You might also like
- FasdfyDocument8 pagesFasdfyzuliamNo ratings yet
- Airway Mana1231dasdsDocument34 pagesAirway Mana1231dasdszuliamNo ratings yet
- A Framework For The Management of The Pediatric AirwayDocument23 pagesA Framework For The Management of The Pediatric AirwayDaniel GallegoNo ratings yet
- Journal Update For Total Intravenous AnsthesiaDocument11 pagesJournal Update For Total Intravenous AnsthesiaalinNo ratings yet
- Guidelines For The Management of Tracheal Intubation in Critically Ill AdultsDocument26 pagesGuidelines For The Management of Tracheal Intubation in Critically Ill AdultsFemiko Panji AprilioNo ratings yet
- COVID 19 - Guidance For Paediatric ServicesDocument16 pagesCOVID 19 - Guidance For Paediatric ServicesKomite Medik RSUD BangilNo ratings yet
- Nutrition Therapy COVID 19 SCCM ASPENDocument8 pagesNutrition Therapy COVID 19 SCCM ASPENtomtranNo ratings yet
- Guidance For Return To Practice For Otolaryngology-Head and Neck SurgeryDocument9 pagesGuidance For Return To Practice For Otolaryngology-Head and Neck SurgeryLeslie Lindsay AlvarezNo ratings yet
- Emergency Endotracheal Intubation in Children - UpToDateDocument63 pagesEmergency Endotracheal Intubation in Children - UpToDatedr_comNo ratings yet
- Respiratory Distress in ChildrenDocument16 pagesRespiratory Distress in ChildrenNanda WibowoNo ratings yet
- Consenso de Sindroe de Dificultad Respiratoria en NeonataosDocument19 pagesConsenso de Sindroe de Dificultad Respiratoria en NeonataosSayonara Mordagon ChoqueticllaNo ratings yet
- Pneumonia in Children - Inpatient Treatment - UpToDateDocument48 pagesPneumonia in Children - Inpatient Treatment - UpToDatejess.khoo.1204No ratings yet
- Guidiline SdraDocument19 pagesGuidiline SdraLariza CostaNo ratings yet
- Covid y TraqueostomíaDocument9 pagesCovid y TraqueostomíaCatalina Muñoz VelasquezNo ratings yet
- Recommendations For Prehospital Airway Management in Patients With Suspected COVID-19 InfectionDocument5 pagesRecommendations For Prehospital Airway Management in Patients With Suspected COVID-19 InfectionConnor StephensonNo ratings yet
- Sop Number Title of SOP Author Consultation With StakeholdersDocument23 pagesSop Number Title of SOP Author Consultation With StakeholdersMr. BamsNo ratings yet
- Children's Respiratory NursingFrom EverandChildren's Respiratory NursingJanice MightenNo ratings yet
- COVID-19 - Guidance For Paediatric Services: Last ModifiedDocument26 pagesCOVID-19 - Guidance For Paediatric Services: Last ModifiedIrfan Ullah KhanNo ratings yet
- Bronchiolitis in Children Bronchiolitis in Children: NICE Guideline Published: 1 June 2015Document30 pagesBronchiolitis in Children Bronchiolitis in Children: NICE Guideline Published: 1 June 2015Jan QuinteroNo ratings yet
- Chemicalagentsindisaster: Care and Management in The Intensive Care UnitDocument13 pagesChemicalagentsindisaster: Care and Management in The Intensive Care Unitgarinda almadutaNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal Resuscitationrubie ann tillorNo ratings yet
- Pediatric Rapid Sequence Intubation - An In-Depth ReviewDocument12 pagesPediatric Rapid Sequence Intubation - An In-Depth ReviewDiego LatorreNo ratings yet
- COVID 19. 4 - 13 KashmerDocument42 pagesCOVID 19. 4 - 13 KashmerIshfaq GanaiNo ratings yet
- Resusitasi Neonatus 2020 AAPDocument30 pagesResusitasi Neonatus 2020 AAPWafiq AzizahNo ratings yet
- Ped Asthma Journal 2019Document11 pagesPed Asthma Journal 2019Straits MasterNo ratings yet
- Paediatric Basic Life Support GuidelinesDocument19 pagesPaediatric Basic Life Support GuidelinesstevaniNo ratings yet
- Clinical Practice Guideline: Perinatal-Neonatal Management of COVID-19Document6 pagesClinical Practice Guideline: Perinatal-Neonatal Management of COVID-19Sughosh MitraNo ratings yet
- Refeeding Syndome GuidelineDocument31 pagesRefeeding Syndome GuidelineFidya ArdinyNo ratings yet
