You might also like
- Manual Emdr Parts Work Treating Complex TraumaDocument73 pagesManual Emdr Parts Work Treating Complex Traumacora4eva5699100% (1)
- Dissociative DisorderDocument44 pagesDissociative DisorderKiaraMaeRhiasNo ratings yet
- Understanding PTSDDocument22 pagesUnderstanding PTSDLucy FoskettNo ratings yet
- PTSD Diagnosis & AssessmentDocument2 pagesPTSD Diagnosis & AssessmentAlesha Rose100% (6)
- PTSD PaperDocument7 pagesPTSD PaperBeccaShanksNo ratings yet
- PTSD TreatmentDocument2 pagesPTSD TreatmentAlesha Rose100% (1)
- DSM Diagnosis of Conduct DisorderDocument12 pagesDSM Diagnosis of Conduct DisorderponchossNo ratings yet
- PTSD and Cognitive Processing Therapy Presented by Patricia A. Resick, PHD, AbppDocument28 pagesPTSD and Cognitive Processing Therapy Presented by Patricia A. Resick, PHD, AbppDardo Arreche100% (2)
- Psychotherapy in PTSDDocument14 pagesPsychotherapy in PTSDraquka06100% (2)
- PTSD Research PaperDocument11 pagesPTSD Research Paperapi-548851649No ratings yet
- Trauma and Stressor-Related DisordersDocument58 pagesTrauma and Stressor-Related DisordersHamid Colangcag AmborNo ratings yet
- Ask and RecieveDocument60 pagesAsk and RecieveScribdnera100% (1)
- Post Traumatic Stress Disorder PowerpointDocument18 pagesPost Traumatic Stress Disorder Powerpointapi-505733770100% (3)
- Pat Ogden Sensorimotor Therapy PDFDocument16 pagesPat Ogden Sensorimotor Therapy PDFEmili Giralt GuarroNo ratings yet
- Amistoso - DMDDDocument25 pagesAmistoso - DMDDAndréAmistosoNo ratings yet
- Behavioral Problems EncounteredDocument35 pagesBehavioral Problems EncounteredNamoAmitofou100% (1)
- Practice Essentials: Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)Document20 pagesPractice Essentials: Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)Anonymous 2ernTkNo ratings yet
- Post-Traumatic Stress Disorder (PTSD) PDFDocument13 pagesPost-Traumatic Stress Disorder (PTSD) PDFSheza SiddiquiNo ratings yet
- 2018.02.08 Trauma and Stressor Related DisordersDocument38 pages2018.02.08 Trauma and Stressor Related DisordersErin RyanNo ratings yet
- The Uk College of Hypnosis Hypnotherapy PDFDocument23 pagesThe Uk College of Hypnosis Hypnotherapy PDFblu6660% (1)
- The Evolution of Morality - Todd K. Shackelford y Ranald D. HansenDocument327 pagesThe Evolution of Morality - Todd K. Shackelford y Ranald D. HansenSam De León100% (1)
- The Art of EMDR Therapy in PTSD and Trauma: A Practical HandbookFrom EverandThe Art of EMDR Therapy in PTSD and Trauma: A Practical HandbookNo ratings yet
- Emotion Perception in MusicDocument5 pagesEmotion Perception in Musicnefeli123No ratings yet
- Prescribing Antipsychotics in Geriatric Patients:: First of 3 PartsDocument8 pagesPrescribing Antipsychotics in Geriatric Patients:: First of 3 PartsAlexRázuri100% (1)
- PTSD Takes Over The BrainDocument3 pagesPTSD Takes Over The Brainapi-548851649No ratings yet
- Trauma - and Stressor-Related DisordersDocument39 pagesTrauma - and Stressor-Related Disordersraneemghandour28No ratings yet
- Psych AdjustmentDocument2 pagesPsych Adjustmentapi-3704562No ratings yet
