You might also like
- Mathematics For Engineers - Croft & Davison - Parte1Document260 pagesMathematics For Engineers - Croft & Davison - Parte1MarioNo ratings yet
- CRT TV Power ProblemDocument15 pagesCRT TV Power ProblemJoy Chowdhury50% (2)
- Cramers Rule 3 by 3 NotesDocument4 pagesCramers Rule 3 by 3 NotesSaherNo ratings yet
- ProjectDocument18 pagesProjectapi-525983464No ratings yet
- Global State of SunscreensDocument19 pagesGlobal State of SunscreensKenit PatelNo ratings yet
- Sunscreening Agents: A ReviewDocument11 pagesSunscreening Agents: A ReviewNaveen KumarNo ratings yet
- Determination of Sun Protection Factor by Uvvis Spectrophotometry - hccr.1000108Document4 pagesDetermination of Sun Protection Factor by Uvvis Spectrophotometry - hccr.1000108rnd labNo ratings yet
- Hyster H1.50XM (D001) Parts ManualDocument404 pagesHyster H1.50XM (D001) Parts ManualПетр75% (4)
- Basic Programming XRC PDFDocument204 pagesBasic Programming XRC PDFOscar SaucedoNo ratings yet
- Resumen Congreso 2017Document251 pagesResumen Congreso 2017M Victoria SalazarNo ratings yet
- SPPM Notes 1Document12 pagesSPPM Notes 1kokiladevirajaveluNo ratings yet
- Biology IA FinalDocument12 pagesBiology IA FinalAndrea ClavijoNo ratings yet
- SunscreenDocument8 pagesSunscreenmonitamiftahNo ratings yet
- Relationship Between Sun-Protection Factor and Application Thickness in High-Performance Sunscreen: Double Application of Sunscreen Is RecommendedDocument6 pagesRelationship Between Sun-Protection Factor and Application Thickness in High-Performance Sunscreen: Double Application of Sunscreen Is RecommendedArkantos TirbaNo ratings yet
- Broad-Spectrum Sunscreens Offer Protection Against Urocanic Acid Photoisomerization by Arti®cial Ultraviolet Radiation in Human SkinDocument6 pagesBroad-Spectrum Sunscreens Offer Protection Against Urocanic Acid Photoisomerization by Arti®cial Ultraviolet Radiation in Human SkinFenni OktoberryNo ratings yet
- Powerpoint JR NelsiDocument29 pagesPowerpoint JR NelsiNelsi Mellisa DewiNo ratings yet
- Methods That Is Most Robust and Accurate Compared To Equivalent In-Vivo SPF Tests in Predictive In-Vitro SPF MethodDocument4 pagesMethods That Is Most Robust and Accurate Compared To Equivalent In-Vivo SPF Tests in Predictive In-Vitro SPF MethodRosalie BachillerNo ratings yet
- Foto Prote To ResDocument19 pagesFoto Prote To ResEryandson MoraisNo ratings yet
- (Sinecatechins: Key ReferencesDocument14 pages(Sinecatechins: Key ReferencesFerdy Arif FadhilahNo ratings yet
- Accepted Manuscript: 10.1016/j.jaad.2017.12.062Document30 pagesAccepted Manuscript: 10.1016/j.jaad.2017.12.062Dave AbrahamNo ratings yet
- Oral Photoprotection: Effective Agents and Potential CandidatesDocument19 pagesOral Photoprotection: Effective Agents and Potential CandidatesThaís SagratzhiNo ratings yet
- Sunscreens: Obtaining Adequate Photoprotection: Mark E. Burnett, Judy Y. Hu & Steven Q. WangDocument8 pagesSunscreens: Obtaining Adequate Photoprotection: Mark E. Burnett, Judy Y. Hu & Steven Q. WangCpa cpaNo ratings yet
- Sunscreen App at The BeachDocument7 pagesSunscreen App at The BeachBryan NguyenNo ratings yet
- Are Cosmetic Products Which Include An S PDFDocument6 pagesAre Cosmetic Products Which Include An S PDFdewidiah31No ratings yet