- Bronchiolitis in Children: Scottish Intercollegiate Guidelines NetworkDocument46 pagesBronchiolitis in Children: Scottish Intercollegiate Guidelines NetworkAnonymous 6iwMFwNo ratings yet
- 399 ImagesDocument11 pages399 ImageskhalidNo ratings yet
- Paediatric Basic Life Support GuidelinesDocument19 pagesPaediatric Basic Life Support GuidelinesDellaneira SetjiadiNo ratings yet
- Pneumonia in Children - Inpatient Treatment - UpToDateDocument23 pagesPneumonia in Children - Inpatient Treatment - UpToDateJunny Yeliitza Wilches GualdronNo ratings yet
- Journal NicuDocument4 pagesJournal NicuMargaret LlavorNo ratings yet
- Suction SOP 2018Document13 pagesSuction SOP 2018ika lestariNo ratings yet
- Handbook of Patient Safety 2022Document370 pagesHandbook of Patient Safety 2022Agus SalimNo ratings yet
- 2011 Chapter 6 Protocol PEDIATRIEDocument42 pages2011 Chapter 6 Protocol PEDIATRIESbarcea AurelNo ratings yet
- 2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisDocument22 pages2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisAuliaRahmanNo ratings yet
- Baby Sleep Incidental Aspiration Case ReportDocument4 pagesBaby Sleep Incidental Aspiration Case ReportSebastian Jaén Vinueza SoteloNo ratings yet
- Rapid Training of Healthcare Staff For Protected Cardiopulmonary Resuscitation in The COVID-19 PandemicDocument3 pagesRapid Training of Healthcare Staff For Protected Cardiopulmonary Resuscitation in The COVID-19 PandemicRicardo BarreraNo ratings yet
- Anaesthesia and Perioperative Care: Mark Newton Stella A. Eguma Olamide O. DairoDocument6 pagesAnaesthesia and Perioperative Care: Mark Newton Stella A. Eguma Olamide O. DairoNana Virtuoso EsselNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationMarcela ZerilloNo ratings yet
- CPG Management of Childhood Asthma (2014)Document20 pagesCPG Management of Childhood Asthma (2014)Haz100% (1)
- Adult NebuliserDocument13 pagesAdult NebuliserBeh Boon CongNo ratings yet
- Management of Multiple PregnancyDocument14 pagesManagement of Multiple PregnancyxxdrivexxNo ratings yet
- Specialconsiderationsin Neonatalmechanical Ventilation: Stacey Dalgleish,, Linda Kostecky,, Irina CharaniaDocument22 pagesSpecialconsiderationsin Neonatalmechanical Ventilation: Stacey Dalgleish,, Linda Kostecky,, Irina CharaniaGuisela Carbajal RomeroNo ratings yet
- Artigo 3Document11 pagesArtigo 3Luísa KarolinaNo ratings yet
- Advances in Emergent Airway Management in PediatricsDocument19 pagesAdvances in Emergent Airway Management in PediatricsLuis Miguel VillanuevaNo ratings yet
- PSSJN - Volume 1 - Issue 2 - Pages 265-280Document16 pagesPSSJN - Volume 1 - Issue 2 - Pages 265-280Praveen YadavNo ratings yet
- 1.e. Bronchiolitis Treatment & Management - Approach Considerations, Initial Management, Admission CriteriaDocument12 pages1.e. Bronchiolitis Treatment & Management - Approach Considerations, Initial Management, Admission CriteriaDavid CraigNo ratings yet
- Algorithm For Difficult Airway Management in PediatricsDocument13 pagesAlgorithm For Difficult Airway Management in PediatricsWandi MuhammadNo ratings yet
- JPEN 9999 NaDocument28 pagesJPEN 9999 NaedithNo ratings yet
- 02a - PPE - Summary and Rationale For RecommendationsDocument2 pages02a - PPE - Summary and Rationale For RecommendationsMohammedNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationAngela Giselle Garcia RuizNo ratings yet
- RCP NeonatalDocument42 pagesRCP NeonatalWinny CastroNo ratings yet
- Neoreviews 2013 Keszler E237 51Document17 pagesNeoreviews 2013 Keszler E237 51Gun HawkNo ratings yet
- NAC en NiñosDocument14 pagesNAC en NiñosAnonymous DxJyWJwtNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationFandoko ChaniagoNo ratings yet
- Resuscitation: European Resuscitation Council Guidelines 2021: Paediatric Life SupportDocument61 pagesResuscitation: European Resuscitation Council Guidelines 2021: Paediatric Life SupportditarusdianaNo ratings yet
- Rapid Sequence Intubation (RSI) Outside The Operating Room in Children - Approach - UpToDateDocument29 pagesRapid Sequence Intubation (RSI) Outside The Operating Room in Children - Approach - UpToDatedr_comNo ratings yet
