You might also like
- Making MethamphetamineDocument31 pagesMaking MethamphetamineFeisya NahlaNo ratings yet
- Asme B I Addenda: To Asme Metallic Gaskets For Pipe Flanges Ring-Joint, Spiral-Wound, and JacketedDocument51 pagesAsme B I Addenda: To Asme Metallic Gaskets For Pipe Flanges Ring-Joint, Spiral-Wound, and JacketedTimilehin OladiranNo ratings yet
- g12 2nd Folk, Ballet, BallroomDocument82 pagesg12 2nd Folk, Ballet, BallroomJennifer ArnaizNo ratings yet
- Role of World Bank in Developing CountriesDocument19 pagesRole of World Bank in Developing Countriesdrmz4you79% (14)
- Case Study Pre FinalDocument11 pagesCase Study Pre FinalJohn Russel Buenviaje Reyes0% (1)
- BMC Musculoskeletal DisordersDocument16 pagesBMC Musculoskeletal DisordersRogerDelaCernaNo ratings yet
- Tese SnotDocument16 pagesTese SnotCaio GonçalvesNo ratings yet
- Evaluation of An Interdisciplinary Screening Program For People With Parkinson Disease and Movement DisordersDocument10 pagesEvaluation of An Interdisciplinary Screening Program For People With Parkinson Disease and Movement DisordersAbu Faris Al-MandariNo ratings yet
- Impact of Spasticity On Quality of Life of Lebanese Individuals With Spinal Cord Injury Validity and Reliability of The Arabic Modified PatientDocument11 pagesImpact of Spasticity On Quality of Life of Lebanese Individuals With Spinal Cord Injury Validity and Reliability of The Arabic Modified PatientResearch and Development DepartmentNo ratings yet
- SUPER KIDZ Pain ScaleDocument10 pagesSUPER KIDZ Pain Scalepfi_jenNo ratings yet
- 1 s2.0 S152994301830634X MainDocument7 pages1 s2.0 S152994301830634X MainOana RuxandraNo ratings yet
- How Much Does The Dallas Pain Questionnaire Score Have To Improve To Indicate That Patients With Chronic Low Back Pain Feel Better or Well?Document6 pagesHow Much Does The Dallas Pain Questionnaire Score Have To Improve To Indicate That Patients With Chronic Low Back Pain Feel Better or Well?mitchNo ratings yet
- 10.1007@s00784 019 03188 1Document12 pages10.1007@s00784 019 03188 1Hélder MouraNo ratings yet
- Orebro Portuguese QOLR2015Document12 pagesOrebro Portuguese QOLR2015Ju ChangNo ratings yet
- E1134 The Effect of Logotherapy On Depression in Cancer Patients A Systematic Review StudyDocument6 pagesE1134 The Effect of Logotherapy On Depression in Cancer Patients A Systematic Review StudyfitranoenoeNo ratings yet
- Assesement 1Document6 pagesAssesement 1mono1144No ratings yet
- 641-Texto Del Artículo-1808-1-10-20210425Document27 pages641-Texto Del Artículo-1808-1-10-20210425Maximiliano AzconaNo ratings yet
- Gum Mess On 2003Document6 pagesGum Mess On 2003fajarcolzzzNo ratings yet
- 0 Heinemann2003 - Varias VersionesDocument4 pages0 Heinemann2003 - Varias VersionesALETA44No ratings yet
- Ijspt 14 845Document15 pagesIjspt 14 845Magno FilhoNo ratings yet
- Measuring The Impact of MigraineDocument11 pagesMeasuring The Impact of MigraineIdada EzekielNo ratings yet
- Sitasi 2Document7 pagesSitasi 2Silvia ManurungNo ratings yet
- Current Practice in The Rehabilitation of Complex Regional Pain Syndrome A Survey of PractitionersDocument8 pagesCurrent Practice in The Rehabilitation of Complex Regional Pain Syndrome A Survey of Practitionersgeschrich7No ratings yet
- Master's and Doctoral Programs in Physical TherapyDocument26 pagesMaster's and Doctoral Programs in Physical TherapyJu ChangNo ratings yet
- Carlozzi-14 RS Outcomes HDDocument20 pagesCarlozzi-14 RS Outcomes HDMARIA MONTSERRAT SOMOZA MONCADANo ratings yet
- Pressure Ulcer QoLDocument5 pagesPressure Ulcer QoLSevalNo ratings yet
