You might also like
- Guidelines Adhd AdultDocument19 pagesGuidelines Adhd AdultJavier Cotobal100% (1)
- 90 Essential Nutrients-Cellular LevelDocument3 pages90 Essential Nutrients-Cellular Leveliamfree175% (8)
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument12 pagesPlan Plan Plan Premium: Important Questions Answers Why This Mattersapi-252555369No ratings yet
- KATO Design Manual HighDocument98 pagesKATO Design Manual HighJai Bhandari100% (1)
- Aura and Chakra 3Document88 pagesAura and Chakra 3Theodore Yiannopoulos100% (2)
- Study Abroad Consultant in PanchkulaDocument17 pagesStudy Abroad Consultant in Panchkulashubham mehtaNo ratings yet
- PM Speed Adjusting Motor For PSGDocument2 pagesPM Speed Adjusting Motor For PSGFathima Regin100% (2)
- B Veletsis PDFDocument2 pagesB Veletsis PDFdonnaNo ratings yet
- AARP UHC 2024 Benefit Highlights LA 004P FocusDocument4 pagesAARP UHC 2024 Benefit Highlights LA 004P FocusAlaa ZaidNo ratings yet
- Benefit Highlights: AARP Medicare Advantage Choice (PPO)Document3 pagesBenefit Highlights: AARP Medicare Advantage Choice (PPO)EstherNo ratings yet
- Orge Compare PDFDocument2 pagesOrge Compare PDFdonnaNo ratings yet
- Your Prescription Benefit at A GlanceDocument2 pagesYour Prescription Benefit at A GlancepverdanceNo ratings yet
- Doxycycline Hyclate Prices, Coupons & Savings Tips - GoodRxDocument1 pageDoxycycline Hyclate Prices, Coupons & Savings Tips - GoodRxOmayra AvilaNo ratings yet
- ViewyoursbcdocumentDocument12 pagesViewyoursbcdocumentapi-531507901No ratings yet
- B.Veletsis-Anthem MediBlue RX Plus (PDP) PDFDocument9 pagesB.Veletsis-Anthem MediBlue RX Plus (PDP) PDFdonnaNo ratings yet
- B.Veletsis-Humana Walmart Value RX Plan (PDP) PDFDocument8 pagesB.Veletsis-Humana Walmart Value RX Plan (PDP) PDFdonnaNo ratings yet
- H. Taylor PDFDocument2 pagesH. Taylor PDFdonnaNo ratings yet
- MR Veletsis-Compare PDFDocument2 pagesMR Veletsis-Compare PDFdonnaNo ratings yet
- Aurora - Baseline Option 2019 SOBIDocument4 pagesAurora - Baseline Option 2019 SOBISean MurrayNo ratings yet
- Buy Bulker Stack Online - SARMs Swiss ChemsDocument1 pageBuy Bulker Stack Online - SARMs Swiss ChemsPetruNo ratings yet
- Ipnature S Bounty Sleep3 Sleep Aid With Melatonin Relaxation and Stress Relief Tri Layered Tablets 10 MDocument1 pageIpnature S Bounty Sleep3 Sleep Aid With Melatonin Relaxation and Stress Relief Tri Layered Tablets 10 Mkuddusi kurtNo ratings yet
- Bupropion XL 150mg: W H 6 0 0 0 0 3 DR33 0 1 5 9 9 5 GDCDocument1 pageBupropion XL 150mg: W H 6 0 0 0 0 3 DR33 0 1 5 9 9 5 GDCAlex LuNo ratings yet
- Foodpanda Coupons: Upto Rs. 75 Cashback From CouponduniaDocument4 pagesFoodpanda Coupons: Upto Rs. 75 Cashback From CouponduniaRandNo ratings yet
- 2022-2023 FCPS - Anthem KeyCare 25 SBCDocument13 pages2022-2023 FCPS - Anthem KeyCare 25 SBCRichardRobbinsNo ratings yet
- Veletsis-Wellcare Value Script (PDP) PDFDocument8 pagesVeletsis-Wellcare Value Script (PDP) PDFdonnaNo ratings yet
- Pharma & Lifescience: - Rasesh KelkarDocument9 pagesPharma & Lifescience: - Rasesh Kelkar9980139892No ratings yet
- Supply Chain - Alt 3Document8 pagesSupply Chain - Alt 3sriram.srikanthNo ratings yet
- WWW Healthcare Gov/sbc-GlossaryDocument6 pagesWWW Healthcare Gov/sbc-Glossarytroubledcutie1987No ratings yet
- Anthem Anthem Gold Hmo 35 4huvDocument11 pagesAnthem Anthem Gold Hmo 35 4huvLn TranNo ratings yet
- Everyday Extras: Get The Same Amount Back Each Time You VisitDocument2 pagesEveryday Extras: Get The Same Amount Back Each Time You Visitfrank.wangNo ratings yet
- Certo Detox - Google ShoppingDocument1 pageCerto Detox - Google ShoppingSosa BlickemNo ratings yet
- HDHPDocument10 pagesHDHPAnonymous KnnAxcNo ratings yet
- HomeDocument1 pageHomeMiranda HathewayNo ratings yet
- 2018 Mhealth DirectDocument2 pages2018 Mhealth DirectSasha NelsonNo ratings yet
