You might also like
- 2019 Article 1560Document7 pages2019 Article 1560Karylle Ezra GulifardoNo ratings yet
- Curriculum Alignment and EvaluationDocument11 pagesCurriculum Alignment and Evaluationapi-695177304No ratings yet
- Model Pendidikan Interprofesional Dalam 5487b47c PDFDocument11 pagesModel Pendidikan Interprofesional Dalam 5487b47c PDFNabila PamardikaNo ratings yet
- Purposes of Health Education and Education ProcessDocument5 pagesPurposes of Health Education and Education ProcessBonsucan, Lee Deniel D.No ratings yet
- Template For Evaluation of Curriculum Week 4Document12 pagesTemplate For Evaluation of Curriculum Week 4api-598498344No ratings yet
- A Systematic Review of The Effects of Residency Training On Patients OutcomesDocument11 pagesA Systematic Review of The Effects of Residency Training On Patients OutcomesMaik MouraNo ratings yet
- Compassion Cultivation Training Promotes Medical Student Wellness and Enhanced Clinical CareDocument11 pagesCompassion Cultivation Training Promotes Medical Student Wellness and Enhanced Clinical CareMichelle TorresNo ratings yet
- Role of Medical Education in Cultivating LifelongDocument4 pagesRole of Medical Education in Cultivating LifelongRudolph SunnydaysNo ratings yet
- Jurnas Bull2017Document10 pagesJurnas Bull2017miftah zannahNo ratings yet
- Importance and Purposes of Research: Instruction: Answer Comprehensively and ExtensivelyDocument3 pagesImportance and Purposes of Research: Instruction: Answer Comprehensively and ExtensivelyKarl Kiw-isNo ratings yet
- Motivational Interviewing Training For Medical StudentsDocument35 pagesMotivational Interviewing Training For Medical StudentsBruno AlencarNo ratings yet
- Health Coaching Quality FrameworkDocument22 pagesHealth Coaching Quality FrameworkGONDHES CHANNELNo ratings yet
- Faculty Development CPDDocument6 pagesFaculty Development CPDAida TantriNo ratings yet
- Name: Hida Zulfiyah NIM: 2021102030029 Class: 1C Semester: 1 Study Program: Bachelor of NursingDocument14 pagesName: Hida Zulfiyah NIM: 2021102030029 Class: 1C Semester: 1 Study Program: Bachelor of NursingShafiraa MaharaniNo ratings yet
- Interpersonal SkillsDocument2 pagesInterpersonal SkillsUmarameshKNo ratings yet
- Ijerph 17 05442Document8 pagesIjerph 17 05442NIAZ HUSSAINNo ratings yet
- Effectiveness of A Self-Directed LearningDocument8 pagesEffectiveness of A Self-Directed LearningZilbran BerontaxNo ratings yet
- Sicometrik ICP IndonesiaDocument10 pagesSicometrik ICP IndonesiaUchi SuhermanNo ratings yet
- Research in Continuing EducationDocument2 pagesResearch in Continuing EducationAchademaatram Molu100% (2)
- Effectiveness of Continuing Education Programmes in Nursing: Literature ReviewDocument1 pageEffectiveness of Continuing Education Programmes in Nursing: Literature ReviewSilpa RatheeshNo ratings yet
- Meresume Artikel Konsep Dasar KeperawatanDocument24 pagesMeresume Artikel Konsep Dasar KeperawatanTika SetyariniNo ratings yet
- Interprofessional Educationand CollaborationDocument7 pagesInterprofessional Educationand CollaborationnersrosdianaNo ratings yet
- CMPP Syllabus. December.2018Document124 pagesCMPP Syllabus. December.2018Harsh SNo ratings yet
- Physiotherapy Students DiSC Behaviour Styles CanDocument16 pagesPhysiotherapy Students DiSC Behaviour Styles CanThanh Ha LeNo ratings yet
- Nursing Staffs Self-Perceived Outcome From A Rehabilitation 24/7 Educational Programme - A Mixed-Methods Study in Stroke CareDocument13 pagesNursing Staffs Self-Perceived Outcome From A Rehabilitation 24/7 Educational Programme - A Mixed-Methods Study in Stroke Care2020614266No ratings yet
- Interprofessional Edited EditedDocument4 pagesInterprofessional Edited EditedjuliuswamuguNo ratings yet
- Citit 1Document11 pagesCitit 1Florina AnichitoaeNo ratings yet
- Medical Education in Pulmonary, Critical Care, and Sleep Medicine: Advanced Concepts and StrategiesFrom EverandMedical Education in Pulmonary, Critical Care, and Sleep Medicine: Advanced Concepts and StrategiesPatricia A. KritekNo ratings yet
- Kidney Careoutline1203Document3 pagesKidney Careoutline1203weesiniNo ratings yet