- Research Article in Vitro Assessment of Sunscreen Efficacy Using Fourier Transform Infrared (FTIR) Spectroscopy On Synthetic SkinDocument11 pagesResearch Article in Vitro Assessment of Sunscreen Efficacy Using Fourier Transform Infrared (FTIR) Spectroscopy On Synthetic SkinJanavi MotwaniNo ratings yet
- 2023 Sunscreens Misconceptions and MisinformationDocument6 pages2023 Sunscreens Misconceptions and MisinformationBelen CoronaNo ratings yet
- Human Use of Sunscreens: AvailabilityDocument40 pagesHuman Use of Sunscreens: AvailabilityTamásHankovszkiNo ratings yet
- Formulation and Characterization of Sunscreen Creams With Synergistic EfficacyDocument6 pagesFormulation and Characterization of Sunscreen Creams With Synergistic EfficacydewiNo ratings yet
- Kosmetik 4Document1 pageKosmetik 4Aji SakaNo ratings yet
- Daily Use of Sunscreen PDFDocument8 pagesDaily Use of Sunscreen PDFNelsi Mellisa DewiNo ratings yet
- Here Comes SummerDocument2 pagesHere Comes SummerLazar CrinaNo ratings yet
- ArtigoDocument8 pagesArtigoDaniela HaltiNo ratings yet
- Analysis of Immediate Use of Sunscreen After MicroneedlingDocument20 pagesAnalysis of Immediate Use of Sunscreen After MicroneedlingTais Amadio MenegatNo ratings yet
- Sayre 1979Document8 pagesSayre 1979AnisaLastriNo ratings yet
- Photochem Photobiology - 2022 - Aguilera - Sun Protective Properties of Technical Sportswear Fabrics 100 Polyester TheDocument9 pagesPhotochem Photobiology - 2022 - Aguilera - Sun Protective Properties of Technical Sportswear Fabrics 100 Polyester Thethelazyllama444No ratings yet
- Skin Penetration and Sun Protection Factor of Five UV Filters - Effect of The VehicleDocument8 pagesSkin Penetration and Sun Protection Factor of Five UV Filters - Effect of The VehicleDavid Fernando Rojas BayonaNo ratings yet
- The Use of LED For Acne TreatmentDocument9 pagesThe Use of LED For Acne TreatmentDavid RahanraNo ratings yet
- Photoprotection in Changing times-UV Filter Efficacy and Safety, Sensitization Processes and Regulatory AspectsDocument29 pagesPhotoprotection in Changing times-UV Filter Efficacy and Safety, Sensitization Processes and Regulatory AspectsDavid Fernando Rojas BayonaNo ratings yet
- Sun Production Factor (SPF) Determination of Marketed Sunscreen Formulation by In-Vitro Method Using UV-VIS SpectrophotometerDocument4 pagesSun Production Factor (SPF) Determination of Marketed Sunscreen Formulation by In-Vitro Method Using UV-VIS SpectrophotometerArsiaty SumuleNo ratings yet
- Distribution of Sunscreens On SkinDocument7 pagesDistribution of Sunscreens On SkinDouglas DouradoNo ratings yet
- Ijpr 097501Document5 pagesIjpr 097501Neni Sri GunartiNo ratings yet
- Pi-Rard Et Al-2015-Journal of Cosmetic DermatologyDocument7 pagesPi-Rard Et Al-2015-Journal of Cosmetic DermatologyputrisarimelialaNo ratings yet
- Analisa Tingkat Paparan Radiasi Pesawat Sinar-XDocument5 pagesAnalisa Tingkat Paparan Radiasi Pesawat Sinar-XEva Lifstiani Al-fallasifahNo ratings yet
- Jcad 6 1 16 PDFDocument11 pagesJcad 6 1 16 PDFLPC AyiNo ratings yet
- FDA 1978 N 0018 0698 - Attachment - 65 PDFDocument46 pagesFDA 1978 N 0018 0698 - Attachment - 65 PDFDiva Ratna ShabrinaNo ratings yet
- Wistar UV Dan DMBADocument7 pagesWistar UV Dan DMBAdeyaNo ratings yet
- Liu 2020 IOP Conf. Ser. Earth Environ. Sci. 531 012034Document7 pagesLiu 2020 IOP Conf. Ser. Earth Environ. Sci. 531 012034letslearn procurementNo ratings yet