- Post-Traumatic Stress Disorder and Acute Stress DisorderDocument3 pagesPost-Traumatic Stress Disorder and Acute Stress Disorderag.carismaaNo ratings yet
- Ies RDocument2 pagesIes RJohn PrestonNo ratings yet
- Adjustment DisordersDocument2 pagesAdjustment DisordersIsabel CastilloNo ratings yet
- PTSDDocument4 pagesPTSDAzim Arif HashmiNo ratings yet
- Stress and Related DsDocument49 pagesStress and Related DsRibhav GuptaNo ratings yet
- Depression in Children and Young People: Symposium: PsychiatryDocument8 pagesDepression in Children and Young People: Symposium: Psychiatry126 - Askandarnur riskisa PahleviNo ratings yet
- PTSD EssayDocument7 pagesPTSD Essayaqsa rehmanNo ratings yet
- Abnormal Psychology (Chapter 5)Document3 pagesAbnormal Psychology (Chapter 5)Mavy QueenNo ratings yet
- DepressionDocument2 pagesDepressionIQRA ZAINABNo ratings yet
- Leaflet JiwaDocument3 pagesLeaflet JiwabilaNo ratings yet
- PTSDDocument3 pagesPTSDdaryaNo ratings yet
- Abpsych Midterms NotesDocument8 pagesAbpsych Midterms NotesJoshua MendezNo ratings yet
- Module 5a - Stress, Health, and Coping: Selye's Concept of StressDocument2 pagesModule 5a - Stress, Health, and Coping: Selye's Concept of Stress5676758457No ratings yet
- Perinatal Depression Review 20Document5 pagesPerinatal Depression Review 20Paula SouzaNo ratings yet
- Psych 410 PTSD NotesDocument4 pagesPsych 410 PTSD Notesapi-736917344No ratings yet
- Psychiatry - Mood Life and DeathDocument2 pagesPsychiatry - Mood Life and Deathhaladaqqa1No ratings yet
- Mental Health AwarenessDocument8 pagesMental Health AwarenessOyvin SemillaNo ratings yet
- Understanding and Dealing With ViolenceDocument58 pagesUnderstanding and Dealing With ViolenceIrene Grace FernandezNo ratings yet
- BCMJ 49 Vol3 Articles Posttraumatic StressDocument6 pagesBCMJ 49 Vol3 Articles Posttraumatic StressFrancisca AldunateNo ratings yet
- PTSD AwarenessDocument2 pagesPTSD AwarenessAdyson MorrisNo ratings yet
- PTSD-reading 2Document11 pagesPTSD-reading 2Az Z IrcNo ratings yet
- 4 - StressDocument60 pages4 - StressAman Singh RaoNo ratings yet
- Megan Simpson SBCNA 2018Document7 pagesMegan Simpson SBCNA 2018Priya JadhavNo ratings yet
- P.E. Group 3 PTSDDocument17 pagesP.E. Group 3 PTSDDavid Aldrich LimNo ratings yet
- DialoguesClinNeurosci 21 417Document12 pagesDialoguesClinNeurosci 21 417VickeyNo ratings yet
- Prof - Ed Task10Document2 pagesProf - Ed Task10Xyriz Seline SecillanoNo ratings yet
- Chapter 2 Trauma and Trauma ReactionsDocument42 pagesChapter 2 Trauma and Trauma ReactionsAnton BalansagNo ratings yet
- Chapter 9Document11 pagesChapter 9nayaddouaihyNo ratings yet
- Clinical Significance of A Proposed Developmental Trauma Disorder Diagnosis - Results of An International Survey of Clinicians - 2020 11 09 232956Document14 pagesClinical Significance of A Proposed Developmental Trauma Disorder Diagnosis - Results of An International Survey of Clinicians - 2020 11 09 232956abelim01No ratings yet
- Perinatal Depression: A ReviewDocument5 pagesPerinatal Depression: A ReviewDewi NofiantiNo ratings yet
