You might also like
- The Quality and Reporting of Randomized Trials in Cardiothoracic Physical Therapy Could Be Substantially ImprovedDocument8 pagesThe Quality and Reporting of Randomized Trials in Cardiothoracic Physical Therapy Could Be Substantially ImprovedJu ChangNo ratings yet
- Spin Abstracts Back PainDocument28 pagesSpin Abstracts Back Paincaio sachettiNo ratings yet
- Gordon Et Al., (2019) Efecct of Pulmonary Rehabilitation On Symptoms of Anxiety and Depression in Chronic Obstructive Pulmonary DiseaseDocument12 pagesGordon Et Al., (2019) Efecct of Pulmonary Rehabilitation On Symptoms of Anxiety and Depression in Chronic Obstructive Pulmonary DiseaseAna Flávia SordiNo ratings yet
- DFHDF DFJKJK DFDocument8 pagesDFHDF DFJKJK DFAndrés Araneda VásquezNo ratings yet
- 2016 Slade CERTDocument30 pages2016 Slade CERTdamicarbo_297070015No ratings yet
- Rehabilitación CardiacaDocument17 pagesRehabilitación Cardiacamsq.cv5919No ratings yet
- Evaluation of Knowledge and Practices of PhysicalDocument6 pagesEvaluation of Knowledge and Practices of Physicalbesho 2013No ratings yet
- 10 1016@J Jphys 2019 08 005Document1 page10 1016@J Jphys 2019 08 005Tote Cifuentes AmigoNo ratings yet
- Jurnal Keperawatan MuhammadiyahDocument11 pagesJurnal Keperawatan MuhammadiyahSofa MarwahNo ratings yet
- Planning A Change ProjectDocument7 pagesPlanning A Change Projectsaima anwarNo ratings yet
- Carlozzi-14 RS Outcomes HDDocument20 pagesCarlozzi-14 RS Outcomes HDMARIA MONTSERRAT SOMOZA MONCADANo ratings yet
- Dec14 16 PDFDocument7 pagesDec14 16 PDFijasrjournalNo ratings yet
- Evaluation of An Interdisciplinary Screening Program For People With Parkinson Disease and Movement DisordersDocument10 pagesEvaluation of An Interdisciplinary Screening Program For People With Parkinson Disease and Movement DisordersAbu Faris Al-MandariNo ratings yet
- Medi 100 E26976Document13 pagesMedi 100 E26976Nur Afifah TadaengNo ratings yet
- Ann Rheum Dis 2013 Edwards Annrheumdis 2013 203913Document10 pagesAnn Rheum Dis 2013 Edwards Annrheumdis 2013 203913rizki amaiNo ratings yet
- Boutron 10Document10 pagesBoutron 10Fernando GómezNo ratings yet
- 02 Reference For ElevationDocument8 pages02 Reference For ElevationFederico BristotNo ratings yet
- TIDieR InglésDocument12 pagesTIDieR InglésPG TavoNo ratings yet
- BMJ g1687 FullDocument12 pagesBMJ g1687 FullJaumeNo ratings yet
- RC0602 Prolotherapy FinalDocument42 pagesRC0602 Prolotherapy Finalesma bekirogluNo ratings yet
- Satisfaction Levels With Physical Therapy in Hospitalized PatientsDocument6 pagesSatisfaction Levels With Physical Therapy in Hospitalized PatientscarolciveNo ratings yet
- The Effectiveness of Physiotherapy in The Management of Temporomandibular DisordersDocument11 pagesThe Effectiveness of Physiotherapy in The Management of Temporomandibular DisordersLaura Espejo SalamancaNo ratings yet
- 2014 145 1 1 1 PandisDocument1 page2014 145 1 1 1 PandisAlla MushkeyNo ratings yet
- 1111 PDFDocument355 pages1111 PDFJameel KhanNo ratings yet
- TIDie RDocument12 pagesTIDie RBruno SantinonNo ratings yet
- HLTH 520 Reseach Appraisal - ResearchDocument16 pagesHLTH 520 Reseach Appraisal - Researchapi-479186899No ratings yet
- 1106 FullDocument14 pages1106 Fullmarcos viniciusNo ratings yet
- Clinimetric Analyses of The Modified Parkinson Activity Scale PDFDocument7 pagesClinimetric Analyses of The Modified Parkinson Activity Scale PDFdanielNo ratings yet
- CARE Guidelines For Case ReportingDocument7 pagesCARE Guidelines For Case ReportingPriyanka SharmaNo ratings yet
- Assessment of Pharmacist-Led Patient Counseling in Randomized Controlled Trials: A Systematic ReviewDocument11 pagesAssessment of Pharmacist-Led Patient Counseling in Randomized Controlled Trials: A Systematic ReviewNishant ShresthaNo ratings yet
