
Professional Documents
Culture Documents
Preparacion Hospitalaria JAMA
Uploaded by
CVOED Nivel CentralCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Preparacion Hospitalaria JAMA
Uploaded by
CVOED Nivel CentralCopyright:
Available Formats
SPECIAL COMMUNICATION
Weapons of Mass Destruction Events
With Contaminated Casualties
Effective Planning for Health Care Facilities
Anthony G. Macintyre, MD
Biological and chemical terrorism is a growing concern for the emergency
Lt Col George W. Christopher, USAF, MC preparedness community. While health care facilities (HCFs) are an essen-
COL Edward Eitzen, Jr, MC, USA tial component of the emergency response system, at present they are poorly
prepared for such incidents. The greatest challenge for HCFs may be the sud-
LTC Robert Gum, MC, USA
den presentation of large numbers of contaminated individuals. Guidelines
Scott Weir, MD for managing contaminated patients have been based on traditional haz-
Craig DeAtley, PA-C ardous material response or military experience, neither of which is directly
CDR Kevin Tonat, DrPH, MPH, USPHS applicable to the civilian HCF. We discuss HCF planning for terrorist events
that expose large numbers of people to contamination. Key elements of an
Joseph A. Barbera, MD effective HCF response plan include prompt recognition of the incident, staff
and facility protection, patient decontamination and triage, medical therapy,
T
HE PERCEIVED THREAT OF
chemical or biological weap- and coordination with external emergency response and public health agen-
ons directed against the US ci- cies. Controversial aspects include the optimal choice of personal protective
vilian population has in- equipment, establishment of patient decontamination procedures, the role of
creased substantially.1-3 The designation chemical and biological agent detectors, and potential environmental im-
of these weapons, along with nuclear ma- pacts on water treatment systems. These and other areas require further in-
terials and high explosives, as “weap- vestigation to improve response strategies.
JAMA. 2000;283:242-249 www.jama.com
ons of mass destruction” emphasizes
their potential catastrophic effect on the
exposed persons. Such a response must transportation to the HCF unassisted by
health of a large population. Compre-
be coordinated within the entire com- emergency medical services (EMS).5
hensive communitywide management
munity response framework, as in the in- These patients will not have undergone
programs for civilians exposed to chemi-
cident command system, the most widely triage or decontamination, and the least
cal or biological warfare agents are still
accepted command and control model injured will often present first. The HCF
under development and many response
for emergency response in the United must have the ability to immediately de-
issues have not been fully addressed.
States.4 Events that are likely to chal- contaminate and treat those who are ill
Health care facilities (HCFs) are an in-
lenge the decontamination capability of from the agent.6 Some persons may have
tegral yet often overlooked component
a HCF include 2 types of worst-case sce-
of the overall community response.
narios, chemical and biological. Author Affiliations: Institute for Crisis, Disaster and
Although response requirements dif-
With the release of a chemical weapon Risk Management (Dr Barbera) and Department of
fer for chemical and biological agent re- Emergency Medicine (Drs Macintyre and Weir and Mr
in a populated area, casualties may pre-
leases, in both cases there might be situ- DeAtley), George Washington University Medical Cen-
sent en masse with little or no advance ter, Washington, DC; US Army Medical Research In-
ations necessitating the removal of the stitute of Infectious Diseases, Fort Detrick, Md (Lt Col
notification.Thechemicalagentdeployed
agent from exposed individuals Christopher and COL Eitzen); US Army Center for
could be a traditional militarized agent Health Promotion and Preventive Medicine—
(decontamination). We discuss the plan- Europe, Landstuhl Army Regional Medical Center,
(such as the vesicant mustard) or a more
ning of an effective HCF response to in- Landstuhl, Germany (LTC Gum); and the Office of
readily obtainable industrial hazardous Emergency Preparedness, US Public Health Service,
cidents that require decontamination of
material. As shown in the Tokyo sarin at- Rockville, Md (CDR Tonat).
Corresponding Author and Reprints: Anthony G.
tack, a significant number of exposed in- Macintyre, MD, 2140 Pennsylvania Ave NW, Wash-
For editorial comment see p 252.
dividuals may find their own means of ington, DC 20037 (e-mail: emdagm@gwumc.edu).
242 JAMA, January 12, 2000—Vol 283, No. 2 ©2000 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a SWINBURNE UNIVERSITY OF TECHNOLOGY User on 05/18/2015
PLANNING FOR WEAPONS OF MASS DESTRUCTION EVENTS
experienced very little exposure to the The unintentional release of milita- have also disrupted communities across
agent, or none at all. They may still re- rized chemical agents from US military the country.33
quire decontamination because exposure depots has been another civilian con-
cannot be ruled out. Symptoms may be cern. In response, a major prepared- CURRENT CAPABILITY
accompanied by anxiety and may be di- ness initiative, the Chemical Stockpile As the potential threat of civilian expo-
verse and confusing.5,7 Residual chemi- Emergency Preparedness Program, has sure increases, the new challenge for the
cal agents on those exposed may pose a been implemented in communities sur- medical emergency response community
risk of secondary spread to the HCF and rounding the depots.21 The response sys- will be managing contaminated mass ca-
its workers by contact or vaporization.8,9 tem has never been activated.22 No simi- sualties, some of whom may be ill. Many
In a biological attack, an infectious lar community preparedness program for HCFs are poorly prepared for the decon-
agent may be released surreptitiously and biological release has been developed, tamination requirements of even small-
discovered after the incubation period, since the US military ceased maintain- scale HAZMAT incidents,34,35 as demon-
when patients present with illness. How- ing biological weapons in 1972.23,24 strated by the temporary closures of well-
ever, if a biological attack is announced The newly perceived threat entails run, full-service emergency departments
or discovered publicly as it is occur- the deliberate use of chemical and bio- after presentation of only 1 or 2 contami-
ring, it could result in large numbers of logical weapons against civilians. In nated patients in 1997.36 The most com-
patients suddenly presenting for ser- many instances, these weapons are rela- prehensive HCF response plans to date
vices. In contrast with chemical agents, tively easy to produce, inexpensive, and were designed to cope with specific in-
most biological agents (except mycotox- can be deployed covertly. Most signifi- dividualchemicalorbiologicalagentsand
ins) are not dermally active or volatile. cantly, the widespread terror caused by radioactive nucleotides.37
Reaerosolization of infectious particles the use of these weapons could com- Development of HCF response plans
is theorized to be a low but possible risk.10 plicate response needs.25,26 has been hampered by many factors.
