Professional Documents
Culture Documents
LCH 3
Uploaded by
giant nitaCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
LCH 3
Uploaded by
giant nitaCopyright:
Available Formats
REVIEW
published: 08 March 2021
doi: 10.3389/fmed.2020.582581
Update on Pulmonary Langerhans
Cell Histiocytosis
Elzbieta Radzikowska*
III Department of Lung Diseases and Oncology, National Tuberculosis and Lung Diseases Research Institute, Warsaw, Poland
Pulmonary Langerhans cell (LC) histiocytosis (PLCH) has unknown cause and is a
rare neoplastic disorder characterized by the infiltration of lungs and various organs
by bone marrow-derived Langerhans cells with an accompanying strong inflammatory
response. These cells carry somatic mutations of BRAF gene and/or NRAS, KRAS,
and MAP2K1 genes, which cause activation of the mitogen-activated protein kinase
(MAPK)/extracellular signal-regulated kinase (ERK) signaling pathway. PLCH occurs
predominantly in young smokers, without gender predominance. Lungs might be
involved as an isolated organ or as part of a multiorgan disease. High-resolution
computed chest tomography plays an outstanding role in PLCH diagnosis. The
typical radiological picture of PLCH is the presence of small intralobular nodules,
“tree in bud” opacities, cavitated nodules, and thin- and thick-walled cysts, frequently
confluent. Histological examination of the lesion and demonstration of characteristic
eosinophilic granulomas with the presence of LCs that display antigen CD1a or CD207
Edited by: in immunohistochemistry are required for definite diagnosis. Smoking cessation is the
Kai-Feng Xu,
Peking Union Medical College
most important recommendation for PLCH patients, but treatment of progressive PLCH
Hospital (CAMS), China and multisystem disease is based on chemotherapy. Recently, new targeted therapies
Reviewed by: have been implemented.
Xiaowen Hu,
Anhui Provincial Hospital, China Keywords: pulmonary Langerhans cell histiocytosis, adults, lung, BRAF, MAPK
Paola Rottoli,
University of Siena, Italy
Itziar Astigarraga, INTRODUCTION
Cruces University Hospital, Spain
*Correspondence: Pulmonary Langerhans cell (LC) histiocytosis (PLCH) is a rare neoplastic disorder of unknown
Elzbieta Radzikowska etiology, characterized by the infiltration of the lungs and various organs by bone marrow-derived
e.radzikowska@wp.pl LCs with an accompanying strong inflammatory response (1). These cells carry somatic mutations
orcid.org/0000-0002-2585-8594 of the BRAF gene and/or NRAS, KRAS, and MAP2K1 genes, which cause activation of the
mitogen-activated protein kinase (MAPK)/extracellular signal-regulated kinase (ERK) signaling
Specialty section: pathway (2–5).
This article was submitted to
The histiocytic diseases have been reclassified into five categories; LCH is considered a member
Pulmonary Medicine,
of group L, along with Erdheim–Chester disease, indeterminate cell histiocytosis, and mixed
a section of the journal
Frontiers in Medicine LCH/Erdheim–Chester disease (1, 6). PLCH occurs predominantly in young smokers and shows no
predominance in either sex. The lungs may be involved as isolated organs or as part of a multisystem
Received: 12 July 2020
disease (7). Proliferating LCs form nodular lesions of various sizes, which infiltrate neighboring
Accepted: 21 December 2020
Published: 08 March 2021 tissues and damage their structure. In adults, LCH most commonly affects the lungs, bones, skin,
and pituitary gland. The involvement of lymphopoietic organs (e.g., lymph nodes, liver, spleen, and
Citation:
Radzikowska E (2021) Update on
bone marrow), alimentary system, and central nervous system (CNS) is rare. In the course of LCH,
Pulmonary Langerhans Cell pulmonary lesions may be isolated, occur after chronic systemic disease, or are an initial sign of
Histiocytosis. Front. Med. 7:582581. disease. The isolated pulmonary form of LCH is observed in approximately 50–70% of patients
doi: 10.3389/fmed.2020.582581 with PLCH (8–11).
