda Palakkad 2016 NewAasifKNazarNo ratings yet
- Oral MedicineDocument4 pagesOral MedicineRizki Dwi LestariNo ratings yet
- Trichomonas Rapid Test: CLIA Complexity: WaivedDocument8 pagesTrichomonas Rapid Test: CLIA Complexity: WaivedRabecca TobingNo ratings yet
- CDS - Scrub TyphusDocument17 pagesCDS - Scrub TyphuskirustagyNo ratings yet
- Outline On Dengue Fever - EDITEDDocument2 pagesOutline On Dengue Fever - EDITEDDavid Skeat0% (1)
- Leprosy and Leprosy ProgramDocument26 pagesLeprosy and Leprosy ProgramAnne LeeNo ratings yet
- Wuchereria BancroftiDocument46 pagesWuchereria BancroftiSolomon Fallah Foa SandyNo ratings yet
- Week 4: Part 1 Notes MBP 108 Lecture Medical and Surgical Asepsis Learning ObjectivesDocument7 pagesWeek 4: Part 1 Notes MBP 108 Lecture Medical and Surgical Asepsis Learning Objectivesthe someoneNo ratings yet
- Systemic MycosesDocument12 pagesSystemic Mycosesdrunken monkeyNo ratings yet
- Poultry Medication: Product Indication Composition Reg No G979 G1305Document1 pagePoultry Medication: Product Indication Composition Reg No G979 G1305irfan syuhadaNo ratings yet
- 387-Article Text-900-1-10-20190714Document5 pages387-Article Text-900-1-10-20190714Ftri RhmnNo ratings yet
- Performance Task #111 & 2 EappDocument3 pagesPerformance Task #111 & 2 EappEricka Rivera SantosNo ratings yet
- Sexually Transmitted Diseases - Part 1: DR Clarissa ListerDocument20 pagesSexually Transmitted Diseases - Part 1: DR Clarissa Listerandreas kevinNo ratings yet
- CroupDocument40 pagesCroupAbigail Basco100% (1)
- Blood Bank 2Document21 pagesBlood Bank 2moonfire2009No ratings yet
- Community Acquired PneumoniaDocument4 pagesCommunity Acquired PneumoniaKenPedreso100% (2)
- Rekap - Klaim-5d9c153e1f403Document108 pagesRekap - Klaim-5d9c153e1f403Yulianti NurNo ratings yet
- Virus Web WorksheetDocument3 pagesVirus Web WorksheetBrian Ramirez RamirezNo ratings yet
- 08-0923 FinaldDocument5 pages08-0923 FinaldAndri YansyahNo ratings yet
- Black Death ReportDocument2 pagesBlack Death ReportArthur YanNo ratings yet
- National Tuberculosis Program: Valenzuela City Accomplishment 2018-2019-2020Document43 pagesNational Tuberculosis Program: Valenzuela City Accomplishment 2018-2019-2020JohnPhilipTiongcoNo ratings yet
- HerpesDocument2 pagesHerpesSyafruddin GBNo ratings yet
- DM No. 2020-0405 Interim Guidelines On The Tagging of Suspect, Probable, and Confirmed COVID-19 CasesDocument7 pagesDM No. 2020-0405 Interim Guidelines On The Tagging of Suspect, Probable, and Confirmed COVID-19 CasesZero Toribio MellaNo ratings yet
- Precautions - Isolation Precautions - Guidelines Library - Infection Control - CDCDocument6 pagesPrecautions - Isolation Precautions - Guidelines Library - Infection Control - CDCKomite PPI RSUDPCNo ratings yet
- Hiv AidsDocument18 pagesHiv AidsK EV INNo ratings yet