- Medication Pricing - PharmacyDocument4 pagesMedication Pricing - Pharmacysuresh420No ratings yet
- Can I Apply?: P.O. Box 5727, Louisville, Kentucky 40255-0727 Phone: 1-800-830-9159 Fax: 1-800-497-0928Document4 pagesCan I Apply?: P.O. Box 5727, Louisville, Kentucky 40255-0727 Phone: 1-800-830-9159 Fax: 1-800-497-0928VelozaNo ratings yet
- Lower Prescription Prices With Pharmacy Discounts and Coupons With The WebMDRx Savings CardDocument1 pageLower Prescription Prices With Pharmacy Discounts and Coupons With The WebMDRx Savings Card36tacosNo ratings yet
- 2018 Employee Benefits at A GlanceDocument27 pages2018 Employee Benefits at A GlancePeter RussoNo ratings yet
- 2019 Plan BenefitsDocument14 pages2019 Plan BenefitsMichelleJeungNo ratings yet
- Medications Details Mark Cuban Cost Plus Drug CompanyDocument1 pageMedications Details Mark Cuban Cost Plus Drug Companyk7n7fc4dc7No ratings yet
- 2024 KP Gold SummaryDocument16 pages2024 KP Gold Summaryapi-531507901No ratings yet
- The Ordinary The Daily Set 3 Piece Skincare Gift SetsDocument1 pageThe Ordinary The Daily Set 3 Piece Skincare Gift Setslaragribble10No ratings yet
- Cessation Therapy 2 4Document1 pageCessation Therapy 2 4Alexander ChamessianNo ratings yet
- GV 27Document68 pagesGV 27Christopher CarrilloNo ratings yet
- GreeNatr Ginseng Ginkgo BilobaDocument10 pagesGreeNatr Ginseng Ginkgo BilobamikeNo ratings yet
- CARRIER APPROVED 12052018 Legion-Limited-Medical Sales-Aid - 8.7.2018Document4 pagesCARRIER APPROVED 12052018 Legion-Limited-Medical Sales-Aid - 8.7.2018Antonio DavisNo ratings yet
- Advil Ibuprofen Pain Reliever & Fever Reducer Tablets WalgreensDocument1 pageAdvil Ibuprofen Pain Reliever & Fever Reducer Tablets WalgreensLorette AraujoNo ratings yet
- VEBA Plan PresentationDocument19 pagesVEBA Plan PresentationMitchell BigleyNo ratings yet
- Allowed Amount Balance Billing Coinsurance Copayment Deductible ProviderDocument10 pagesAllowed Amount Balance Billing Coinsurance Copayment Deductible ProviderHunter WilliamsNo ratings yet
- M2A1 US Census Data SearchDocument6 pagesM2A1 US Census Data SearchragcajunNo ratings yet
- Novus Research Order FormsDocument1 pageNovus Research Order Formstyjc87No ratings yet
- TonicgreensDocument7 pagesTonicgreenshafizefaisalsandhuNo ratings yet
- Group Project 1Document21 pagesGroup Project 1api-547174770No ratings yet
- Kentucky: Medicare Advantage Cost Plans and DemonstrationsDocument46 pagesKentucky: Medicare Advantage Cost Plans and Demonstrationsanon-76504No ratings yet
- Anoc Saver TXDocument11 pagesAnoc Saver TXIsmael LanderosNo ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument6 pagesPlan Plan Plan Premium: Important Questions Answers Why This MattersDavid TranNo ratings yet
- Bounty Quick-Size Paper Towels, White, 12 Family Rolls 30 Regular Rolls (Packaging May Vary) Health & HouseholdDocument1 pageBounty Quick-Size Paper Towels, White, 12 Family Rolls 30 Regular Rolls (Packaging May Vary) Health & HouseholdMassabaliKhanNo ratings yet
- Adrenal & Cortisol Support-Combat Adrenal Fatigue Dr. BergDocument1 pageAdrenal & Cortisol Support-Combat Adrenal Fatigue Dr. BergPetra KratochvilovaNo ratings yet
- SignupplanformDocument1 pageSignupplanformmt2z48jhbmNo ratings yet
- Med AssestsDocument6 pagesMed Assestsapi-26219976No ratings yet
- Felix Khuluza & Lutz Heide 22. April 2014: PHA 406 Drug and Medical Supplies Management IIDocument36 pagesFelix Khuluza & Lutz Heide 22. April 2014: PHA 406 Drug and Medical Supplies Management IIShoaib BiradarNo ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument8 pagesPlan Plan Plan Premium: Important Questions Answers Why This Mattersrocerev539No ratings yet
- Check Store Stock Add To Favourites: Anusol Soothing Relief Ointment 15gDocument1 pageCheck Store Stock Add To Favourites: Anusol Soothing Relief Ointment 15gAlbiSarah MazariNo ratings yet