- Functional Assessment of Cancer Therapy-Brain Questionnaire: Translation and Linguistic Adaptation To Brazilian PortugueseDocument6 pagesFunctional Assessment of Cancer Therapy-Brain Questionnaire: Translation and Linguistic Adaptation To Brazilian PortugueserudolfpeterssonNo ratings yet
- Effectiveness of Global Postural Re-Education For Treatment of Spinal Disorders A Meta-AnalysisDocument10 pagesEffectiveness of Global Postural Re-Education For Treatment of Spinal Disorders A Meta-AnalysisraquelbibiNo ratings yet
- Interventions For Treating Pain and Disability in Adults With Complex Regional Pain Syndrome-An Overview of Systematic ReviewsDocument5 pagesInterventions For Treating Pain and Disability in Adults With Complex Regional Pain Syndrome-An Overview of Systematic ReviewsmahunNo ratings yet
- Peer Role-Play and Standardised Patients in Communication Training A Comparative Study On The Student Perspective On Acceptability, Realism, and Perceived EffectDocument9 pagesPeer Role-Play and Standardised Patients in Communication Training A Comparative Study On The Student Perspective On Acceptability, Realism, and Perceived EffectAndré GuerraNo ratings yet
- Ventosa Na Dor LombarDocument7 pagesVentosa Na Dor Lombarmauricio da silva barbosaNo ratings yet
- Journal of ScienceDocument4 pagesJournal of ScienceEndang SetiawatiNo ratings yet
- Assessing Fatigue in The ESRD Patient: A Step Forward: Related Article, P. 327Document3 pagesAssessing Fatigue in The ESRD Patient: A Step Forward: Related Article, P. 327Rina FebriantiNo ratings yet
- RN Prescribing in General PracticeDocument12 pagesRN Prescribing in General PracticeAhmad IsmailNo ratings yet
- Health Related Quality of Life Among Pateints With Cronic Obstructive Pulmonary DiseaseDocument9 pagesHealth Related Quality of Life Among Pateints With Cronic Obstructive Pulmonary DiseaseOana D. RaduNo ratings yet
- Brazilian Version of The Berg Balance ScaleDocument11 pagesBrazilian Version of The Berg Balance ScaleWinter FigueiredoNo ratings yet
- 55.literature Review About Neurodevelopmental Approaches-1Document37 pages55.literature Review About Neurodevelopmental Approaches-1Zeeshan AhmadNo ratings yet
- An To Patient-Reported Outcome Measures (Proms) in PhysiotherapyDocument7 pagesAn To Patient-Reported Outcome Measures (Proms) in PhysiotherapyAline VidalNo ratings yet
- Helweg Joergensen2019Document12 pagesHelweg Joergensen2019Manon MorenoNo ratings yet
- Tveter 2014Document8 pagesTveter 2014Thays VotaçõesNo ratings yet
- HLTH 520 Reseach Appraisal - ResearchDocument16 pagesHLTH 520 Reseach Appraisal - Researchapi-479186899No ratings yet
- 1 s2.0 S1201971214017214 Main PDFDocument5 pages1 s2.0 S1201971214017214 Main PDFYohanna ekasntNo ratings yet
- The Outcome Rating Scale ArticleDocument24 pagesThe Outcome Rating Scale ArticleAdhie DarmawanNo ratings yet
- Does The Addition of Manual Therapy Approach To A Cervical Exercise Program Improve Clinical Outcomes For Patients With Chronic Neck Pain in Short - and Mid-Term? A Randomized Controlled Trial - PMCDocument26 pagesDoes The Addition of Manual Therapy Approach To A Cervical Exercise Program Improve Clinical Outcomes For Patients With Chronic Neck Pain in Short - and Mid-Term? A Randomized Controlled Trial - PMCEri KafexhiNo ratings yet
- Review Article: Efficacy and Safety of Medicinal Plants or Related Natural Products For Fibromyalgia: A Systematic ReviewDocument11 pagesReview Article: Efficacy and Safety of Medicinal Plants or Related Natural Products For Fibromyalgia: A Systematic ReviewPablo IgnacioNo ratings yet
- Delphi Self MangementDocument41 pagesDelphi Self Mangementrespaldonatie4No ratings yet