- Radiation Physics and Chemistry: S.F. Sabato, J.N. Cruz, P.R. Rela, P.O. BroislerDocument3 pagesRadiation Physics and Chemistry: S.F. Sabato, J.N. Cruz, P.R. Rela, P.O. Broisler891218No ratings yet
- BMC Dermatology: The Treatment of Melasma by Silymarin CreamDocument13 pagesBMC Dermatology: The Treatment of Melasma by Silymarin CreamAnna Listyana DewiNo ratings yet
- Ppe 3Document19 pagesPpe 3Sajin AlexanderNo ratings yet
- Dokumentasjon DimethiconeDocument6 pagesDokumentasjon DimethiconeJacqueline SunaryoNo ratings yet
- Research Capsule - UP StudentsDocument2 pagesResearch Capsule - UP StudentsKarra CasañaresNo ratings yet
- Clark 2015Document11 pagesClark 2015Nazera SalejeeNo ratings yet
- Alara PrincipleDocument4 pagesAlara PrincipleDevender KumarNo ratings yet
- Bagus 2Document10 pagesBagus 2Windra WartanaNo ratings yet
- Clays As Vehicles For Drug PhotostabilityDocument15 pagesClays As Vehicles For Drug PhotostabilityAdriana SampaioNo ratings yet
- Cohen2016 PDFDocument6 pagesCohen2016 PDFNati MalvehyNo ratings yet
- 13highway PDFDocument12 pages13highway PDFEl MarcelokoNo ratings yet
- PIIS0190962223010174Document7 pagesPIIS01909622230101745jnpzgz4cqNo ratings yet
- Ppe 10Document12 pagesPpe 10Sajin AlexanderNo ratings yet
- Mosaic TreatmentDocument5 pagesMosaic TreatmentMACPANAMERANo ratings yet
- Sophomore Research FinalDocument126 pagesSophomore Research Finalapi-397491176No ratings yet
- Vitamina CDocument8 pagesVitamina CCristina PastiuNo ratings yet
- Solarium Use and Risk For Malignant Melanoma Meta-Analysis and Evidence-Based Medicine Systematic Review BurgardDocument13 pagesSolarium Use and Risk For Malignant Melanoma Meta-Analysis and Evidence-Based Medicine Systematic Review BurgardSunbed-Association UK-IrelandNo ratings yet
- N95DECON UV Technicalreport v1.2 FinalDocument8 pagesN95DECON UV Technicalreport v1.2 FinalBrandonRojasNo ratings yet
- 3 Eye Irritation enDocument76 pages3 Eye Irritation enEvelyng Taype Espinoza100% (1)
- Radiation Protection in Nuclear MedicineFrom EverandRadiation Protection in Nuclear MedicineSören MattssonNo ratings yet
- S31 Wood S Light in DermatologyDocument8 pagesS31 Wood S Light in DermatologyGabriel CampolinaNo ratings yet
- S31 S77 Screening For Skin Cancer AIMDocument6 pagesS31 S77 Screening For Skin Cancer AIMGabriel CampolinaNo ratings yet
- U35 DipsticksDocument7 pagesU35 DipsticksGabriel CampolinaNo ratings yet
- P71 NEJM DeliriumDocument10 pagesP71 NEJM DeliriumGabriel CampolinaNo ratings yet
- P70 SIGN Dementia QuickReference GuideDocument2 pagesP70 SIGN Dementia QuickReference GuideGabriel CampolinaNo ratings yet
- P76 Depression AnnIntMed 2007Document16 pagesP76 Depression AnnIntMed 2007Gabriel CampolinaNo ratings yet
- P76 Men and DepressionDocument4 pagesP76 Men and DepressionGabriel CampolinaNo ratings yet
- S96 CKS Acne VulgarisDocument41 pagesS96 CKS Acne VulgarisGabriel CampolinaNo ratings yet
- Sinusitis - Acute Adults: PRODIGY Quick Reference GuideDocument4 pagesSinusitis - Acute Adults: PRODIGY Quick Reference GuideGabriel CampolinaNo ratings yet
- W19 BMJ Managing Common Breast Feeding Problems in The CommunityDocument9 pagesW19 BMJ Managing Common Breast Feeding Problems in The CommunityGabriel CampolinaNo ratings yet
