You might also like
- DR Write UpDocument15 pagesDR Write Upjansestacio100% (3)
- Root Operations in The Medical and Surgical Section (ICD-10)Document2 pagesRoot Operations in The Medical and Surgical Section (ICD-10)Nicholas Henry100% (1)
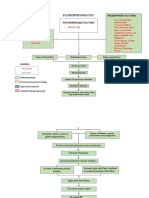
- Pathophysiology of Pulmonary Embolism (Loria.J)Document2 pagesPathophysiology of Pulmonary Embolism (Loria.J)Justine Mae Loria0% (1)
- Technical Report Cereform ImplantsDocument44 pagesTechnical Report Cereform Implantsrik4100No ratings yet
- JessDocument20 pagesJessdeepaliarneja67% (3)
- Palpable Lumps After MastectomyDocument23 pagesPalpable Lumps After MastectomyMinh Thư DươngNo ratings yet
- Normal Findings and Complications of Breast Implants.: Poster No.: Congress: Type: AuthorsDocument35 pagesNormal Findings and Complications of Breast Implants.: Poster No.: Congress: Type: AuthorsYasminSolbergNo ratings yet
- Breast 8Document5 pagesBreast 8giant nitaNo ratings yet
- Appropriate Use of Magnetic Resonance Imaging and Ultrasound To Detect Early Silicone Gel Breast Implant Rupture in Postmastectomy ReconstructionDocument8 pagesAppropriate Use of Magnetic Resonance Imaging and Ultrasound To Detect Early Silicone Gel Breast Implant Rupture in Postmastectomy ReconstructionJuan Daniel NaranjoNo ratings yet
- Nihms 233903 PDFDocument92 pagesNihms 233903 PDFGonzalo ZieglerNo ratings yet
- Primary Fibrosarcoma of Breast: A Rare Case Presentation: Cash ReportDocument4 pagesPrimary Fibrosarcoma of Breast: A Rare Case Presentation: Cash ReportBastiaanNo ratings yet
- Mammography and Breast Localization For The InterventionalistDocument6 pagesMammography and Breast Localization For The InterventionalistrasminojNo ratings yet
- Silicon Induced LymphoafenopathyDocument5 pagesSilicon Induced LymphoafenopathyDiana RomanovaNo ratings yet
- Imaging in The Post-Partum Period: Clinical Challenges, Normal Findings, and Common Imaging PitfallsDocument13 pagesImaging in The Post-Partum Period: Clinical Challenges, Normal Findings, and Common Imaging PitfallsBesse Darmita Yuana PutriNo ratings yet
- PIIS1089251613000930Document9 pagesPIIS1089251613000930rasminojNo ratings yet
- 1 s2.0 S1110036217300481 MainDocument3 pages1 s2.0 S1110036217300481 MainPutri YingNo ratings yet
- Tu of The OrbitDocument12 pagesTu of The OrbitChavdarNo ratings yet
- Cesarean Scar Niche An Evolving Concern in Clinical Practice - 2021Document11 pagesCesarean Scar Niche An Evolving Concern in Clinical Practice - 2021sauwalsuraiyaNo ratings yet
- 34 Use of Ultrasound in Breast Surgery.Document16 pages34 Use of Ultrasound in Breast Surgery.waldemar russellNo ratings yet
- Imaging of Breast Implants - A Pictorial ReviewDocument18 pagesImaging of Breast Implants - A Pictorial Reviewcomfica.formacion1.2023No ratings yet
- Cancer de Cervix 2019pdfDocument6 pagesCancer de Cervix 2019pdfCristian RodríguezNo ratings yet
- RG 232025065Document21 pagesRG 232025065rulitoss_41739No ratings yet
- Cranio Pha Ryn Gio MaDocument3 pagesCranio Pha Ryn Gio MaSerious LeoNo ratings yet
- Peled 2012 Ann Surg Skin Sparing Immediate ReconstructionDocument8 pagesPeled 2012 Ann Surg Skin Sparing Immediate ReconstructionAndreea PopescuNo ratings yet
- Valeur 2015Document16 pagesValeur 2015Nourma Kusuma WinawanNo ratings yet