- Lesión Cerebral TraumáticaDocument8 pagesLesión Cerebral TraumáticaAlexRázuriNo ratings yet
- Deterioro Neurocognitivo en Desorde BipolarDocument11 pagesDeterioro Neurocognitivo en Desorde BipolarAlexRázuriNo ratings yet
- s41380 021 01021 4Document14 pagess41380 021 01021 4Juan M SagnirbNo ratings yet
- COVID-19 Long Term EffectsDocument22 pagesCOVID-19 Long Term EffectsMcKenzie Stauffer100% (10)
- s41380 021 01021 4Document14 pagess41380 021 01021 4Juan M SagnirbNo ratings yet
- Trastornos PsicóticosDocument5 pagesTrastornos PsicóticosAlexRázuriNo ratings yet
- Estrés, Trauma y Trastornos RelacionadosDocument6 pagesEstrés, Trauma y Trastornos RelacionadosAlexRázuriNo ratings yet
- EEG Epilepsia y Sueño 2Document12 pagesEEG Epilepsia y Sueño 2AlexRázuriNo ratings yet
- BMJ inflammatorySD ChildrenDocument1 pageBMJ inflammatorySD ChildrenAlexRázuriNo ratings yet
- Correspondence: Atypical Presentation of COVID-19 in Young InfantsDocument1 pageCorrespondence: Atypical Presentation of COVID-19 in Young InfantsAlexRázuriNo ratings yet
- Declaration of ConformityDocument1 pageDeclaration of ConformityTiago GomesNo ratings yet
- Remember:: Before Caring For Patients With Confirmed or Suspected COVID-19, Healthcare Personnel (HCP) MustDocument1 pageRemember:: Before Caring For Patients With Confirmed or Suspected COVID-19, Healthcare Personnel (HCP) MustAlexRázuriNo ratings yet
- Article Covid-19 Children ReviewDocument12 pagesArticle Covid-19 Children ReviewAlexRázuri100% (1)
- Uptodate - Covid Critical PDFDocument49 pagesUptodate - Covid Critical PDFAlexRázuriNo ratings yet
- Consensus Guidelines For Managing The Airway in Children With COVID-19Document11 pagesConsensus Guidelines For Managing The Airway in Children With COVID-19AlexRázuriNo ratings yet
- UK - Rapid Guideline Critical Care in AdultsDocument13 pagesUK - Rapid Guideline Critical Care in AdultsAlexRázuriNo ratings yet
- Recommended PPE For Healthcare Workers by Secondary Care Inpatient Clinical Setting, NHS and Independent SectorDocument1 pageRecommended PPE For Healthcare Workers by Secondary Care Inpatient Clinical Setting, NHS and Independent Sectorumerjaved86No ratings yet
- T2 Poster Recommended PPE For Primary Outpatient Community and Social Care by SettingDocument1 pageT2 Poster Recommended PPE For Primary Outpatient Community and Social Care by SettingAlexRázuriNo ratings yet
- Uptodate - Coronavirus Epi, PreventionDocument55 pagesUptodate - Coronavirus Epi, PreventionAlexRázuriNo ratings yet
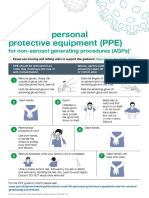
- Taking Off Personal Protective Equipment (Ppe) : For Non-Aerosol Generating Procedures (Agps)Document1 pageTaking Off Personal Protective Equipment (Ppe) : For Non-Aerosol Generating Procedures (Agps)AlexRázuriNo ratings yet
- UK - BTS - Respiratory Support of Patients On Medical WardsDocument5 pagesUK - BTS - Respiratory Support of Patients On Medical WardsAlexRázuriNo ratings yet
- Considerations For Acute Personal Protective Equipment (PPE) Shortages - GOV - UKDocument7 pagesConsiderations For Acute Personal Protective Equipment (PPE) Shortages - GOV - UKAlexRázuriNo ratings yet
- Article Epidemio Therapeutics Vaccines Covid PDFDocument12 pagesArticle Epidemio Therapeutics Vaccines Covid PDFAlexRázuriNo ratings yet
- Adjusting in Public Health PDFDocument4 pagesAdjusting in Public Health PDFShams LadakNo ratings yet
- Coronavirus Disease 2019 (COVID-19) : The Right Clinical Information, Right Where It's NeededDocument128 pagesCoronavirus Disease 2019 (COVID-19) : The Right Clinical Information, Right Where It's NeededpedroNo ratings yet
- OUP Lockdowns Through World CovidDocument1 pageOUP Lockdowns Through World CovidAlexRázuriNo ratings yet
- Article Origin Transmission Characterist COVID PDFDocument8 pagesArticle Origin Transmission Characterist COVID PDFAlexRázuriNo ratings yet