- Trauma and Related DisorderDocument127 pagesTrauma and Related DisorderMayla WahabNo ratings yet
- Psychological Therapies For Posttraumatic Stress Disorder PDFDocument5 pagesPsychological Therapies For Posttraumatic Stress Disorder PDFJessicaPudduNo ratings yet
- Acute Stress DisorderDocument13 pagesAcute Stress DisorderYaska MusaNo ratings yet
- TRAUMADocument18 pagesTRAUMAcameronjuli.patubo.sciNo ratings yet
- Trauma Concept PaperDocument7 pagesTrauma Concept Paperapi-226804663No ratings yet
- What Is Trauma?Document10 pagesWhat Is Trauma?gayle livelo100% (1)
- Jane - Narrative PresentationDocument75 pagesJane - Narrative PresentationKathy ProcykNo ratings yet
- James Morrison Chapter 6 and 7 JMDocument7 pagesJames Morrison Chapter 6 and 7 JMAmanda ParrellaNo ratings yet
- Lesión Cerebral TraumáticaDocument8 pagesLesión Cerebral TraumáticaAlexRázuriNo ratings yet
- Correspondence: Atypical Presentation of COVID-19 in Young InfantsDocument1 pageCorrespondence: Atypical Presentation of COVID-19 in Young InfantsAlexRázuriNo ratings yet
- Trastornos PsicóticosDocument5 pagesTrastornos PsicóticosAlexRázuriNo ratings yet
- BMJ inflammatorySD ChildrenDocument1 pageBMJ inflammatorySD ChildrenAlexRázuriNo ratings yet
- EEG Epilepsia y Sueño 2Document12 pagesEEG Epilepsia y Sueño 2AlexRázuriNo ratings yet
- UK - BTS - Respiratory Support of Patients On Medical WardsDocument5 pagesUK - BTS - Respiratory Support of Patients On Medical WardsAlexRázuriNo ratings yet
- UK - Rapid Guideline Critical Care in AdultsDocument13 pagesUK - Rapid Guideline Critical Care in AdultsAlexRázuriNo ratings yet
- Article Covid-19 Children ReviewDocument12 pagesArticle Covid-19 Children ReviewAlexRázuri100% (1)
- Consensus Guidelines For Managing The Airway in Children With COVID-19Document11 pagesConsensus Guidelines For Managing The Airway in Children With COVID-19AlexRázuriNo ratings yet
- Remember:: Before Caring For Patients With Confirmed or Suspected COVID-19, Healthcare Personnel (HCP) MustDocument1 pageRemember:: Before Caring For Patients With Confirmed or Suspected COVID-19, Healthcare Personnel (HCP) MustAlexRázuriNo ratings yet
- Uptodate - Covid Guidelines LinksDocument10 pagesUptodate - Covid Guidelines LinksAlexRázuriNo ratings yet
- Article Origin Transmission Characterist COVID PDFDocument8 pagesArticle Origin Transmission Characterist COVID PDFAlexRázuriNo ratings yet
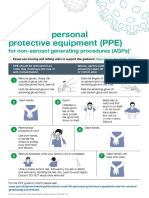
- Taking Off Personal Protective Equipment (Ppe) : For Non-Aerosol Generating Procedures (Agps)Document1 pageTaking Off Personal Protective Equipment (Ppe) : For Non-Aerosol Generating Procedures (Agps)AlexRázuriNo ratings yet
- T2 Poster Recommended PPE For Primary Outpatient Community and Social Care by SettingDocument1 pageT2 Poster Recommended PPE For Primary Outpatient Community and Social Care by SettingAlexRázuriNo ratings yet
- Uptodate - Coronavirus Epi, PreventionDocument55 pagesUptodate - Coronavirus Epi, PreventionAlexRázuriNo ratings yet
- Article Epidemio Therapeutics Vaccines Covid PDFDocument12 pagesArticle Epidemio Therapeutics Vaccines Covid PDFAlexRázuriNo ratings yet