- Associate Price List: United States PacksDocument4 pagesAssociate Price List: United States PacksMonette EvangelistaNo ratings yet
- Goodyear RebateForm US NPP4 2021 PDFDocument1 pageGoodyear RebateForm US NPP4 2021 PDFdonnaNo ratings yet
- H. Taylor PDFDocument2 pagesH. Taylor PDFdonnaNo ratings yet
- B.Veletsis-Humana Walmart Value RX Plan (PDP) PDFDocument8 pagesB.Veletsis-Humana Walmart Value RX Plan (PDP) PDFdonnaNo ratings yet
- B.Veletsis-Anthem MediBlue RX Plus (PDP) PDFDocument9 pagesB.Veletsis-Anthem MediBlue RX Plus (PDP) PDFdonnaNo ratings yet
- Veletsis-Wellcare Value Script (PDP) PDFDocument8 pagesVeletsis-Wellcare Value Script (PDP) PDFdonnaNo ratings yet
- MR Veletsis-Compare PDFDocument2 pagesMR Veletsis-Compare PDFdonnaNo ratings yet
- PCH301 (Lab) - Midterm - Q1 - LA 6 - Volhard MethodDocument3 pagesPCH301 (Lab) - Midterm - Q1 - LA 6 - Volhard MethodAdi MinisterioNo ratings yet
- Ishida Checkweigher Scotraco PDFDocument6 pagesIshida Checkweigher Scotraco PDFchrissNo ratings yet
- B 03 01 Operation Guide Parameters Material ManagementDocument12 pagesB 03 01 Operation Guide Parameters Material ManagementCdcArduino ArduinoNo ratings yet
- Format For The Industrial Training ReportDocument7 pagesFormat For The Industrial Training ReportAbdulHalimNo ratings yet
- Week 1Document27 pagesWeek 1Bawa BoyNo ratings yet
- CASE STUDY - Nirma V.S HulDocument4 pagesCASE STUDY - Nirma V.S HulRicha Shruti0% (1)
- ADAU1701Document12 pagesADAU1701onafetsNo ratings yet
- Icpna Project 1Document29 pagesIcpna Project 1Jesus Martin Yaya TorresNo ratings yet
- Sociologia Şi Ştiinţa Naţiunii În Doctrina Lui Dimitrie GustiDocument35 pagesSociologia Şi Ştiinţa Naţiunii În Doctrina Lui Dimitrie GustiSaveanu RazvanNo ratings yet
- ProgramDetails PDF 134Document2 pagesProgramDetails PDF 134samyakgaikwad12No ratings yet
- Chapter 24 - Glass and Glazing PDFDocument14 pagesChapter 24 - Glass and Glazing PDFpokemonNo ratings yet
- Harsh PatelDocument14 pagesHarsh PatelPradeepNo ratings yet
- SpinnerbaitDocument1 pageSpinnerbaitDioônata VieiraNo ratings yet
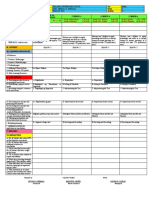
- DLL Q3 Week 4 Day5 WWDocument3 pagesDLL Q3 Week 4 Day5 WWCecilia Guevarra DumlaoNo ratings yet
- Imaginefx How To Draw and Paint Anatomy Volume 2Document116 pagesImaginefx How To Draw and Paint Anatomy Volume 2tofupastaNo ratings yet
- TPG Alstom - Distance RelayDocument7 pagesTPG Alstom - Distance RelayFranz Erwin Gabriel FuentesNo ratings yet
- Jurnal 1Document8 pagesJurnal 1Dela Amelia Nur SalehaNo ratings yet
- BSC MSC PHD Scholarships by DR Oluseun Ajayi 1673218909 PDFDocument3 pagesBSC MSC PHD Scholarships by DR Oluseun Ajayi 1673218909 PDFInnocent MataazNo ratings yet
- Aceleradores Serie 6900Document2 pagesAceleradores Serie 6900jdavis5548No ratings yet
- Industry CPD: Modelling Buildings For Seismic AnalysisDocument4 pagesIndustry CPD: Modelling Buildings For Seismic Analysisshare4learnNo ratings yet
- SMAW WeldingDocument37 pagesSMAW Weldingvishwas salunkheNo ratings yet
- Selected Objective Question On Introduction To Computers With Answer Set 5Document27 pagesSelected Objective Question On Introduction To Computers With Answer Set 5Ankit JainNo ratings yet
- Ferrite Core Transformer Design Engineering and Technology 6Document10 pagesFerrite Core Transformer Design Engineering and Technology 6nedian_2006100% (1)
- The Main Factors Influencing Consumer Behavior Towards Bershka Store in KazakhstanDocument5 pagesThe Main Factors Influencing Consumer Behavior Towards Bershka Store in KazakhstanIJEMR JournalNo ratings yet
- 6.+ (1035) +Hasna+Nabikha+Khoirunnisa Determination+Of+Attitude+Using+Games+And+Purchase+Intentions+In+E-CommerceDocument21 pages6.+ (1035) +Hasna+Nabikha+Khoirunnisa Determination+Of+Attitude+Using+Games+And+Purchase+Intentions+In+E-CommerceJenzel DelavictoriaNo ratings yet