- Novel Coronavirus Disease (COVID-19) : A Pandemic (Epidemiology, Pathogenesis and Potential Therapeutics)Document10 pagesNovel Coronavirus Disease (COVID-19) : A Pandemic (Epidemiology, Pathogenesis and Potential Therapeutics)sameer sahaanNo ratings yet
- UK - Transmission and Prevention and ControlDocument4 pagesUK - Transmission and Prevention and ControlAlexRázuriNo ratings yet
- Clippers and ClampersDocument8 pagesClippers and Clamperspuneeth kumarNo ratings yet
- Vo 1263 AaDocument8 pagesVo 1263 Aa801400No ratings yet
- Dangote Fertilizer Project NDT Analysis For U/G: Radiographic Test - Ultrasonic TestDocument6 pagesDangote Fertilizer Project NDT Analysis For U/G: Radiographic Test - Ultrasonic Testaakash100% (1)
- Recruiting Test General KnowledgeDocument15 pagesRecruiting Test General KnowledgeRelando Bailey84% (174)
- Asus Prime b250m Plus RGDocument13 pagesAsus Prime b250m Plus RGRenattech SilvaNo ratings yet
- The ID.4 New Model Overview: Self Study Program 891213Document50 pagesThe ID.4 New Model Overview: Self Study Program 891213António FernandesNo ratings yet
- Dyneema Vs SteelDocument5 pagesDyneema Vs SteelSaurabh KumarNo ratings yet
- Okuma GENOS M560R-V TECHNICAL SHEET (4th Edition)Document79 pagesOkuma GENOS M560R-V TECHNICAL SHEET (4th Edition)Ferenc Ungvári100% (1)
- Galleria MellonellaDocument6 pagesGalleria MellonellaJustin GarciaNo ratings yet
- Health & Performance Monitoring Using Active Magnetic BearingsDocument104 pagesHealth & Performance Monitoring Using Active Magnetic BearingsAbhinav RajNo ratings yet
- Ma2 - Acca - Chapter 1Document24 pagesMa2 - Acca - Chapter 1leducNo ratings yet
- Carte Tehnica Panou Fotovoltaic Cu Celule Policristaline Eging 250 WDocument1 pageCarte Tehnica Panou Fotovoltaic Cu Celule Policristaline Eging 250 WConstantin CilibiuNo ratings yet
- GDPDocument6 pagesGDPBenedetta NardiNo ratings yet
- Differential Release of Mast Cell Mediators and The Pathogenesis of InflammationDocument14 pagesDifferential Release of Mast Cell Mediators and The Pathogenesis of InflammationklaumrdNo ratings yet
- Essay Test 2021 (Practice Test)Document3 pagesEssay Test 2021 (Practice Test)Philani HadebeNo ratings yet
- Class 10 Syllabus Breakup ChemistryDocument4 pagesClass 10 Syllabus Breakup ChemistryUmme AbdullahNo ratings yet
- Srotomaya Shariram: Dr. Prasanna N. Rao Principal, SDM College of Ayurveda, Hassan-KaranatakaDocument21 pagesSrotomaya Shariram: Dr. Prasanna N. Rao Principal, SDM College of Ayurveda, Hassan-KaranatakaDrHemant ToshikhaneNo ratings yet
- A Framework For Developing and Evaluating Utility Substation Cyber Security - Schneider ElectricDocument10 pagesA Framework For Developing and Evaluating Utility Substation Cyber Security - Schneider ElectricHugh cabNo ratings yet
- Lab 6 - Wide Flange BeamDocument4 pagesLab 6 - Wide Flange BeamJanithNo ratings yet
- Fluke Acess TemperatureDocument4 pagesFluke Acess TemperatureJuan José Villavicencio CantoNo ratings yet
- Well Control Daily Checklist Procedure VDocument13 pagesWell Control Daily Checklist Procedure VmuratNo ratings yet
- Examination, June/July: ExplainDocument6 pagesExamination, June/July: ExplainSandesh KulalNo ratings yet
- Solving Poisson's Equation Using The FFTDocument9 pagesSolving Poisson's Equation Using The FFTJhon CerónNo ratings yet
- LogDocument8 pagesLogMaria SuyantiNo ratings yet
- Spare Parts Quotation For Scba & Eebd - 2021.03.19Document14 pagesSpare Parts Quotation For Scba & Eebd - 2021.03.19byhf2jgqprNo ratings yet
- Tank Vessel Overflow Line SizingDocument4 pagesTank Vessel Overflow Line SizingSteve Wan100% (1)
- OOO The Word Center: Love Is Our HeadquartersDocument39 pagesOOO The Word Center: Love Is Our HeadquartersNkor IokaNo ratings yet
- BP503T Unit 1-3Document432 pagesBP503T Unit 1-3Solomon GyampohNo ratings yet
- An Open Letter To Annie Besant PDFDocument2 pagesAn Open Letter To Annie Besant PDFdeniseNo ratings yet
- EMI Unit 1Document98 pagesEMI Unit 1Anirudhh RaviNo ratings yet