- 1106 FullDocument14 pages1106 Fullnanthini kanasanNo ratings yet
- Li 2019Document9 pagesLi 2019Ade Cahyo IslamiNo ratings yet
- Clinical Practice Guidelines For Nursing - and HealDocument24 pagesClinical Practice Guidelines For Nursing - and HealHAMNA ZAINABNo ratings yet
- Guidelines For Perioperative Care For Pancreaticoduodenectomy WJSDocument19 pagesGuidelines For Perioperative Care For Pancreaticoduodenectomy WJSFelipe BerbertNo ratings yet
- JURNAL 26 NadaDocument18 pagesJURNAL 26 NadaResky Ika Sah PutriNo ratings yet
- Ebp Final DraftDocument14 pagesEbp Final Draftapi-436039292No ratings yet
- Journal of Yoga and Physical TherapyDocument1 pageJournal of Yoga and Physical Therapykhadesakshi55No ratings yet
- Randomized Controlled Trial Quality in Pediatric Physical TherapyDocument14 pagesRandomized Controlled Trial Quality in Pediatric Physical TherapyMelinda Fila BethaNo ratings yet
- 2013 Consort ProDocument9 pages2013 Consort ProSiney De la CruzNo ratings yet
- Management of Plantar Heel Pain: A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesDocument14 pagesManagement of Plantar Heel Pain: A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesMaximiliano LabraNo ratings yet
- Psychiatry ResearchDocument12 pagesPsychiatry ResearchErse Kusuma EndraswariNo ratings yet
- The Effects of Pay-for-Performance Programs On Health, Health Care Use, and Processes of CareDocument14 pagesThe Effects of Pay-for-Performance Programs On Health, Health Care Use, and Processes of CareMasrun FatanahNo ratings yet
- MCFARLANE - 2016 - ARD - EULAR-recommendations - FibromyalgiaDocument11 pagesMCFARLANE - 2016 - ARD - EULAR-recommendations - FibromyalgiaTata2666No ratings yet
- Management of Plantar Heel Pain. A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesDocument14 pagesManagement of Plantar Heel Pain. A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesJesusNavarrete97No ratings yet
- Efficacy of Computer Based Developmental Pediatric Screening (CBDPS)Document5 pagesEfficacy of Computer Based Developmental Pediatric Screening (CBDPS)RuchitaNo ratings yet
- Jamda: Clinical ExperienceDocument6 pagesJamda: Clinical ExperienceDivine Mercy De JulianNo ratings yet
- Functional Outcome Measures in Physiotherapybridging Evidence Based Practice Function and Our Future 2165 7025.1000e106Document2 pagesFunctional Outcome Measures in Physiotherapybridging Evidence Based Practice Function and Our Future 2165 7025.1000e106Tirumala RaoNo ratings yet
- Reporting of Patient-Reported Outcomes in Randomized Trials: The CONSORT PRO ExtensionDocument9 pagesReporting of Patient-Reported Outcomes in Randomized Trials: The CONSORT PRO ExtensionPAULA ALEJANDRA MARTIN RAMIREZNo ratings yet
- Effectiveness of Formal Physical Therapy Following Total Shoulder Arthroplasty: A Systematic ReviewDocument8 pagesEffectiveness of Formal Physical Therapy Following Total Shoulder Arthroplasty: A Systematic ReviewBüşra YılmazNo ratings yet
- ERS Statement On Standardisation of Cardiopulmonary Exercise Testing in Chronic Lung DiseasesDocument25 pagesERS Statement On Standardisation of Cardiopulmonary Exercise Testing in Chronic Lung Diseasesnatalia cunha varellaNo ratings yet
- Tos CronicaDocument12 pagesTos CronicasaloNo ratings yet
- Jurnal PendukungDocument5 pagesJurnal PendukungrekaNo ratings yet
- Jurnal PendukungDocument5 pagesJurnal PendukungrekaNo ratings yet
- Thorell2016 Article GuidelinesForPerioperativeCareDocument19 pagesThorell2016 Article GuidelinesForPerioperativeCareDiego CadenaNo ratings yet
- Guidelines For Perioperative Care in Bariatric SurgeryDocument23 pagesGuidelines For Perioperative Care in Bariatric Surgerymilagros12300No ratings yet