- Diagnosing Breast Cancer by Using Raman SpectrosDocument7 pagesDiagnosing Breast Cancer by Using Raman SpectrosVidal VillanuevaNo ratings yet
- Eyelid TattoingDocument15 pagesEyelid Tattoing小島隆司No ratings yet
- Toag 7 4 000 27000Document9 pagesToag 7 4 000 27000Dian Putri NingsihNo ratings yet
- Argument For The Conservative Management of Mandibular AmeloblastomasDocument5 pagesArgument For The Conservative Management of Mandibular AmeloblastomasVincentius Novian RomilioNo ratings yet
- Anaesthesia For Breast Surgery: Andrew J Westbrook Fcarcsi Donal J Buggy MD MSC Dipmedeld Frcpi Fcarcsi FrcaDocument4 pagesAnaesthesia For Breast Surgery: Andrew J Westbrook Fcarcsi Donal J Buggy MD MSC Dipmedeld Frcpi Fcarcsi FrcajonathanNo ratings yet
- Diagnostic and Therapeutic Pieges Before Clinicoradiological Elements Eviding A Mandibular AmeloblastomaDocument4 pagesDiagnostic and Therapeutic Pieges Before Clinicoradiological Elements Eviding A Mandibular AmeloblastomaAnjay MabarNo ratings yet
- Giant Liposarcoma in Left ThighDocument3 pagesGiant Liposarcoma in Left ThighInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unveiling Breast Cancer Metastasis Through An Advanced X-Ray Imaging Approach - s41598-024-51945-4Document9 pagesUnveiling Breast Cancer Metastasis Through An Advanced X-Ray Imaging Approach - s41598-024-51945-4Guilherme de OliveiraNo ratings yet
- Breast Ultrasound For The Interventionalist: Madhavi Raghu, MD, and Regina Hooley, MDDocument7 pagesBreast Ultrasound For The Interventionalist: Madhavi Raghu, MD, and Regina Hooley, MDrasminojNo ratings yet
- Growth Patterns of Craniopharyngiomas: Clinical Analysis of 226 PatientsDocument16 pagesGrowth Patterns of Craniopharyngiomas: Clinical Analysis of 226 PatientsAmina GoharyNo ratings yet
- Management of Parapharyngeal-Space TumorsDocument6 pagesManagement of Parapharyngeal-Space Tumorsstoia_sebiNo ratings yet
- Diagnostic Imaging Pathways ArticleDocument6 pagesDiagnostic Imaging Pathways Articlemashuri muhammad bijuriNo ratings yet
- Breast Implant Safety: An Overview of Current Regulations and Screening GuidelinesDocument5 pagesBreast Implant Safety: An Overview of Current Regulations and Screening GuidelinesbbkdabdfaNo ratings yet
- 03 AnatomyDocument9 pages03 AnatomymaytorenacgerNo ratings yet
- 10 1016@j Bpobgyn 2015 11 014Document17 pages10 1016@j Bpobgyn 2015 11 014Marco Julcamoro AsencioNo ratings yet
- Soft Tissue Tumors of The Neck: David E. Webb, DDS, Brent B. Ward, DDS, MDDocument15 pagesSoft Tissue Tumors of The Neck: David E. Webb, DDS, Brent B. Ward, DDS, MDCynthia BarrientosNo ratings yet
- MRI of The Breast and Emerging TechnologiesDocument15 pagesMRI of The Breast and Emerging Technologiesგიორგი ჯიქიძე100% (1)
- Transvaginal US After Bowel Preparation For DeeplyDocument17 pagesTransvaginal US After Bowel Preparation For DeeplySante PlusNo ratings yet
- Omental RhabdoDocument4 pagesOmental RhabdoDaisuke KiritoNo ratings yet
- Mary Rose S. Gargar Bsn-Iv Cancer of The Female ReproductiveDocument9 pagesMary Rose S. Gargar Bsn-Iv Cancer of The Female ReproductiveMary Rose Silva GargarNo ratings yet
- Schwartz's Principles of Surgery 11th EditionDocument13 pagesSchwartz's Principles of Surgery 11th EditionKobe Brian Franco PeterosNo ratings yet