Therefore, decontamination to lessen the The toxic and psychological threats Foremost is the lack of civilian experi-
effects of primary exposure and to pre- posed by chemical terrorism were dem- ence with mass casualty events of a
vent secondary exposure is less impor- onstrated by the 1995 sarin attack in the chemical or biological nature. Many civil-
tant than with chemical agents, but may Tokyo subway system.5,27 The assault re- ian plans are derived from the experi-
be necessary.11,12 The procedure could be sulted in 11 deaths and more than 5000 ences of prehospital HAZMAT response
as simple as taking a shower and chang- emergency medical evaluations, of which teams or military defense procedures that
ing clothes (exposure to mycotoxins 73.9% had no identifiable clinical in- may not be appropriate.
would call for procedures similar to those jury.28 The majority of those exposed ap- The HAZMAT approach assumes that
used for chemical agents, including ex- parently had either a subclinical expo- responders will enter a highly toxic en-
tensive patient decontamination).13 A sure or psychogenic symptoms. No vironment near the source of release
sudden biological event may require ad- chemical attacks of this nature have been (away from an HCF). Maximum protec-
ministration of prophylactic medica- reported in the United States. tion is provided for a few workers rescu-
tions and vaccines and could place ex- No successful biological attack has ing a small number of patients, usually
traordinary demands on medical and occurred in the United States with an without time pressure for decontamina-
public health staff and facilities.14-16 We aerosolized agent, but other crimes and tion. The primary objectives are scene
do not address the epidemiological in- hoaxes involving biological agents have containment and environmental protec-
vestigation and large-scale measures occurred.29-31 The potential psychologi- tion. In line with these assumptions, the
needed to control infection in the event cal effects of bioterrorism were dem- Occupational Health and Safety Admin-
a mass exposure to infectious agents is onstrated by the 1997 B’nai B’rith inci- istration (OSHA) has mandated the use
recognized in a delayed fashion. Plans dent in Washington, DC.32 A Petri dish of a “Personal Protection Level based
for HCF response to these types of found in the mail room of the B’nai B’rith upon site hazards.”38 However, site haz-
events are under development.11,17 headquarters was labeled to indicate the ards are more easily defined at the point
presence of Bacillus anthracis and of release than at the HCF, where patient
BACKGROUND Yersinia pestis. Responders and inci- care is conducted. Thus, current OSHA
Until recently, any threat to civilians dent managers were unaware that guidelinesmaybeinappropriateforHCFs.
from hazardous materials (HAZMATs) nonaerosolized, agar-based organisms Traditional HAZMAT products, such as
primarily has come from industrial pose no inhalation or cutaneous expo- decontamination tents, trailers, and iso-
events.18 While unintentional releases are sure hazard (it was later proven that nei- lation rooms, are expensive, require pro-
relatively common, they generally cause ther organism was present). As a result, longed setup time, or are inadequate for
few serious toxic exposures per event.19 an expensive scene-control operation large numbers of patients.39
HAZMAT response guidelines have been took place, causing fear and inconve- Military countermeasures for chemi-
developed and implemented for man- nience among those potentially ex- cal and biological weapons are also inap-
aging these incidents.20 posed. Other recent biological hoaxes propriate for civilian use without modi-
©2000 American Medical Association. All rights reserved. JAMA, January 12, 2000—Vol 283, No. 2 243
Downloaded From: http://jama.jamanetwork.com/ by a SWINBURNE UNIVERSITY OF TECHNOLOGY User on 05/18/2015
PLANNING FOR WEAPONS OF MASS DESTRUCTION EVENTS
fication.Militarypersonnelareamoreho- The federal government has estab- the HCF is receiving patients but is not
mogenous population, generally phy- lished a National Domestic Prepared- within the primary release area). Oth-
sically fit, mentally disciplined, and eq- ness Office (NDPO) under the aus- erwise, facility evacuation or “shelter-
uippedforchemicalwarfare.Becausethey pices of the Department of Justice to act ing in place” may be indicated. Key
are designed for operations in very toxic as a clearing house during responses to components of the model prepared-
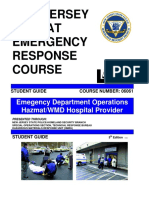
environments,militarycontingencyplans domestic chemical and biological ter- ness plan are illustrated in the FIGURE.
can be complex.40 Incorrect civilian use rorist incidents. The NDPO will handle
of military protective equipment and de- information pertinent to law enforce- Event Recognition
contamination procedures may be haz- ment, emergency medical response, In an unannounced event, it is essen-
ardous, as with the use of military-style medical, and public health sectors. tial to recognize contaminated patients
gas masks by Israeli civilians during Gulf Federal preparedness initiatives have before their entrance into the facility. Se-
War missile attacks. Fatalities resulted been paralleled by private industry’s de- curity personnel must be trained in early
from improper mask use.41,42 velopment of chemical and biological recognition and should be stationed at
The US government has recently be- agent response products and training the hospital entrances. Security person-
gun addressing civilian preparedness programs. Self-described expert con- nel should immediately notify manage-
deficits. A 1995 presidential initiative sultant groups offer risk analysis and ment personnel when they suspect a
funded the prototype for Metropolitan training for various components of lo- problem, and they should be prepared
MedicalStrikeTeams,43 whichwerecom- cal emergency response, including to protect themselves by donning per-
posed of specially trained local person- HCFs. Some programs market equip- sonnel protective equipment (PPE).
nel were organized to help communities ment packages supplied by vendors Even so, it is reasonable to expect some
respond to events. This effort has been working in conjunction with the con- contaminated individuals may gain en-
revised to include a systems approach sultants.49 Most offer operational guide- trance into the facility. These situa-
and has been renamed Metropolitan lines based on traditional HAZMAT tions should be handled on a case-by-
Medical Response Systems (MMRS). The procedures. As yet, no published large- case basis with a rational approach. It
overall goal of the MMRS program is to scale exercise or response experience will not be necessary to completely seal
link first-response, public health, and has validated these programs. off the facility or a department in most
health care systems. As a component of circumstances.50
the MMRS, HCFs will remain respon- PROPOSED HCF CONCEPT
sible for initial management of contami- OF OPERATIONS Activation of Plan
nated patients. To date, 47 urban areas Owing to the complexity of a civilian The alert mechanism should be expe-
have received funding for development event involving chemical or biological ditious: PPE must be immediately acces-
of an MMRS and more communities are weapons, HCFs should begin by delin- sible to decontamination and patient
expected to receive similar support. eating priorities that guide their pre- care personnel, and the decontamina-
The Nunn-Lugar-Domenici congres- paredness process. These objectives tion facility should be operational within
sional legislation allocated federal funds should be established in coordination 2 to 3 minutes.