- N01 Cefaleia - SIGNDocument88 pagesN01 Cefaleia - SIGNGabriel CampolinaNo ratings yet
- A44 CMAJ Reducing The Pain of Childhood VaccinationDocument7 pagesA44 CMAJ Reducing The Pain of Childhood VaccinationGabriel CampolinaNo ratings yet
- A06 NEJM Neurocardiogenic SyncopeDocument7 pagesA06 NEJM Neurocardiogenic SyncopeGabriel CampolinaNo ratings yet
- A01 Pain in The Cognitively Impaired ElderlyDocument9 pagesA01 Pain in The Cognitively Impaired ElderlyGabriel CampolinaNo ratings yet
- 4gauging GTXDocument1 page4gauging GTXZulfahmi NurdinNo ratings yet
- UM CML720 en 50119589Document197 pagesUM CML720 en 50119589Julian David Rocha OsorioNo ratings yet
- Web Application TORDocument3 pagesWeb Application TORFaxikko FazyNo ratings yet
- Digital Designer's Guide To Linear Voltage Regulators & Thermal Management - SLVA118 - 2003Document25 pagesDigital Designer's Guide To Linear Voltage Regulators & Thermal Management - SLVA118 - 2003Kevin PlayerNo ratings yet
- csc1201 Lecture13Document23 pagescsc1201 Lecture13Richard CoronelNo ratings yet
- Tomar - Industrial Signalling CatalogDocument82 pagesTomar - Industrial Signalling CatalogPrejit RadhakrishnaNo ratings yet
- Bomba Calpeda Cat - 60hz2004Document172 pagesBomba Calpeda Cat - 60hz2004brenossNo ratings yet
- How To Use Laravel 4 Filters: What Is A Filter?Document5 pagesHow To Use Laravel 4 Filters: What Is A Filter?bm2i89No ratings yet
- Simplification PDFDocument51 pagesSimplification PDFsubapacetNo ratings yet
- Ficha Tecnica Aquarius VeterinaryDocument1 pageFicha Tecnica Aquarius Veterinarydiana ruizNo ratings yet
- Multi V IV Indoor PDFDocument526 pagesMulti V IV Indoor PDFDavid AlbortNo ratings yet
- Skittles LabDocument4 pagesSkittles Labapi-363892860100% (1)
- Universal Transverse Mercator Coordinate System: History DefinitionsDocument8 pagesUniversal Transverse Mercator Coordinate System: History Definitionsanon_114803412No ratings yet
- ForecastingDocument2 pagesForecastingprashantNo ratings yet
- Simatic: STEP 7 Professional 2010 SR4 Engineering Software For SIMATIC S7 / M7 / C7Document16 pagesSimatic: STEP 7 Professional 2010 SR4 Engineering Software For SIMATIC S7 / M7 / C7Noureddine ElaatmaniNo ratings yet
- How To Manage Inbound Outbound Route On UCMDocument23 pagesHow To Manage Inbound Outbound Route On UCMEmilio I WildeNo ratings yet
- Curriculum Master Computational Science 2021-2022Document1 pageCurriculum Master Computational Science 2021-2022Kiran MenonNo ratings yet
- Chapter 2 THE NATURE OF SCIENCEDocument17 pagesChapter 2 THE NATURE OF SCIENCENur-aine HajijulNo ratings yet
- A Brief Overview of The Regime Shift Detection Methods: Sergei RodionovDocument28 pagesA Brief Overview of The Regime Shift Detection Methods: Sergei RodionovDaniela MerchanNo ratings yet
- Treynor Black ModelDocument20 pagesTreynor Black ModelVaidyanathan RavichandranNo ratings yet
- Parker - CYL - Cross RefDocument15 pagesParker - CYL - Cross RefAlaa saidNo ratings yet
- Zipf 1945 The Meaning-Frequency Relationship of WordsDocument8 pagesZipf 1945 The Meaning-Frequency Relationship of WordsIker SalaberriNo ratings yet
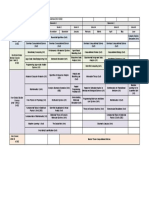
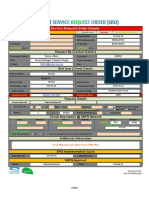
- Service Request Order DetailsDocument4 pagesService Request Order DetailsKashif NaeemNo ratings yet