- Referral To Rehabilitation in Parkinson's Disease Who, When and To What EndDocument6 pagesReferral To Rehabilitation in Parkinson's Disease Who, When and To What EndFrancisco Ahumada MéndezNo ratings yet
- Alcohol and Low Back Pain A Systematic Literature ReviewDocument4 pagesAlcohol and Low Back Pain A Systematic Literature RevieweubvhsvkgNo ratings yet
- The Knee Society Short Form Reduces Respondent Burden in The Assessment of Patient-Reported OutcomesDocument9 pagesThe Knee Society Short Form Reduces Respondent Burden in The Assessment of Patient-Reported OutcomesSantiago Mondragon RiosNo ratings yet
- 10 1016@j JHT 2017 02 001 PDFDocument10 pages10 1016@j JHT 2017 02 001 PDFGusti Ayu KrisnayantiNo ratings yet
- What Does Clinically Important Really Mean AJP 2008Document2 pagesWhat Does Clinically Important Really Mean AJP 2008Ju ChangNo ratings yet
- Visa - P, Jospt 2013Document9 pagesVisa - P, Jospt 2013Ju ChangNo ratings yet
- Use of Placebo Controls in Clinical Research - Trials2012Document7 pagesUse of Placebo Controls in Clinical Research - Trials2012Ju ChangNo ratings yet
- Manual TherapyDocument14 pagesManual TherapyJu ChangNo ratings yet
- Which One Is The Best, Spine 2008Document5 pagesWhich One Is The Best, Spine 2008Ju ChangNo ratings yet
- What Are The Main Running Related Musculoskeletal.6Document15 pagesWhat Are The Main Running Related Musculoskeletal.6Ju ChangNo ratings yet
- Us SR PTJ, 2009Document15 pagesUs SR PTJ, 2009Ju ChangNo ratings yet
- Transparent Reporting English RBF2011Document5 pagesTransparent Reporting English RBF2011Ju ChangNo ratings yet
- Treatment Based Subgroups LBP 2010Document11 pagesTreatment Based Subgroups LBP 2010Ju ChangNo ratings yet
- Tatiane BJPT 2015Document10 pagesTatiane BJPT 2015Ju ChangNo ratings yet
- Shoulder CCA Questionnaires, JOSPT 2013Document10 pagesShoulder CCA Questionnaires, JOSPT 2013Ju ChangNo ratings yet
- Responsiveness PSFS Vs RMDQ - ESJ2010Document8 pagesResponsiveness PSFS Vs RMDQ - ESJ2010Ju ChangNo ratings yet
- TSK Xfabq Spine 2008Document6 pagesTSK Xfabq Spine 2008Ju ChangNo ratings yet
- Manual TherapyDocument14 pagesManual TherapyJonathan BaldeonNo ratings yet
- SR Cross Cultural AdaptationsDocument10 pagesSR Cross Cultural AdaptationsJu ChangNo ratings yet
- PF Scales, Jospt 2013Document11 pagesPF Scales, Jospt 2013Ju ChangNo ratings yet
- Manual Therapy: Susan Armijo-Olivo, Sharon Warren, Jorge Fuentes, David J. MageeDocument10 pagesManual Therapy: Susan Armijo-Olivo, Sharon Warren, Jorge Fuentes, David J. MageeJu ChangNo ratings yet
- Recall BiasDocument9 pagesRecall BiasJu ChangNo ratings yet
- Reporting of SR in Portuguese - RBF 2012Document8 pagesReporting of SR in Portuguese - RBF 2012Ju ChangNo ratings yet
- MedRisk - Índice de Satisfação Do PacienteDocument11 pagesMedRisk - Índice de Satisfação Do PacienteScientifica EducacionalNo ratings yet
- Pilates Cochrane Full 2015Document73 pagesPilates Cochrane Full 2015Ju ChangNo ratings yet
- Orebro Portuguese QOLR2015Document12 pagesOrebro Portuguese QOLR2015Ju ChangNo ratings yet
- Menezes Costa CMAJ 2012 (SR of Prognosis of Low Back Pain and Commentary)Document14 pagesMenezes Costa CMAJ 2012 (SR of Prognosis of Low Back Pain and Commentary)Ju ChangNo ratings yet
- PEDro Portuguese CSP2011Document5 pagesPEDro Portuguese CSP2011Ju ChangNo ratings yet
- P Values Effect SizesDocument2 pagesP Values Effect SizesJu ChangNo ratings yet
- Missing Data and Multi ImputationDocument5 pagesMissing Data and Multi ImputationJu ChangNo ratings yet
- KTversusmicropore, BJPT2015Document9 pagesKTversusmicropore, BJPT2015Ju ChangNo ratings yet
- KT Trial Added JOSPT2016Document8 pagesKT Trial Added JOSPT2016Ju ChangNo ratings yet