to the Department of Defense to upgrade with the other members of the com-
the capabilities of civilian first respond- munity involved in emergency re- Management
ers, including HCF personnel.44 This Do- sponse. The priorities of the HCF could The principles of the incident com-
mesticPreparednessProgramisbeingcon- be ranked in this order: (1) protection mand system should be incorporated
ducted serially in 120 metropolitan areas of the current patients, staff, and facil- into the HCF’s emergency prepared-
by the US Army Soldier and Biological ity; (2) provision of the best possible ness plan.51 The use of this system will
Chemical Command.45 This program is medical care for contaminated pa- enable HCF staff to fully integrate their
intendedtoprovideoperational-levelpre- tients presenting to the institution for activities with community emergency re-
paredness,witheducationaltractsforcom- care; and (3) environmental protec- sponse assets, since it is widely used by
munityresponseentities,includingemer- tion external to the HCF. In a large- fire, EMS, and police personnel as well
gencymanagement,lawenforcement,fire, scale event, containment of wastewa- as many state and federal agencies. Al-
and medical personnel. The current pro- ter will probably be impossible, though though initial response efforts will be
gramforhospitalpersonnelhaslackedde- no consensus has yet been reached on centered in the decontamination and
tailed operational methods.46,47 A large- this controversial point. This issue treatment areas, other HCF depart-
scalechemicalagentexerciseinNewYork should be addressed through compre- ments will play vital roles. For in-
City, conducted after hospital personnel hensive planning that includes local en- stance, security officers must direct the
hadparticipatedintheDomesticPrepared- vironmental and water authorities. flow of casualties and vehicles to pre-
ness Program, demonstrated that hospi- Certain assumptions can be made to vent facility compromise and must
tals would still have difficulty managing simplify planning. One is that the ex- prevent unauthorized access to the de-
patient decontamination.48 posure site is remote from the HCF (ie, contamination and treatment areas.
244 JAMA, January 12, 2000—Vol 283, No. 2 ©2000 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a SWINBURNE UNIVERSITY OF TECHNOLOGY User on 05/18/2015
PLANNING FOR WEAPONS OF MASS DESTRUCTION EVENTS
Personnel from departments including nated, they may be handled by staff us- tially requiring medical intervention will
emergency, critical care services, plant ing universal precaution guidelines. be assigned to medical decontamina-
operations, pharmacy, supply services, Crowd control will require firm, au- tion by staff.
infectious disease, respiratory therapy, thoritative direction from hospital se- Throughout the decontamination
laboratory, and toxicology must be tar- curity and, if available, police or the Na- process, attention must be given to
geted for education and training in the tional Guard. Since PPE face masks symptoms of exposure to chemical or
response plan. muffle the voice, loudspeakers should biological agents that may indicate early
A widespread chemical or biological be provided to personnel directing con- life-threatening deterioration (eg, a sore
incident will result in extended opera- taminated patients. Signs designating throat or mild shortness of breath af-
tional periods. Staff should be coordi- functional areas and providing patient ter exposure to pulmonary or laryn-
nated to provide relief from physically instructions should be in place. geal irritants).
taxing activities such as patient decon-
tamination. Providing food and hydra- Primary Triage Patient Sign-in/Identification
tion in a hygienic manner will enhance All exposed and potentially exposed in- and Securing Property
staff performance. Psychological sup- dividuals should receive an initial brief A brief sign-in process should capture
port for staff should be available. triage, performed by medical personnel name and date of birth (full registration
Personnel caring for contaminated pa- in PPE, before decontamination. They can occur after decontamination and
tients should be properly outfitted in should then be directed to 1 of 2 areas, should be consistent with the commu-
PPE. Specific data to determine the ap- nonmedical decontamination or medi- nity patient tracking system). A num-
propriate level of hospital worker pro- cal decontamination. The uninjured, ber on a log can be assigned to each pa-
tection remains limited, and a recent ex- those with minor injuries requiring no tient, who would receive 2 identically
tensive review on chemical and biologi- medical intervention during decontami- numbered plastic bags and a nonperme-
cal terrorism published by the Institute nation, and the majority of ambulatory able wristband. Clothing would be placed
of Medicine is inconclusive on this patients will be assigned to nonmedical into the larger clear, impervious bag.
issue.52 Level C PPE consists of a non- decontamination. These individuals may Separation of valuables into the second,
encapsulated, chemical-resistant suit, require nonmedical assistance with smaller bag would enhance the security
gloves, and boots, with a full-face air pu- washing themselves (eg, unaccompa- of these items. A meticulous, practical
rifier cartridge mask (powered or non- nied children, persons in wheelchairs, method of cataloging belongings will en-
powered). This gear should afford ad- and those with other special needs). sure their return and possibly assist in
equate respiratory protection for out- Those with injuries or illness poten- forensic investigations.
door exposure to contaminated chemi-
cal casualties who have survived trans- Figure. Health Care Facility Response Plan for Chemical or Biological Weapons Release
port to the HCF.21,53 For HCF workers
conducting decontamination of patients Event Recognition
acutelycontaminatedwithinfectiousbio-
logical agents, level D protection (stan- Activation of Plan
dard work clothes) plus latex gloves, eye
Prepare Staff, Decontamination,
splash protection, and N-95 respiratory and Treatment Areas and Initiate
masks (used in many hospitals for pro- Plans for Crowd Control
tection against tuberculosis) should be Minor or No Apparent Moderate and Major
Injury or Illness Injury or Illness
adequate.54,55 If responders are concerned
Primary
about reaerosolizing an agent during Nonmedical Decontamination Triage Medical Decontamination
clothing removal, a high-efficiency par-
ticulate air (HEPA) filter mask could be
added. If the agent class for a sudden re- Patient Sign-in Identify Patient (If Possible)
lease cannot be identified, level C PPE Emergency Treatment
Patient Disrobes Patient Disrobed
with an organic vapor/HEPA filter car- Initiated as Needed
tridge mask is recommended. Patient Decontamination Patient Decontaminated
Training is essential for the correct use
of PPE. Work times and conditions must
be monitored while personnel are us-
Minor or No Apparent Major and Moderate
ing PPE to prevent fatigue or heat stress. Injury or Illness Injury or Illness
Secondary
Personnel should be rotated if decon- Triage
tamination operations are prolonged. Holding Area Treatment Areas
Once patients have been decontami-
©2000 American Medical Association. All rights reserved. JAMA, January 12, 2000—Vol 283, No. 2 245
Downloaded From: http://jama.jamanetwork.com/ by a SWINBURNE UNIVERSITY OF TECHNOLOGY User on 05/18/2015
PLANNING FOR WEAPONS OF MASS DESTRUCTION EVENTS
Patient Decontamination promising overall flow. Patients whose long-term surveillance program to
The HCF should possess partially fixed clinical condition deteriorates in the de- monitor possible health effects.