- Diagnostic Imaging Pathways ArticleDocument14 pagesDiagnostic Imaging Pathways Articlemashuri muhammad bijuriNo ratings yet
- 2019 Article 1119Document7 pages2019 Article 1119elvirNo ratings yet
- High-Resolution Magnetic Resonance Imaging Can Reliably Detect Orbital Tumor Recurrence After Enucleation in Children With RetinoblastomaDocument11 pagesHigh-Resolution Magnetic Resonance Imaging Can Reliably Detect Orbital Tumor Recurrence After Enucleation in Children With RetinoblastomakarimahihdaNo ratings yet
- Manejo Ca Cervical BMJDocument5 pagesManejo Ca Cervical BMJNathalia M.No ratings yet
- JurnalDocument35 pagesJurnalAndi MujtahidaNo ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- Leiomiosarkoma VaginaDocument4 pagesLeiomiosarkoma VaginaUci FebriNo ratings yet
- Breast Carcinoma in Axillary Tail of Spence: A Rare Case ReportDocument4 pagesBreast Carcinoma in Axillary Tail of Spence: A Rare Case Reportrajesh domakuntiNo ratings yet
- Retromolar Embryonal Rhabdomyosarcoma: A CaseDocument6 pagesRetromolar Embryonal Rhabdomyosarcoma: A CaseNabila RizkikaNo ratings yet
- Breast SarcomaDocument4 pagesBreast SarcomaMinh Thư DươngNo ratings yet
- RG Radiologists' Role in Breast Cancer StagingDocument14 pagesRG Radiologists' Role in Breast Cancer StagingAzucena BCNo ratings yet
- Sarcoma of The Breast - An Update On A Rare EntityDocument10 pagesSarcoma of The Breast - An Update On A Rare EntityZaniru Raúl Marín MartínezNo ratings yet
- ASCO 2014 CrossDocument6 pagesASCO 2014 Crossdrrajeshb77No ratings yet
- RADIOLOGY 1.6 Introduction To MammographyDocument9 pagesRADIOLOGY 1.6 Introduction To MammographyZazaNo ratings yet
- A Pictorial Review of Postpartum ComplicationsDocument25 pagesA Pictorial Review of Postpartum ComplicationsGabriela Serra del CarpioNo ratings yet
- A Case Report On Liposarcoma of BreastDocument6 pagesA Case Report On Liposarcoma of BreastSunilKumar CNNo ratings yet
- Valentini 2016Document7 pagesValentini 2016Pepe pepe pepeNo ratings yet
- Ectopico en Cicatriz de Cesarea, 2022Document12 pagesEctopico en Cicatriz de Cesarea, 2022rafael martinezNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleGrace Juniaty GozaliNo ratings yet
- BCR 2015 210918Document3 pagesBCR 2015 210918giant nitaNo ratings yet
- Loukas 2007Document4 pagesLoukas 2007giant nitaNo ratings yet
- AspergillosisDocument12 pagesAspergillosisgiant nitaNo ratings yet
- Breast 2Document10 pagesBreast 2giant nitaNo ratings yet
- Heterogeneous Imaging Features of Aspergillosis at F FDG Pet/CtDocument11 pagesHeterogeneous Imaging Features of Aspergillosis at F FDG Pet/Ctgiant nitaNo ratings yet
- Research Gate Imaginglungmanifestationsof HIVAIDSDocument17 pagesResearch Gate Imaginglungmanifestationsof HIVAIDSgiant nitaNo ratings yet
- LCH 3Document12 pagesLCH 3giant nitaNo ratings yet
- TB Child ExtrapulmonaryDocument9 pagesTB Child Extrapulmonarygiant nitaNo ratings yet
- Blaser 2015Document12 pagesBlaser 2015giant nitaNo ratings yet
- Transplantology 02 00011Document9 pagesTransplantology 02 00011giant nitaNo ratings yet
- Ali 2Document7 pagesAli 2giant nitaNo ratings yet
- GTN 3Document12 pagesGTN 3giant nitaNo ratings yet
- DD Osteogenesis ImperfectaDocument5 pagesDD Osteogenesis Imperfectagiant nitaNo ratings yet
- TB 2Document11 pagesTB 2giant nitaNo ratings yet