- A Short Questionnaire For The Assessment of Quality of Life in Patients With Chronic Obstructive Pulmonary Disease: Psychometric Properties of VQ11Document11 pagesA Short Questionnaire For The Assessment of Quality of Life in Patients With Chronic Obstructive Pulmonary Disease: Psychometric Properties of VQ11elonaNo ratings yet
- 5 - LOW-BACK-PAIN-AMONG-OCCUPATIONAL-THE5 - RAPISTS-AND-ITS-ASSOCIATED-RISK-FACTORSMalaysian-Journal-of-Public-Health-MedicineDocument12 pages5 - LOW-BACK-PAIN-AMONG-OCCUPATIONAL-THE5 - RAPISTS-AND-ITS-ASSOCIATED-RISK-FACTORSMalaysian-Journal-of-Public-Health-MedicineYANETH PATRICIA BARÓN OSORIONo ratings yet
- The Development and Validation of A Disease-Specific Quality of Life Measure in Hyperhidrosis: The Hyperhidrosis Quality of Life Index (Hidroqol !)Document11 pagesThe Development and Validation of A Disease-Specific Quality of Life Measure in Hyperhidrosis: The Hyperhidrosis Quality of Life Index (Hidroqol !)mleazeNo ratings yet
- Rhinosinusitis - Its Impact On Quality of Life: 3 Medical Faculty of Charles University, Prague Czech RepublicDocument25 pagesRhinosinusitis - Its Impact On Quality of Life: 3 Medical Faculty of Charles University, Prague Czech RepublicBlebea CristinaNo ratings yet
- Cardoso Et Al. 2020Document17 pagesCardoso Et Al. 2020MeltemNo ratings yet
- Jurnal LV Ipd 6Document12 pagesJurnal LV Ipd 6Dudeperfect666No ratings yet
- Articulo 8 AlejoDocument22 pagesArticulo 8 AlejoAngelaVillegasNo ratings yet
- Translating The Research Diagnostic Criteria For Temporomandibular Disorders Into Malay: Evaluation of Content and ProcessDocument0 pagesTranslating The Research Diagnostic Criteria For Temporomandibular Disorders Into Malay: Evaluation of Content and ProcessUniversity Malaya's Dental Sciences ResearchNo ratings yet
- Clinical Classification in Low Back Pain Best-Evidence Diagnostic Rules Based On Systematic ReviewsDocument24 pagesClinical Classification in Low Back Pain Best-Evidence Diagnostic Rules Based On Systematic ReviewsReyn JohnsonNo ratings yet
- A Treatment Schedule of Conventional Physical Therapy Provided To Enhance Upper Limb Sensorimotor Recovery After Stroke Expert Criterion Validity and Intra-Rater ReliabilityDocument10 pagesA Treatment Schedule of Conventional Physical Therapy Provided To Enhance Upper Limb Sensorimotor Recovery After Stroke Expert Criterion Validity and Intra-Rater ReliabilityGeraldo MoraesNo ratings yet
- Intervention Strategies For Improving Patient AdherenceDocument8 pagesIntervention Strategies For Improving Patient AdherenceIon Arrieta ValeroNo ratings yet
- Core OmDocument25 pagesCore OmCristina SencalNo ratings yet
- Ebp Final DraftDocument14 pagesEbp Final Draftapi-436039292No ratings yet
- His 9Document158 pagesHis 9Anjum100% (6)
- Yjmt 30 1992090Document13 pagesYjmt 30 1992090Luis Sebastian Arango OspinaNo ratings yet
- Clinical Global Impression-Severity Score As A Reliable Measure For Routine Evaluation of Remission in Schizophrenia and Schizoaffective DisordersDocument8 pagesClinical Global Impression-Severity Score As A Reliable Measure For Routine Evaluation of Remission in Schizophrenia and Schizoaffective DisordersSadia ShafaqueNo ratings yet
- Ebp PaperDocument16 pagesEbp Paperapi-583545759No ratings yet
- 2017-Ugo Chukwu-International Journal of Medicine and PharmacyDocument10 pages2017-Ugo Chukwu-International Journal of Medicine and PharmacyNurettin AbacıoğluNo ratings yet
- Therapy Response Imaging in OncologyFrom EverandTherapy Response Imaging in OncologyMizuki NishinoNo ratings yet
- Yao2017 PDFDocument27 pagesYao2017 PDFArie BaldwellNo ratings yet
- 149 901 1 PBDocument9 pages149 901 1 PBArie BaldwellNo ratings yet
- Selfeficacti Quest PDFDocument10 pagesSelfeficacti Quest PDFArie BaldwellNo ratings yet