or preconstructed decontamination fa- contamination line can impede the
cilities that can be activated immedi- progress of others. Plans must include Logistics for Treatment
ately. This facility should be designed to means for sidetracking these patients Specific therapies for chemical and bio-
occupy little storage space and not dis- into an area separate from the main de- logical agent casualties vary according to
rupt routine operations while in use. The contamination sites, where treatment the etiologic agent and are described else-
Israeli model, developed during the Gulf can be initiated. where.15,16,60,61 Mass casualties requir-
War, consists of showers permanently Decontamination can be accom- ing specific chemical antidotes, vaccina-
fixed to the ceiling structure of an open- plished by using a sequential copious tions, or antibiotics will quickly deplete
air parking garage or the side of a build- warm water rinse, a hypoallergenic liq- available supplies. In most cases, cur-
ing.56 The George Washington Univer- uid soap wash, another warm water rinse, rent hospital stocks of medications would
sity Hospital model uses fire exit and then a final rinse after walking past be inadequate to meet the needs of even
alleyways. An outdoor decontamina- other in-use showers. Incapacitated pa- a few of these patients.62 Several efforts
tion facility can prevent entry of con- tients will require soap and water cleans- are under way to address this problem,
taminants into the HCF and obviates ing by staff, with attention to washing including a federal initiative to stock-
dedicating space with room ventilation and rinsing the patient’s back and the pile antibiotics and vaccines.63 Other con-
and vapor isolation. An outdoor facil- nonabsorbent backboard. The water tem- cerns have not yet been adequately ad-
ity is also more suitable for the influx of perature must be adjustable. Exces- dressed. After a smallpox release, for
mass casualties. Outdoor decontamina- sively warm water should be avoided, as example, postexposure vaccination
tion, however, must offer protection this may promote peripheral vasodila- might be indicated, but smallpox vac-
from inclement weather and have ad- tation and toxin absorption. Stiff brushes cine is no longer produced and current
equate lighting for night operations. or abrasives should also be avoided as stocks are limited.16,64
Because clothing will be removed be- they may enhance dermal absorption of Otherwise straightforward medical
fore decontamination, privacy must be the toxin and can produce skin lesions problems, including eye injuries, bron-
protected to ensure compliance with that may be mistaken for chemical inju- chospasm, and burns, may also need
full decontamination. The sexes should ries.58,59 Sponges and disposable towels mass intervention. Ventilators and other
be separated, with a visual barrier be- are affordable and effective alternatives. critical care supplies may be needed in
tween shower lines. The need for pro- large quantities. This problem could be
tection of privacy was demonstrated by Secondary Triage resolved in part through mutual aid
a successful lawsuit against a fire de- Persons with major or moderate casu- agreements between HCFs. Such an
partment whose personnel decontami- alties would be referred to treatment ar- agreement established in the Washing-
nated 2 women without ensuring ad- eas designated for such cases. Those ton, DC, area provides for pooling of
equate privacy.57 with minor or no apparent injuries resources (including personnel, sup-
Another important consideration is should be sent to a holding area for fur- plies, and equipment), and sharing of
rapid patient progression through the ther evaluation, observation, and even- information.65 Contingency plans of this
decontamination process. Traditional tual treatment if needed. type may be vital to saving lives, since
HAZMAT decontamination is passive time constraints prevent reliance on re-
(using 2 responders to clean each pa- Holding Area supply support from state and federal
tient), which is time consuming and un- Large spaces such as cafeterias or au- agencies during the initial crucial pe-
necessary for the majority of ambula- ditoriums can be used for observation riod of an event.
tory patients in the nonmedical de- of large numbers of patients with mi-
contamination area. Promoting pa- nor or no apparent injuries and ill- Epidemiological Considerations
tient self-decontamination will signifi- nesses by physicians and nurses. At this Health care facility involvement will ex-
cantly decrease the required number of time, HCF staff should also provide in- tend beyond the treatment of patients
health care workers. Of course, de- formation on the agent involved, po- who are acutely ill or exposed. A com-
contamination assistance for some pa- tential short- and long-term effects, rec- prehensive community response will in-
tients in the nonmedical decontamina- ommended treatment, stress reactions, clude epidemiological analysis under-
tion area and full passive decon- and possible avenues to further assis- taken by local and national public
tamination in the medical decontami- tance. It is essential to provide impor- health organizations to identify all po-
nation area must still be available. tant information in writing because the tential exposed individuals. This should
Decontamination facilities should memory of patients may be impaired by be done during the brief interval when
contain multiple shower stations that the psychological stress of dealing with early intervention can save lives and
are designed to allow patients to an exposure. All potentially exposed in- containment can reduce secondary
progress at various rates without com- dividuals should also be enrolled in a transmission of contagious agents. Such
246 JAMA, January 12, 2000—Vol 283, No. 2 ©2000 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a SWINBURNE UNIVERSITY OF TECHNOLOGY User on 05/18/2015
PLANNING FOR WEAPONS OF MASS DESTRUCTION EVENTS
analysis will require participation by staff should also have access to formal- nal air source (hose-supplied air with an
HCFs. ized stress debriefing at a later date. escape cylinder or a self-contained air
Because injuries and illnesses sus- tank).70 However, these reports do not
Information Resources tained during the response would be cov- mention whether higher levels of pro-
Health care facility personnel must ered under employee compensation in- tection produce a quantified increase in
identify sources of expert information surance, all staff members involved safety, nor do they discuss the possible
on chemical and biological agents to en- should be registered in a health surveil- disadvantages such as additional cost,
sure ready access to such information. lance program. This will ensure that weight, and training requirements.
Ideally, a repository or data bank could medical issues will receive proper atten- Choosing a specific material to pro-
be established at the community or na- tion, and demonstrate the HCFs com- vide chemical barrier protection for HCF
tional level. This would allow for the mitment to employee health. In view of personnel is difficult. Many types of
distribution of uniform information. the possible delayed or chronic effects of chemically resistant suits are available.
Other resources include medical some chemical agents, surveillance could They vary in cost and each has unique
management handbooks developed by continue for years. Assistance for this properties.71 Industrywide testing is
the US Army’s chemical and biologi- type of surveillance is available through based on permeation rates of pure sub-
cal defense medical laboratories.54,60,61 the Agency for Toxic Substances and Dis- stances directly applied to the material,
Some civilian-based protocols, such as ease Registry, which the US Depart- but such data may not be relevant to the
pediatric recommendations, have also ment of Health and Human Services has exposure in the HCF response model.72
been established; these are currently be- identified as the lead agency for the reg- Health care workers remote from the im-
ing revised by the US Public Health Ser- istration of personnel exposed to chemi- pact site or incident scene will be ex-
vice. 66 Consensus statements orga- cal or biological warfare agents.67 posed only to the agent that remains on
nized by the Working Group on It will be essential to clean the de- the skin and clothing of those exposed,
Civilian Biodefense also provide use- contamination facilities and process the so concentrations of substances encoun-
ful guidance.15,16 Consultation is also possessions of contaminated patients, tered during decontamination at the
available 24 hours a day by remote ac- as well as dispose of solid waste. HCF will be more dilute than concen-
cess through the National Response Cleanup will be guided by the specific trations used for the testing PPE mate-
Center at (800) 424-8802. agent involved and the law enforce- rials.68 Less expensive barrier materials
ment investigation. If no adequate, fi- may therefore be adequate.