- Epidemiology and Clinical Characteristics of COVID-19: MedicineDocument4 pagesEpidemiology and Clinical Characteristics of COVID-19: MedicineAlexRázuriNo ratings yet
- 1er ArticuloDocument7 pages1er ArticuloAlexRázuriNo ratings yet
- Betty Neuman Systems TheoryDocument6 pagesBetty Neuman Systems TheoryJenny SorianoNo ratings yet
- The Evaluation of Minecraft SampsonDocument7 pagesThe Evaluation of Minecraft Sampsonapi-279981311No ratings yet
- Barrett D 1992 Through A Glass Darkly Images of The Dead in DreamsDocument12 pagesBarrett D 1992 Through A Glass Darkly Images of The Dead in DreamsJuan ArizaNo ratings yet
- Grade 1 RHGP Module 2023Document59 pagesGrade 1 RHGP Module 2023JEANNo ratings yet
- Homework Marriage SolDocument4 pagesHomework Marriage Soltranthanhhoa2468No ratings yet
- Financial and Non-Financial Incentives - Explained!: by DR - Khalid RashidDocument47 pagesFinancial and Non-Financial Incentives - Explained!: by DR - Khalid RashidAshrafAliNo ratings yet
- Introduction To The Course: Midterm/Final GradeDocument9 pagesIntroduction To The Course: Midterm/Final GradeRanniel EstrellaNo ratings yet
- Action Research Presentation Berf 4.0Document21 pagesAction Research Presentation Berf 4.0Ricardo Evalla Jueves Jr.No ratings yet
- Adult DisordersDocument2 pagesAdult DisordersKai PesquiraNo ratings yet
- Writing Assignment Week TwoDocument3 pagesWriting Assignment Week TwoyesihavenNo ratings yet
- Introduction To Cross Culture and Human Resource ManagementDocument9 pagesIntroduction To Cross Culture and Human Resource ManagementRachel CoutinhoNo ratings yet
- Leadership Questions PDFDocument10 pagesLeadership Questions PDFdeanNo ratings yet
- Chapter 1 To 5Document72 pagesChapter 1 To 5Genesis AngeloNo ratings yet
- Lesson 10 - What - S Your PersonalityDocument21 pagesLesson 10 - What - S Your PersonalityLOVELY DELA CERNA50% (2)
- Teacher Stress Final Pre-Publication DraftDocument18 pagesTeacher Stress Final Pre-Publication DraftRegine CuntapayNo ratings yet
- Socio-Political Realities in Relation To Contemporary World.Document3 pagesSocio-Political Realities in Relation To Contemporary World.emmanuel.egoniaNo ratings yet
- FULLRESEARCHWORKONSTRESS EmmaDocument81 pagesFULLRESEARCHWORKONSTRESS EmmaCarmina BesarioNo ratings yet
- Robert Mager CRIDocument7 pagesRobert Mager CRInelieltuodeshvank50% (2)
- Lesh&harel BigfootDocument33 pagesLesh&harel BigfootAyşe YolcuNo ratings yet
- Group2 Lesson4 ReportDocument15 pagesGroup2 Lesson4 ReportJann Marie CalledoNo ratings yet
- NURS FPX 6105 Assessment 1 Learning Theories and DiversityDocument6 pagesNURS FPX 6105 Assessment 1 Learning Theories and Diversityzadem5266No ratings yet
- Organizational Behavior 4th Edition Hitt Test BankDocument19 pagesOrganizational Behavior 4th Edition Hitt Test BankSaraSmithdgyj100% (40)
- Alex A. Courtney-Guy-Data Blitz PresentationDocument10 pagesAlex A. Courtney-Guy-Data Blitz PresentationEvie EmeryNo ratings yet
- Practical Nursing Clinical Syllabus-2014-15Document110 pagesPractical Nursing Clinical Syllabus-2014-15jedisay1No ratings yet