- 2047487315569401Document13 pages2047487315569401Arie BaldwellNo ratings yet
- 10 18621-Eurj 383180-482288Document9 pages10 18621-Eurj 383180-482288Arie BaldwellNo ratings yet
- Ethics SummitDocument12 pagesEthics SummitArie BaldwellNo ratings yet
- Nursing Philosophy - 2019 - Schiller - But It S Legal Isn T It Law and Ethics in Nursing Practice Related To MedicalDocument11 pagesNursing Philosophy - 2019 - Schiller - But It S Legal Isn T It Law and Ethics in Nursing Practice Related To MedicalArie BaldwellNo ratings yet
- Ethical ClimateDocument16 pagesEthical ClimateArie BaldwellNo ratings yet
- Davidsin, KurtDocument22 pagesDavidsin, KurtArie BaldwellNo ratings yet
- Cerit&DincDocument14 pagesCerit&DincArie BaldwellNo ratings yet
- Chen, S., Et - Al. (2020) - (01-11)Document11 pagesChen, S., Et - Al. (2020) - (01-11)Vielia IrmayantiNo ratings yet
- NSS - Ass 3 - 120ar0010Document3 pagesNSS - Ass 3 - 120ar0010Arpita SahooNo ratings yet
- Maternal and Child Health (MHCH)Document4 pagesMaternal and Child Health (MHCH)rifkatu s. ibrahimNo ratings yet
- Rekha D PDFDocument3 pagesRekha D PDFAbhishek ShrivastavNo ratings yet
- Spa ServicesDocument2 pagesSpa ServicesmozarellarosesNo ratings yet
- Parkell Sensimatic 600SE Electrosurge: Important-Read FirstDocument8 pagesParkell Sensimatic 600SE Electrosurge: Important-Read FirstIPPRS RSBKEDIRINo ratings yet
- Obat Tahap 3Document7 pagesObat Tahap 3kulanavhieaNo ratings yet
- CHN1 Worksheet1Document5 pagesCHN1 Worksheet1Chariza MayNo ratings yet
- HRM ReportDocument8 pagesHRM ReportHumayonkabir ShakilNo ratings yet
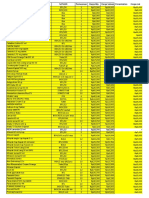
- Pt. Indra Giri Raya: Kode Nama Barang Stock Harga Jual SatuanDocument12 pagesPt. Indra Giri Raya: Kode Nama Barang Stock Harga Jual Satuanrema_rhere95No ratings yet
- BA-BE Study Design and ProtocolDocument6 pagesBA-BE Study Design and ProtocolvarishNo ratings yet
- Endometriosis The Pathophysiology As An Estrogen-Dependent DiseaseDocument7 pagesEndometriosis The Pathophysiology As An Estrogen-Dependent DiseaseHarrison BungasaluNo ratings yet
- Ellis 2023 HandoutsDocument26 pagesEllis 2023 HandoutsJalfeNo ratings yet
- Sample Essays - WiproDocument17 pagesSample Essays - Wiprojansi Vadiyala150% (1)
- The Concept of Necropolitics During The Pandemic of Covid-19 in BrazilDocument26 pagesThe Concept of Necropolitics During The Pandemic of Covid-19 in BrazilLaize RodriguesNo ratings yet
- Tooth Positions On Complete Dentures : David M. WattDocument14 pagesTooth Positions On Complete Dentures : David M. WattArun PrasadNo ratings yet
- Laboratory Technology Course Catalogue LastDocument9 pagesLaboratory Technology Course Catalogue LastBiruk MilionNo ratings yet
- Main - Employee Performance Appraisal FormDocument3 pagesMain - Employee Performance Appraisal FormPalak SinghalNo ratings yet
- Pigmented Lesions of The Skin That You Must Diagnose With ConfidenceDocument23 pagesPigmented Lesions of The Skin That You Must Diagnose With ConfidenceDeba P SarmaNo ratings yet
- Juvinile Delinquency PDFDocument8 pagesJuvinile Delinquency PDFavniNo ratings yet
- Tos - Tle 10Document2 pagesTos - Tle 10May ann BulanNo ratings yet
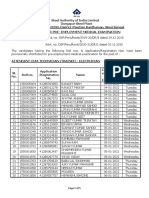
- Notice For PEMEDocument5 pagesNotice For PEMESwarnava LahaNo ratings yet
- Waste Management and Effect To Our EnvironmentDocument31 pagesWaste Management and Effect To Our EnvironmentKeila BayauaNo ratings yet
- Challenges and Issues Faced Concerning ECEDocument4 pagesChallenges and Issues Faced Concerning ECEShiera GannabanNo ratings yet
- Yeast Extrac AgarDocument2 pagesYeast Extrac AgarMegawati KusumaNo ratings yet