Public Information nancially viable method is available to
Prompt attention must be given to in- inactivate a highly toxic, persistent Decontamination Solution
formation issued to the public through agent such as the nerve gas VX, assis- Another controversial concept con-
the news media and bulletins. Media in- tance may be required from other lo- cerns patient decontamination. Should
quiries must be carefully handled, and cal, state, or federal entities.68 decontamination be simplified by es-
the content of these communications tablishing a universal process for all in-
should be discussed with appropriate CONTROVERSIES AND cidents, as suggested by Cox?71 Some
emergency management authorities to RESEARCH REQUIRED authors have already published univer-
prevent the release of conflicting or er- sal decontamination protocols for
roneous reports. Personal Protective Equipment chemical exposures.50 There is little ar-
One major question concerns the opti- gument that soap and water will be ef-
Postincident Actions mal approach to PPE. To simplify guide- fective for most agents. In the past, an
Following the event, HCF manage- lines and reduce confusion about the agent neutralizer such as a 0.5% solu-
ment should conduct an incident re- variety of choices, PPE recommenda- tion of hypochlorite was recom-
view with hospital personnel involved tions could be standardized. This mea- mended. It inactivates biological agents
in the emergency response. The pur- sure would ease financial disincentives (except mycotoxins) and, at a slower
pose of such a review is to determine, as well as training requirements. rate, chemical agents such as mustard
in a nonpejorative manner, the se- Although published research on and organophosphates.13,60,61 The stud-
quence of events and to disseminate the adequacy of PPE is limited, the consen- ies indicate, however, that 15 to 20 min-
rationale behind controversial deci- sus emerging among researchers and utes of contact time is necessary for hy-
sions. Exposure risks and necessary medical planners is that level C protec- drolysis or oxidation and, thus, for the
countermeasures should be discussed tion (using a full-face mask with pow- inactivation of chemical agents.60 Fur-
to alleviate some of the psychological ered or nonpowered canister filtration thermore, dilute bleach can cause tis-
impact of incident stress. The incident system) is adequate for HCF work- sue damage in open wounds, exposed
critique, which will take place later, is ers.21,68,69 A few reports recommend a nerve tissue, and the eyes.13,73 The lack
a technical review designed to evalu- higher level of protection, level B, which of clear safety and efficacy data for
ate and improve the response plan. The includes a mask supplied by an exter- bleach decontamination suggests that
©2000 American Medical Association. All rights reserved. JAMA, January 12, 2000—Vol 283, No. 2 247
Downloaded From: http://jama.jamanetwork.com/ by a SWINBURNE UNIVERSITY OF TECHNOLOGY User on 05/18/2015
PLANNING FOR WEAPONS OF MASS DESTRUCTION EVENTS
it should be avoided, especially if soap reaerosolization.10,13 On the other hand, by contaminated patients presenting to
and water are immediately available. a large-scale chemical incident usually HCFs) that cannot be safely washed into
There may be rare exceptions to a uni- results in significant environmental pol- public water runoff?
versal decontamination process. For in- lution; the amount of agent borne by pa-
stance, pure metals and strong corro- tients presenting to HCFs will consti- CONCLUSION
sives require dry decontamination (ie, tute only a small fraction of the total The threat of a large-scale incident in-
gentle brushing or vacuuming of larger environmental burden. Some authors volving intentional release of chemi-
particles) before water is applied.68,74 suggest that as much as 75% to 90% of cal or biological agents in the United
the hazardous agent may be removed by States is significant, but currently, no
Agent Detectors disrobing.70,71,75 The remaining skin con- practical models exist for HCF re-
Yet another controversial issue is what taminant may be minuscule and can be sponse to a suddenly recognized event
role agent detectors should play in an diluted further during washing and pass- requiring the decontamination of mass
HCF response plan. Agent detectors and ing into public wastewater systems. The casualties. The time has come to estab-
monitors are used in the military and installation of a large-volume wastewa- lish a forum of experts to address the
HAZMAT/EMS arenas. In the HCF en- ter containment system is a prohibi- questions presented in this article and
vironment, however, they would only tively expensive undertaking. Even if elsewhere and to reach a consensus on
complicate and lengthen the decontami- installed, the final disposition of waste- how to develop and disseminate com-
nation process. Much of the monitor- water containing hazardous materials prehensive guidelines for HCFs. These
ing and detection equipment for chemi- can be a catastrophic financial burden. solutions should be fully integrated into
cal and biological agents is expensive and If the facility design does not provide the community response plan for
training intensive. Even handheld as- wastewater containment, appropriate chemical or biological terrorism.
says require attention to standard pro- water authorities should be notified at Precedence for this consensus ap-
tocols. Moreover, some agent detectors the time of the event. proach may be found in the method used
can give false-positive readings when by the Federal Emergency Manage-
perfume, diesel vapors, or nonthreaten- Unanswered Questions ment Agency for the creation of the Na-
ing contaminants are present.75 In some These and other pressing questions tional Urban Search and Rescue Sys-
cases, cool air, the presence of a non- must be investigated if research is to tem.76 Above all, the process must be an
militarized agent, or other factors can help improve response strategies: operationally oriented cooperative ef-
produce false-negative results. Detec- • What are the actual risks to first re- fort and remain uninfluenced by finan-
tion can also be time consuming. If an sponders, clinicians, and other health cial gain and unproved technologies.
HCF is operating without any means of care workers from reaerosolizing bio- The threat posed by chemical and
detection, HCF personnel must con- logical agents on contaminated cloth- biological terrorism must be kept in
sider that most biological agents and ing, skin, or environmental surfaces? proper perspective. Disaster prepar-
some selected chemical toxins (eg, mus- • What is the minimum adequate edness plans must maintain readiness
tard) have delayed clinical manifesta- amount of washing/rinsing time re- for these events as well as the terrorist
tions. Contingency plans must include quired for adequate decontamination use of conventional explosives.77,78 Ac-
the capability to treat potentially ex- from most agents? cidental HAZMAT exposures remain
posed persons, if indicated, while con- • What are the specific limitations of even more likely. Robust, effective HCF
firmatory tests are under way. level C and level B PPE for HCF per- preparedness integrated with local com-
sonnel caring for exposed patients re- munity planning will help address the
Decontamination Wastewater moved from a site where a chemical or more conventional threats.