- Teaching Consistent Hand Hygiene: How Can We Improve?: ReviewsDocument8 pagesTeaching Consistent Hand Hygiene: How Can We Improve?: Reviewsvanessa patayonNo ratings yet
- Ijims 2015 117Document13 pagesIjims 2015 117intan juitaNo ratings yet
- Laura Butz BSN, RN Department of Nursing Education, SUNY DELHI NUR 602: Katherine QuartuccioDocument13 pagesLaura Butz BSN, RN Department of Nursing Education, SUNY DELHI NUR 602: Katherine Quartuccioapi-731721004No ratings yet
- Education Plan #1Document5 pagesEducation Plan #118sn02nr059No ratings yet
- Course Design for Public Health: A Competency Based ApproachFrom EverandCourse Design for Public Health: A Competency Based ApproachNo ratings yet
- Interdisciplinary Collaboration: Experience of Working in An Interdisciplinary Team in Healthcare at The MOI Teaching and Referral Hospital, Intensive Care UnitDocument3 pagesInterdisciplinary Collaboration: Experience of Working in An Interdisciplinary Team in Healthcare at The MOI Teaching and Referral Hospital, Intensive Care UnitInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Attention To Fidelity: Why Is It ImportantDocument2 pagesAttention To Fidelity: Why Is It ImportantDalene EvangelioNo ratings yet
- Development and Experimental Results of Outcomes-Based Nursing ProgramDocument6 pagesDevelopment and Experimental Results of Outcomes-Based Nursing ProgramIJAR JOURNALNo ratings yet
- Interprofessional Education - The Way Forward in Health ProfessionDocument2 pagesInterprofessional Education - The Way Forward in Health ProfessionJLatriece Elizabeth CedeñoNo ratings yet
- Exploring Faculty Preparedness and Capability For Interprofessional LearningDocument1 pageExploring Faculty Preparedness and Capability For Interprofessional LearningSadashiv RahaneNo ratings yet
- Jurnal 8Document9 pagesJurnal 8IRFANNo ratings yet
- Health Educ1Document6 pagesHealth Educ1Märsh Pascual-DapunNo ratings yet
- Continuando La Educacion Medica para Los Practicantes Generales - Un Formato para PracticasDocument6 pagesContinuando La Educacion Medica para Los Practicantes Generales - Un Formato para PracticasAnonymous 3MPClbaCDNo ratings yet
- Aet2 10354Document8 pagesAet2 10354Edris ZamroniNo ratings yet
- Researcharticle Open Access: Kuo-Chen Liao, Shou-Jin Pu, Maw-Sen Liu, Chih-Wei Yang and Han-Pin KuoDocument7 pagesResearcharticle Open Access: Kuo-Chen Liao, Shou-Jin Pu, Maw-Sen Liu, Chih-Wei Yang and Han-Pin KuoprabhatNo ratings yet
- Assessment of Learning NeedsDocument4 pagesAssessment of Learning NeedsRhonaJoyNo ratings yet
- IPE Interprofessional EducationDocument10 pagesIPE Interprofessional EducationdewaNo ratings yet
- Ojn 2015082114174498Document10 pagesOjn 2015082114174498ahmadNo ratings yet
- Interprofessional Teams-Health CanadaDocument16 pagesInterprofessional Teams-Health CanadaKimberly AvendanoNo ratings yet
- Develop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenDocument8 pagesDevelop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenpsicoterapiavaldiviaNo ratings yet
- Rw-Omj-D-18-00175 (05C)Document6 pagesRw-Omj-D-18-00175 (05C)nersrosdianaNo ratings yet
- Literature Review-Ebc839d4Document4 pagesLiterature Review-Ebc839d4jamesNo ratings yet
- Assigment 2 - 8615Document21 pagesAssigment 2 - 8615umair siddiqueNo ratings yet
- Cuin 7397 Final Project - Resilience Leadership Grant Application - Cohensuessman FinalDocument13 pagesCuin 7397 Final Project - Resilience Leadership Grant Application - Cohensuessman Finalapi-519560362No ratings yet
- Preparing Nursing Students For Interprofessional Learning: June 2014Document7 pagesPreparing Nursing Students For Interprofessional Learning: June 2014Ahmad Tri Anggara SasmitaNo ratings yet
- 2011 Impacto Do Uso Da Estrutura Da CIF em Fisioterapia PediátricaDocument8 pages2011 Impacto Do Uso Da Estrutura Da CIF em Fisioterapia PediátricaCibelle FormigaNo ratings yet
- Research in Continuing Education Seminar Typed ContentDocument17 pagesResearch in Continuing Education Seminar Typed ContentIze C Viji93% (14)
- Module guideNURS209 ClinicalDocument40 pagesModule guideNURS209 ClinicalScelo CalvinNo ratings yet