- MDT Secondary Analysis - PTJ 2016Document10 pagesMDT Secondary Analysis - PTJ 2016Ju ChangNo ratings yet
- Elecsys T4: Cobas e 411 Cobas e 601 Cobas e 602 English System InformationDocument5 pagesElecsys T4: Cobas e 411 Cobas e 601 Cobas e 602 English System InformationIsmael CulquiNo ratings yet
- Labor To DigestDocument32 pagesLabor To Digestphoenix rogueNo ratings yet
- (Nikolaj Wolfson, Alexander Lerner, Leonid Roshal (B-Ok - CC)Document589 pages(Nikolaj Wolfson, Alexander Lerner, Leonid Roshal (B-Ok - CC)Andi sutandi100% (1)
- "Unadulterated" - The Organic and Ethnic - For Vegetarians and Non-VegetariansDocument21 pages"Unadulterated" - The Organic and Ethnic - For Vegetarians and Non-VegetariansShilpa PatilNo ratings yet
- Mechanical Operation Slurry TransportDocument113 pagesMechanical Operation Slurry TransportIsrarulHaqueNo ratings yet
- Coronavirus Reported SpeechDocument1 pageCoronavirus Reported SpeechGabiZ - Kalifato SurNo ratings yet
- Nasoalveolar Moulding Seminar at MalakkaraDocument54 pagesNasoalveolar Moulding Seminar at MalakkaraAshwin100% (1)
- Name of Learner: Section: Subject Teacher: Date:: Practical Research 2Document4 pagesName of Learner: Section: Subject Teacher: Date:: Practical Research 2J-heart Basabas Malpal100% (6)
- Judicial Affidavit - P:CPL PolutanDocument2 pagesJudicial Affidavit - P:CPL PolutanRain HofileñaNo ratings yet
- Rigatoni With Beef and Onion RaguDocument3 pagesRigatoni With Beef and Onion RagumadduxdavidNo ratings yet
- Policy and Procedures For Hiring, PromotionsDocument2 pagesPolicy and Procedures For Hiring, PromotionsRazel Ann ElagioNo ratings yet
- CoC VampireCharacterPrimerPDFDocument5 pagesCoC VampireCharacterPrimerPDFDavid Alexander TomblinNo ratings yet
- 150.66-RP4 YcalDocument92 pages150.66-RP4 YcalJosé RamosNo ratings yet
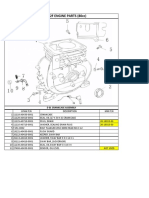
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- Compact Water Treatment 200 m3Document3 pagesCompact Water Treatment 200 m3civil eng915No ratings yet
- Neonatal SepsisDocument29 pagesNeonatal SepsisElton Ndhlovu100% (3)
- Bylaws-Craigs Mill Hoa 2013Document10 pagesBylaws-Craigs Mill Hoa 2013api-243024250No ratings yet
- Physical, Biology and Chemical Environment: Its Effect On Ecology and Human HealthDocument24 pagesPhysical, Biology and Chemical Environment: Its Effect On Ecology and Human Health0395No ratings yet
- Fleming Trio-E Promotional SheetDocument2 pagesFleming Trio-E Promotional SheetRed BarnNo ratings yet
- CORONADocument25 pagesCORONAMohammedNo ratings yet
- Natural Medicine - 2016 October PDFDocument100 pagesNatural Medicine - 2016 October PDFDinh Ta HoangNo ratings yet
- Annual Report Ministry of Social JusticeDocument262 pagesAnnual Report Ministry of Social JusticeBhargav RamNo ratings yet
- Alcohol Facts and Statistics: Alcohol Use in The United StatesDocument6 pagesAlcohol Facts and Statistics: Alcohol Use in The United StatesVictor EnemNo ratings yet
- Cation Ion Exchange CapacityDocument1 pageCation Ion Exchange CapacityGopal MallickNo ratings yet
- Lesson Plan Personality DisorderDocument7 pagesLesson Plan Personality DisorderRaj MeghwalNo ratings yet
- Key MechanicalDocument72 pagesKey MechanicalDasuki FahmiNo ratings yet
- Arduino CertificationDocument8 pagesArduino Certificationhack reportNo ratings yet
- Hydraulic Seat Puller KitDocument2 pagesHydraulic Seat Puller KitPurwanto ritzaNo ratings yet
- Kualitas Hidup Lanjut Usia Yang Tinggal Di Panti: Studi Literatur Majesty Kowureng, Carla Kairupan, KristamulianaDocument15 pagesKualitas Hidup Lanjut Usia Yang Tinggal Di Panti: Studi Literatur Majesty Kowureng, Carla Kairupan, KristamulianaVita AmiliaNo ratings yet
- Substation Basic PDFDocument6 pagesSubstation Basic PDFSaraswatapalitNo ratings yet