Questions have also been raised about a biological agent has been released? Disclaimer: The opinions and findings in this article
the potential environmental impact of • What are the ideal avenues through are those of the authors and should not be construed
releasing decontamination wastewater which HCFs can disseminate informa- as official policies or positions of the US Department
of the Army, US Department of the Air Force, US Pub-
into the water treatment system. To date, tion during an event of this type or mag- lic Health Service, or US government.
the Environmental Protection Agency nitude?
has not published an official statement • What equipment and training re- REFERENCES
on this issue in relation to HCF plan- quirements can HCFs realistically sup- 1. US Congress, Office of Technology Assessment.
ning. The decision not to contain waste- port for this preparedness? Should pub- Proliferation of Weapons of Mass Destruction:
Assessing the Risks. Washington, DC: US Govern-
water can be justified for most agents in lic policy provide funding for HCF ment Printing Office; 1993. Publication OTA-ISC-
a life-threatening mass casualty situa- preparedness? 559.
2. The Emergency Regarding Weapons of Mass De-
tion. Biological agents may pose only a • Does every HCF in a defined area struction. Congressional Record; November 8, 1995:
temporary risk to the environment or to need this preparedness capability? S16818-16820. Executive order 12938.
3. Flanagin A, Lederberg J. The threat of biological
the people in the area because of rapid • Are there specific chemical and bio- weapons. JAMA. 1996;275:1714-1715.
environmental degradation or difficult logical agents (in the amounts carried 4. Christen H, Maniscalco P. The EMS Incident Man-
248 JAMA, January 12, 2000—Vol 283, No. 2 ©2000 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a SWINBURNE UNIVERSITY OF TECHNOLOGY User on 05/18/2015
PLANNING FOR WEAPONS OF MASS DESTRUCTION EVENTS
agement System. Upper Saddle River, NJ: Prentice- 28. Lillibridge S, Liddle J, Leffingwell S, Sidell F. Re- 54. Eitzen E, Pavlin J, Cieslak T, et al, eds. Medical
Hall Inc; 1998:1-15. port of the American Medical Delegation to Japan. Management of Biological Casualties Handbook. 3rd
5. Nozaki H, Aikawa N, Shinozawa Y, et al. Sarin gas Atlanta, Ga: Centers for Disease Control and Preven- ed. Fort Detrick, Md: US Army Medical Research In-
poisoning in the Tokyo subway. Lancet. 1995;345: tion; 1995. stitute of Infectious Disease; 1998:appendix B.
980-981. 29. Haynes V, Coates J. Motive unclear for 2 charged 55. PPE specifically for biologic agents. In: Chemi-
6. Sidell F, Urbanetti J, Smith W, Hurst C. Vesicants. in germ plot. Chicago Tribune. February 22, 1998:E98. cal and Biological Terrorism; Research and Devel-
In: Zatchuk R, ed. Textbook of Military Medicine. 30. United States v Wheeler, 98 F3d 330 (8th Cir 1996). opment to Improve Civilian Medical Response.
Washington, DC: US Dept of Army, Surgeon Gen- 31. Torok TJ, Tauxe RV, Wise RP, et al. Large com- Washington, DC: National Academy Press; 1999:
eral, and the Borden Institute; 1997:197-228. munity outbreak of salmonellosis caused by inten- 41-42.
7. Carmeli A, Liberman N, Mevorach L. Anxiety- tional contamination of restaurant salad bars. JAMA. 56. Adler J. Missile attacks on Israel during the Gulf
related somatic reactions during missile attacks. Isr 1997;278:389-395. War. Handout prepared for: National Disaster Medi-
J Med Sci. 1991;27:677-680. 32. Horowitz S. B’nai B’rith package contained com- cal System Conference on Lifesaving Intervention; May
8. Nozaki H, Hori S, Shinozawa Y, et al. Secondary ex- mon bacteria. Washington Post. April 29, 1997:B2. 4-7, 1997; Tampa, Fla.
posure of medical staff to sarin vapor in the emergency 33. Bioterrorism alleging use of anthrax and interim 57. Gong E, Dauber W. Policewomen win settle-
room. Intensive Care Med. 1995;21:1032-1035. guidelines for management—United States, 1998. ment. Seattle Times. July 11, 1996:B1.
9. Merritt N, Anderson M. Malathion overdose. MMWR Morb Mortal Wkly Rep. 1999;48:69-74. 58. Stokes J, Banderet L. Psychological aspects of
J Emerg Nurs. 1989;15:463-465. 34. Cone D, Davidson S. Hazardous materials pre- chemical defense and warfare. Mil Psychol. 1997;9:
10. Birenzvige A. Inhalation Hazard from Reaerosol- paredness in the emergency department. Prehosp 395-415.
ized Biological Agents: A Review. Aberdeen, Md: US Emerg Care. 1997;1:85-90. 59. Sidell F. What to do in case of the unthinkable
Army Chemical Research, Development and Engi- 35. Landesman L, Leonard R. SARA three years later. chemical warfare attack or accident. Postgrad Med.
neering Center; 1992. Report TR-413. J Prehosp Disaster Med. 1993;8:39-44. 1990;88:70-84.
11. Association for Professionals in Infection Control 36. Sorokin E. Mystery mail sickens, briefly shuts Fair- 60. Medical Management of Chemical Casualties
and Epidemiology Bioterrorism Task Force and Cen- fax ER. Fairfax Journal. May 2, 1997:A11. Handbook. Aberdeen, Md: US Army Medical Re-
ters for Disease Control and Prevention Bioterrorism 37. Waldron R, Danielson R, Schultz H, et al. Radia- search Institute of Chemical Defense; 1995.
Working Group. Bioterrorism Readiness Plan: A Tem- tion decontamination unit for the community hospi- 61. Medical Management of Biological Casualties
plate for Healthcare Facilities. April 13, 1999. Avail- tal. AJR Am J Roentgenol. 1981;136:977-981. Handbook. Fort Detrick, Md: US Army Medical Re-
able at: http://www.apic.org/html/resc/biomain 38. General Description and Discussion of the Levels search Institute of Infectious Diseases; 1996.
.html. Accessed November 12, 1999. of Protection and Protective Gear, 29 USC §1910.120B 62. Woolf A, Chrisanthus K. On-site availability of se-
12. Keim M, Kaufmann A. Principles for emergency (1989). lected antidotes. Am J Emerg Med. 1997;15:62-66.
response to bioterrorism. Ann Emerg Med. 1999;34: 39. El Sanadi N, Grove C, Takacs M, Daly S, Ellen- 63. Graham B. Clinton to order reserves of germ weapon
177-182. berger D. A hospital-based, hazardous materials de- antidotes. Washington Post. May 21, 1998:A1.
