You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Types of AnesthesiaDocument3 pagesTypes of AnesthesiaJabber PaudacNo ratings yet
- A Diagnostic Chest Xray: Multiple Myeloma: Daniela Marinho Tridente, Vi FCMSCSP Gillian Lieberman, MDDocument44 pagesA Diagnostic Chest Xray: Multiple Myeloma: Daniela Marinho Tridente, Vi FCMSCSP Gillian Lieberman, MDGani ArlondNo ratings yet
- Equipments and Supplies 4 HospitalDocument4 pagesEquipments and Supplies 4 HospitalSujatha J Jayabal100% (1)
- Streptococci: General Characteristics of StreptococciDocument13 pagesStreptococci: General Characteristics of Streptococcidevesh.hsNo ratings yet
- Hospital Information SystemsDocument32 pagesHospital Information SystemsabhiramghadaiNo ratings yet
- NimbexDocument35 pagesNimbexfad12345No ratings yet
- Hemovigilancia ISBT 2011Document12 pagesHemovigilancia ISBT 2011Leonardo Borges dos SantosNo ratings yet
- Non Invasive Methods of Estimating Pharmacokinetic Parameters2Document31 pagesNon Invasive Methods of Estimating Pharmacokinetic Parameters2Thilak Chandra50% (2)
- Bruchon SchweitzerBIQPMS2002Document11 pagesBruchon SchweitzerBIQPMS2002Gabriela UretuNo ratings yet
- Internal Medicine Summary Notes - GI Bleed (Markdown Formatted)Document2 pagesInternal Medicine Summary Notes - GI Bleed (Markdown Formatted)ArgonDoubleNo ratings yet
- IMRD Grid: Assignment # 2 Fill Out The Table With 8-10 Scholarly Citations Containing Both Argument and CounterargumentDocument2 pagesIMRD Grid: Assignment # 2 Fill Out The Table With 8-10 Scholarly Citations Containing Both Argument and CounterargumentAneelaNo ratings yet
- Neomune PelniDocument57 pagesNeomune PelniSutiyono TyoNo ratings yet
- Cbahi Esr Standards PDFDocument10 pagesCbahi Esr Standards PDFjoan olanteNo ratings yet
- PCT and PropranololDocument6 pagesPCT and Propranololniken retnoNo ratings yet
- Life in The AsylumDocument6 pagesLife in The AsylumShadrach DareNo ratings yet
- WVCH Health Plan ContractDocument185 pagesWVCH Health Plan ContractStatesman JournalNo ratings yet
- IBM WatsonDocument15 pagesIBM WatsonshubuxavNo ratings yet
- A To Z Orthodontics Vol 8 CephalometryDocument17 pagesA To Z Orthodontics Vol 8 CephalometryYury Tenorio Cahuana50% (2)
- Professional Role Development PlanDocument10 pagesProfessional Role Development Planapi-5327002330% (1)
- Adeeko YetundeDocument2 pagesAdeeko YetundeAdeeko YetundeNo ratings yet
- Chamberlain Philosophy Intro PageDocument2 pagesChamberlain Philosophy Intro Pageapi-283996515No ratings yet
- Metabolic Encephalopathy: Behind The Name: TerminologyDocument3 pagesMetabolic Encephalopathy: Behind The Name: TerminologyKARINA ORMACHEANo ratings yet
- Indian Mbbs PatternDocument4 pagesIndian Mbbs PatternArpit SadhuNo ratings yet
- Emergency NursingDocument40 pagesEmergency NursingEstherThompson100% (8)
- Incision and DrainageDocument35 pagesIncision and DrainageVilma Delos Reyes100% (1)
- The Neurology of ProverbsDocument20 pagesThe Neurology of ProverbsDiogo FernandesNo ratings yet
- Chest InjuryDocument3 pagesChest Injurysofia yapNo ratings yet
- Paul E. Marik, MD, FCCM Mark Flemmer, MD Wendy Harrison, PHDDocument7 pagesPaul E. Marik, MD, FCCM Mark Flemmer, MD Wendy Harrison, PHDAde Triansyah EmsilNo ratings yet
- Tertiary Prevention of Disease - DiabetesDocument25 pagesTertiary Prevention of Disease - DiabetesMuhammad Na'im100% (5)
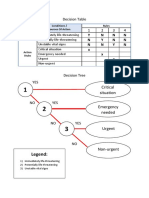
- Decision Table - Tim PDFDocument3 pagesDecision Table - Tim PDFNadia CasmerNo ratings yet