- Overview of Education and Nursing Process 1Document5 pagesOverview of Education and Nursing Process 1kjdobdin23No ratings yet
- INTRODUCTIONDocument13 pagesINTRODUCTIONAdimasu BerNo ratings yet
- Physical Activity Counseling Content and Competency: A Systematic ReviewDocument21 pagesPhysical Activity Counseling Content and Competency: A Systematic Reviewalcione12No ratings yet
- Support 1Document12 pagesSupport 1Khánh LinhNo ratings yet
- Key PaperDocument12 pagesKey PaperKhánh LinhNo ratings yet
- CH 10Document13 pagesCH 10Khánh LinhNo ratings yet
- Ch9 1Document8 pagesCh9 1Khánh LinhNo ratings yet
- Guide To Mindfulness: The 10 Minute For Adults With ADHDDocument21 pagesGuide To Mindfulness: The 10 Minute For Adults With ADHDLuisMariano RiveraCelaNo ratings yet
- Duggan and Reichgelt 2006 Measuring Information System Delivery QualityDocument383 pagesDuggan and Reichgelt 2006 Measuring Information System Delivery QualityJohanes PurbaNo ratings yet
- Ielts Academic Writing Sample ScriptDocument6 pagesIelts Academic Writing Sample Scriptkc103038No ratings yet
- The Roots of Unfairness: The Black Swan in Arts and LiteratureDocument7 pagesThe Roots of Unfairness: The Black Swan in Arts and LiteratureAlfian 'aaL' EikmanNo ratings yet
- Mat 2377 Final 2011Document12 pagesMat 2377 Final 2011David LinNo ratings yet
- Imt 51Document4 pagesImt 51arun1974No ratings yet
- ResearchDocument6 pagesResearchDomNo ratings yet
- Paper 1: Organization & Management Fundamentals - Syllabus 2008 Evolution of Management ThoughtDocument27 pagesPaper 1: Organization & Management Fundamentals - Syllabus 2008 Evolution of Management ThoughtSoumya BanerjeeNo ratings yet
- Learning To Labour by Paul Willis, by Sheryl ShahabDocument13 pagesLearning To Labour by Paul Willis, by Sheryl ShahabSheryl ShahabNo ratings yet
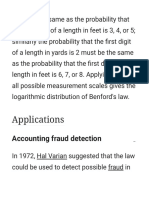
- Benford's Law - WikipediaDocument7 pagesBenford's Law - WikipediaBakari HamisiNo ratings yet
- Nso Census BAGUIO CITY - FINAL PDFDocument121 pagesNso Census BAGUIO CITY - FINAL PDFVictor Conrad AlinioNo ratings yet
- AP Seminar CED 2020 PDFDocument134 pagesAP Seminar CED 2020 PDFTammy DobrzynskiNo ratings yet
- Test Bank For What Is Life A Guide To Biology With Physiology 1st Edition PhelanDocument25 pagesTest Bank For What Is Life A Guide To Biology With Physiology 1st Edition PhelanChester Gildea100% (24)
- Rujukan ARDocument3 pagesRujukan ARcrunx89No ratings yet
- BowTieXP What Is A BowTieDocument18 pagesBowTieXP What Is A BowTieJoseph Markham100% (2)
- 008fnh Bacani FTDocument6 pages008fnh Bacani FTmauliana maul100% (1)
- Downsizing T&DDocument13 pagesDownsizing T&DoxyguyNo ratings yet
- Operations Research - BMS - AssignmentDocument1 pageOperations Research - BMS - AssignmentJennifer MathaisNo ratings yet
- Final Na Talaga ToDocument54 pagesFinal Na Talaga ToJoy ManguneNo ratings yet
- Characteristics of Chinese Students' Learning StylesDocument4 pagesCharacteristics of Chinese Students' Learning StylesRose SugiantoNo ratings yet
- Chem 105 Syllabus 2013 SpringDocument4 pagesChem 105 Syllabus 2013 SpringemuphychemNo ratings yet
- Brainstorming For Research TopicsDocument18 pagesBrainstorming For Research TopicsMa. Aiza SantosNo ratings yet
- Possession and Its Various Kinds: Submitted byDocument3 pagesPossession and Its Various Kinds: Submitted bysajal sanatanNo ratings yet
- PR 3Document6 pagesPR 3Rexie ArcenaNo ratings yet
- Locating Credible Databases and ResearchDocument7 pagesLocating Credible Databases and ResearchTrex WritersNo ratings yet
- CV Dr. HB - Croxatto - English March 2008Document9 pagesCV Dr. HB - Croxatto - English March 2008Camillita BelénNo ratings yet
- Midterm Fall 2019Document8 pagesMidterm Fall 2019NEERAJ KUMARNo ratings yet
- Course Map EconomicsDocument2 pagesCourse Map Economicsshengopal8769No ratings yet
- CH 5 - Consumer Markets and Consumer Buyer BehaviorDocument58 pagesCH 5 - Consumer Markets and Consumer Buyer BehaviorMuhammad Shahbaz AkramNo ratings yet
- Post Normal ScienceDocument22 pagesPost Normal ScienceGuillermo FerraguttiNo ratings yet