13. Hurst C. Decontamination. In: Zatchuk R, ed. Text- contamination and treatment unit. J Prehosp Disas- 64. McClain D. Smallpox. In: Zatchuk R, ed. Text-
book of Military Medicine. Washington, DC: US Dept ter Med. 1993;8:337-340. book of Military Medicine. Washington, DC: US Dept
of Army, Surgeon General, and the Borden Institute; 40. Cancio LC. Chemical casualty decontamination by of Army, Surgeon General, and the Borden Institute;
1997:351-359. medical platoons in the 82d Airborne Division. Mil 1997:539-559.
14. Franz D, Jahrling P, Friedlander A, et al. Clinical rec- Med. 1993;158:1-5. 65. Hospital Mutual Aid Emergency Preparedness
ognition and management of patients exposed to bio- 41. Rivkind A, Barach P, Israeli A, Berdugo M, Richter Plan. Washington, DC: District of Columbia Hospital
logical warfare agents. JAMA. 1997;278:399-411. E. Emergency preparedness and response in Israel dur- Association; 1996.
15. Inglesby TV, Henderson DA, Bartlett JG, et al, for ing the Gulf War. Ann Emerg Med. 1997;30:513-521. 66. Metropolitan Medical Strike Team Field Opera-
the Working Group on Civilian Biodefense. Anthrax as 42. Karsenty E, Shemer J, Alschech I, et al. Medical tions Guide. Rockville, Md: United States Public Health
a biological weapon. JAMA. 1999;281:1735-1745. aspects of the Iraqi missile attacks on Israel. Isr J Med Service, Office of Emergency Preparedness; 1997.
16. Henderson DA, Inglesby TV, Bartlett JG, et al, for Sci. 1991;27:603-607. 67. Health and Medical Services Support Plan for the
the Working Group on Civilian Biodefense. Smallpox 43. Fehr S. Strike team proposed for quick response Federal Response to Acts of Chemical/Biological (C/B)
as a biological weapon. JAMA. 1999;281:2127-2137. to terrorist attack. Washington Post. Nov 7, 1995:B3. Terrorism. Washington, DC: US Dept of Health and
17. US Army Soldier Biological and Chemical Com- 44. Nunn-Lugar-Domenici Amendment to the FY 97 Human Services; 1996.
mand. Biological Warfare Improved Response Pro- Defense Authorization Act, Pub L No. 104-201, Title 68. Sullivan J, Krieger G. Hazardous Materials Toxi-
gram. March 10, 1999. Available at: http://dp.sbccom XIV: Defense Against Weapons of Mass Destruction, cology. Baltimore, Md: Williams & Wilkins; 1992.
.army.mil/fs/index.html. Accessed November 29, 1999. Subtitle A: Domestic Preparedness. US Congress; June 69. Shapira Y, Bar Y, Berkenstadt H, Atsmon J, Danon
18. Hall H, Dhara V, Price-Green P, Kaye W. Surveil- 27, 1996. Y. Outline of hospital organization for a chemical war-
lance for emergency events involving hazardous sub- 45. Report to Congress: Response to Threats of Ter- fare attack. Isr J Med Sci. 1991;27:616-622.
stances—United States, 1990-1992. MMWR Morb rorist Use of Weapons of Mass Destruction. Wash- 70. Levitin H, Siegelson H. Hazardous materials. Emerg
Mortal Wkly Rep. 1994;43(SS-2):1-6. ington, DC: US Dept of Defense; January 31, 1997. Med Clin. 1996;14:327-348.
19. Binder S. Deaths, injuries and evacuations from 46. Domestic Preparedness Program, Defense Against 71. Cox R. Decontamination and management of haz-
acute hazardous material releases. Am J Public Health. Weapons of Mass Destruction. Technician-Hospital ardous materials exposure victims in the emergency
1989;79:1042-1044. Provider Course Manual. Aberdeen, Md: US Army CB- department. Ann Emerg Med. 1994;23:761-770.
20. US Department of Health and Human Services. DCOM, Domestic Preparedness Office; 1997. 72. Noll G, Hildebrand M, Yvorra J. Personal protec-
Managing Hazardous Materials Incidents. Washing- 47. Graham B. Anti-terrorism plans termed inad- tive clothing and equipment. In: Daly P, ed. Hazard-
ton, DC: Agency for Toxic Substances and Disease Reg- equate. Washington Post. October 3, 1998:A9. ous Materials. Stillwater: Fire Protection Publica-
istry; 1992. 48. Hauer JM. Preparing for terrorism involving weap- tions, Oklahoma State University; 1995:285-322.
21. Centers for Disease Control and Prevention. CDC ons of mass destruction. Presented at: US Capitol Po- 73. Gold M, Bongiovanni R, Scharf B, Gresham V,
recommendations for civilian communities near chemi- lice Board; February 26, 1998; Washington, DC. Woodward C. Hypochlorite solution as a decontami-
cal weapons depots. 60 Federal Register 33307- 49. HAZ/MAT DQE involved in national prepared- nant in sulfur mustard contaminated skin defects in
33318 (1995). ness. HAZ/MAT DQE News. 1998;6:2. the euthymic hairless guinea pig. Drug Chem Toxi-
22. Carnes S, Watson A. Disposing of the US chemi- 50. Burgess J, Kirk M, Borron S, Cisek J. Emergency col. 1994;17:499-527.
cal weapons stockpile. JAMA. 1989;262:653-659. department hazardous materials protocol for contami- 74. Borak J, Callan M, Abbott W. Hazardous Mate-
23. Memorandrum 35 from President Richard M. Nixon nated patients. Ann Emerg Med. 1999;34:205-212. rials Exposures. Englewood Cliffs, NJ: Brady Publica-
regarding national security decision; November 25, 1969. 51. Londorf D. Hospital application of the incident tions; 1991:145.
24. Memorandrum 44 from President Richard M. Nixon management system. J Prehosp Disaster Med. 1995; 75. Sullivan F, Wang R, Jenouri I. Principles and pro-
regarding national security decision; February 20, 1970. 10:184-188. tocols for prevention, evaluation, and management
25. Fullerton C, Ursano R. Health care delivery in the 52. Access to PPE. In: Chemical and Biological Ter- of exposure to hazardous materials. Emerg Med Rep.
high stress environment of chemical and biological war- rorism; Research and Development to Improve Civil- 1998;19:21-32.
fare. Mil Med. 1994;159:524-528. ian Medical Response. Washington, DC: National 76. Barbera J, Macintyre A. Urban search and res-
26. Bleich A, Shmuel K, Margalit C, et al. Israeli psy- Academy Press; 1999:35-36. cue. Emerg Med Clin North Am. 1996;14:399-412.
chological casualties of the Persian Gulf War. Isr J Med 53. Protective measures and handling of casualties. 77. Frykberg E, Tepas J. Terrorist bombings. Ann Surg.
Sci. 1991;27:673-676. In: Treatment of Chemical Agent Casualties and Con- 1988;208:569-576.