- Narita 2014Document1 pageNarita 2014giant nitaNo ratings yet
- Cranium 3Document26 pagesCranium 3giant nitaNo ratings yet
- LCH 5Document9 pagesLCH 5giant nitaNo ratings yet
- GTN 6Document13 pagesGTN 6giant nitaNo ratings yet
- LCH 2Document10 pagesLCH 2giant nitaNo ratings yet
- Gambar PatomekanismeDocument10 pagesGambar Patomekanismegiant nitaNo ratings yet
- Pseudo 1Document20 pagesPseudo 1giant nitaNo ratings yet
- Chapter 2 Suffixes (2024)Document29 pagesChapter 2 Suffixes (2024)mohammadmehrabinia592No ratings yet
- Unit V R2019Document46 pagesUnit V R2019Gayathri RadhaNo ratings yet
- Surgical Treatment of Chronic Subdural Hematoma CLDocument12 pagesSurgical Treatment of Chronic Subdural Hematoma CLNikola StevanovicNo ratings yet
- Vaginal SlingDocument11 pagesVaginal Slinghoria raduNo ratings yet
- Vascular Surgery in OncologyDocument578 pagesVascular Surgery in OncologyJuan RivasNo ratings yet
- The Central Nervous SystemDocument41 pagesThe Central Nervous Systemhijrah nafeerNo ratings yet
- Form 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedDocument2 pagesForm 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedRaju.PalNo ratings yet
- Structure and Function of Large IntestineDocument40 pagesStructure and Function of Large IntestineAjay SinghNo ratings yet
- Pentacam 2Document18 pagesPentacam 2AURA PUTRINo ratings yet
- Direction: Encircle The Letter of The Correct AnswerDocument2 pagesDirection: Encircle The Letter of The Correct Answerariel agos100% (1)
- Artikel Nama Medis DhionDocument2 pagesArtikel Nama Medis DhionDhion HernandoNo ratings yet
- Critical Limb IschemiaDocument2 pagesCritical Limb IschemiaDorin DvornicNo ratings yet
- Nasopalatine Nerve BlockDocument29 pagesNasopalatine Nerve Blockoutright RohitNo ratings yet
- Muhammad Rashid, Humaira Saleem, Saeed Bin Ayaz, Ijaz-Un-Nabi, Rashida Hussain, Faisal ManzoorDocument7 pagesMuhammad Rashid, Humaira Saleem, Saeed Bin Ayaz, Ijaz-Un-Nabi, Rashida Hussain, Faisal ManzoorEMIRZA NUR WICAKSONONo ratings yet
- Histology Slides For MBBS 1st Year (With Identification Points) - MedicoholicDocument79 pagesHistology Slides For MBBS 1st Year (With Identification Points) - MedicoholicPatel OmNo ratings yet
- Zahra WiDocument8 pagesZahra WiYacine Tarik AizelNo ratings yet
- Medical EthicsDocument155 pagesMedical EthicsKiran ToorNo ratings yet
- Abdominal HerniaDocument2 pagesAbdominal HerniaAshan BopitiyaNo ratings yet
- Sonosite 180 and 180 Plus UltrasoundDocument2 pagesSonosite 180 and 180 Plus UltrasoundHAITHM MURSHEDNo ratings yet
- Pi Is 0085253815493731Document8 pagesPi Is 0085253815493731Achmad DainuriNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaGenio OscarNo ratings yet
- CIN SeminarDocument53 pagesCIN SeminarA PoudelNo ratings yet
- Cardiac Science AED-9210 Defibrillator - Service Manual PDFDocument82 pagesCardiac Science AED-9210 Defibrillator - Service Manual PDFFábio Vitor MartinsNo ratings yet
- IV-B Total Parenteral Nutrition (TPN) and Central Venous Pressure Line (CVP) / Mechanical VentilatorDocument23 pagesIV-B Total Parenteral Nutrition (TPN) and Central Venous Pressure Line (CVP) / Mechanical VentilatorRio DanteNo ratings yet
- Atrial Fibrillation: Anish DhakalDocument33 pagesAtrial Fibrillation: Anish DhakalDrjawadhussain HussainNo ratings yet