27. Okumara T, Takusa N, Ishimatsu S, et al. Report ventional Military Chemical Injuries. Washington, DC: 78. Mallonee S, Shariat S, Stennies G, et al. Physical
on 640 victims of the Tokyo subway sarin attack. Ann US Government Printing Office; 1990. FM 8-285, injuries and fatalities resulting from the Oklahoma City
Emerg Med. 1996;28:129-135. NAVMED P-5041, AFM 160-11. bombing. JAMA. 1996;276:382-390.
©2000 American Medical Association. All rights reserved. JAMA, January 12, 2000—Vol 283, No. 2 249
Downloaded From: http://jama.jamanetwork.com/ by a SWINBURNE UNIVERSITY OF TECHNOLOGY User on 05/18/2015
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Preparacion Hospitalaria para Evento QBRN IRANDocument5 pagesPreparacion Hospitalaria para Evento QBRN IRANCVOED Nivel CentralNo ratings yet
- Okumura1998 Experiencia de TokyoDocument5 pagesOkumura1998 Experiencia de TokyoCVOED Nivel CentralNo ratings yet
- Rodgers 1998Document5 pagesRodgers 1998CVOED Nivel CentralNo ratings yet
- Liberacion de SustanciasDocument22 pagesLiberacion de SustanciasCVOED Nivel CentralNo ratings yet
- Bioterrorismo 123Document8 pagesBioterrorismo 123CVOED Nivel CentralNo ratings yet
- GuideDocument296 pagesGuideCVOED Nivel CentralNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- PPT15Document22 pagesPPT15Kusuma SaddalaNo ratings yet
- PERCEPTION-OF-TEENAGERS-WHO-HAVE-WITNESSED-THEIR-PARENTS-AS-A-VICTIM-OF-DOMESTIC-VIOLENCE[2]Document13 pagesPERCEPTION-OF-TEENAGERS-WHO-HAVE-WITNESSED-THEIR-PARENTS-AS-A-VICTIM-OF-DOMESTIC-VIOLENCE[2]Christian CudadaNo ratings yet
- Report On School CanteenDocument2 pagesReport On School CanteenChin Kian83% (6)
- Unit 4. CPH - Alma Ata (PHC) SDGDocument111 pagesUnit 4. CPH - Alma Ata (PHC) SDGAesthetics MinNo ratings yet
- Week 2Document11 pagesWeek 2Zanne AlcasidNo ratings yet
- Lesson PlanDocument45 pagesLesson PlanHarman GillNo ratings yet
- Physical Fitness Test Score Card SKILL RELATED FITDocument1 pagePhysical Fitness Test Score Card SKILL RELATED FITPaulo Victor SazonNo ratings yet
- Fundamentals of Nursing Workbook: NUC 103 - SUMMER 2021Document10 pagesFundamentals of Nursing Workbook: NUC 103 - SUMMER 2021Rawan KhateebNo ratings yet
- Application of Acceleration Behavioral TherapyDocument2 pagesApplication of Acceleration Behavioral TherapyCaitlin PeñeraNo ratings yet
- CAED 500C Component A SIMDocument68 pagesCAED 500C Component A SIMWan SebenNo ratings yet
- PreviewpdfDocument41 pagesPreviewpdfNtli RfNo ratings yet
- Atom Electrosurgical SystemDocument40 pagesAtom Electrosurgical SystemOgut AjaNo ratings yet
- Mapeh - P.E. 6: First Quarter-Module 3 Topic: Skills Involved in Playing GamesDocument8 pagesMapeh - P.E. 6: First Quarter-Module 3 Topic: Skills Involved in Playing GamesNICOLE ALANA100% (1)
- Diploma in Yogic ScienceDocument18 pagesDiploma in Yogic ScienceRadhey KrishnaNo ratings yet
- Module 1 - Introduction To Community Engagement: Lesson No. 1.1 - Understanding The CommunityDocument4 pagesModule 1 - Introduction To Community Engagement: Lesson No. 1.1 - Understanding The CommunityCamille MarapocNo ratings yet
- 843 Ai MSDocument5 pages843 Ai MSHitarth ShahNo ratings yet
- Knox hw425 Unit 9 PresentationDocument12 pagesKnox hw425 Unit 9 Presentationapi-587886115No ratings yet
- Body Image Disturbance NCPDocument1 pageBody Image Disturbance NCPreneighd50% (4)
- Coding DecodingDocument78 pagesCoding DecodingShashank ParateNo ratings yet
- Jurnal Data P4GN 2015 - Edisi 2016 - ENDocument228 pagesJurnal Data P4GN 2015 - Edisi 2016 - ENAnti NarkobaNo ratings yet
- Welcome To Month 36 of Booty by Bret!: This Month Is A & PlanDocument14 pagesWelcome To Month 36 of Booty by Bret!: This Month Is A & PlanLi SaNo ratings yet
- Process Industry Practices Piping: PIP PNE00003 Process Unit and Offsites Layout GuideDocument14 pagesProcess Industry Practices Piping: PIP PNE00003 Process Unit and Offsites Layout GuideSilambarasan PalanisamyNo ratings yet
- PMTCT NamibiaDocument17 pagesPMTCT NamibiaMayom MabuongNo ratings yet
- Group 2 Locsin OrlandoDocument5 pagesGroup 2 Locsin OrlandoBrent Ederson AmadoNo ratings yet
- Right To Food in India: A Constitutional Perspective: Sanjeeve Gowda.G.SDocument12 pagesRight To Food in India: A Constitutional Perspective: Sanjeeve Gowda.G.SZainy KhanNo ratings yet
- Philippine Infectious Control Nurse AssociationDocument3 pagesPhilippine Infectious Control Nurse AssociationFerdinand Natividad0% (1)
- Prolonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkDocument5 pagesProlonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkRahulLife'sNo ratings yet
- Prime-Hrm 2Document16 pagesPrime-Hrm 2Cha Magaoay TamaniNo ratings yet
- UEFA B Licence Football Physiology 2 Injury PreventionDocument82 pagesUEFA B Licence Football Physiology 2 Injury PreventionSadio ManéNo ratings yet
- Grimslingers-Core Rulebook (5.5x8.5in) v1.3Document43 pagesGrimslingers-Core Rulebook (5.5x8.5in) v1.3Mister ZombieNo ratings yet















































![PERCEPTION-OF-TEENAGERS-WHO-HAVE-WITNESSED-THEIR-PARENTS-AS-A-VICTIM-OF-DOMESTIC-VIOLENCE[2]](https://imgv2-2-f.scribdassets.com/img/document/730674957/149x198/cd66d91213/1715205612?v=1)



