Frontiers in Medicine | www.frontiersin.org 1 March 2021 | Volume 7 | Article 582581
Radzikowska Update on PLCH
Single-system LCH (SS-LSH) comprises single or multiple Recently, it was noticed that 20–33% of patients smoked
involvement of the following single organs or systems: both cigarettes and cannabis [(18), personal observations].
Bone, with involvement of a single or multiple bones and The intensity and smoking duration do not influence the
many foci in many bones; development of PLCH. Isolated PLCH in children is extremely
Skin; rare; the disease is reportedly associated with passive exposure
Lymph nodes, excluding lymph nodes that drain the area to tobacco smoke in the majority of pediatric patients,
of histiocyte infiltration or multiple lymph nodes (i.e., more and ∼10–30% of children with multisystem LCH exhibit
than one lymph node group); pulmonary lesions (11, 19). Familial occurrence of LCH has been
Hypothalamus–hypophysis/CNS; reported, but no genetic predisposition toward LCH has been
Isolated pulmonary involvement; found (7).
Other, with involvement of oral mucosa, thyroid, thymus,
or intestine.
Multisystem LCH (MS-LCH) comprises disease in which two PATHOGENESIS
or more organs or systems are affected:
Involvement of critical organs, e.g., hemopoietic system, There have been many investigations regarding the pathogenesis
spleen, liver; of LCH; the finding that dendritic cells with mutations in MAPK
No involvement of critical organs. pathway genes contribute to the development of the disease has
yielded new insights. Dendritic cells are a heterogeneous group
The involvement of specific areas and bones [e.g., vertebrae
of cells, which mainly serve to process and present antigens to
(possible compression spinal fracture and damage to the spinal
immune cells. Normal LCs are present in the skin, as well as
cord), orbital bones, mastoid process, sphenoid bone, and
beneath the epithelia of the bronchial tree and other mucosae
temporal bones with transition into soft tissue (possible injury
(3, 6). Toll-like receptors, expressed on pathogen-sensing cells,
to facial nerves and pituitary gland)] is associated with the risk of
and factors released from damaged or dying cells, stimulate
CNS involvement, which impacts decisions regarding treatment
the activity of normal LCs. Subsequently, the immunological
(7, 12).
response involves the migration of activated dendritic cells to
Previously, the lungs were considered as a “risk organ,” but
the nearest lymph nodes and presentation of antigens to naive T
multivariable analysis of cohorts of 420 children with MS-
lymphocytes. In addition, tolerance to harmless inhaled antigens
LCH showed that lung involvement was not the significant
is mediated by normal LCs (20).
prognostic variable (13). However, patients with lung lesions
Tobacco smoke plays a major role in the development of
have a high risk of developing life-threatening complications
PLCH (21). It causes inflammatory cell accumulation in the
(e.g., pneumothoraces, pulmonary infections). Recently, Le Louet
lungs; these cells include LCs, which release cytokines such as
et al. (14) presented the assessment of French LCH registry,
tumor necrosis factor alpha, interleukin 1 beta, granulocyte-
and it was found that severe lung involvement in children was
macrophage colony-stimulating factor, transforming growth
associated with high mortality. These findings suggested revision
factor beta, and the dendritic cell chemokine (chemokine
of treatment guidelines for this group of patients.
ligand 20) (22). In addition, bronchial epithelial cells and
fibroblasts release granulocyte-macrophage colony-stimulating
EPIDEMIOLOGY factor, which is a strong mitogenic factor for LCs.
Moreover, PLCH lesions exhibit elevated expression of
LCH has an estimated prevalence in adults of 1–2/1,000,000.
osteopontin, a glycoprotein that induces chemotactic activity
However, there have been few population-based epidemiological
in macrophages, monocytes, and dendritic cells, including LCs.
studies regarding this disease. In Japanese hospitalized patients,
Activated pathological LCs show strong lymphocyte-stimulating
the prevalence rates of PLCH were reported to be 0.07/100,000
properties and are characterized by elevated expression of CD40,
in women and 0.27/100,000 in men. PLCH is presumed to affect
CD80, and CD86. Previous studies have yielded inconsistent
approximately 5% of patients undergoing open lung biopsy. The
results regarding the importance of interleukin-17 released by
prevalence of PLCH may be underestimated due to the nature of
T lymphocytes in the pathogenesis of histiocytic lesions. This
the disease (7, 15).
cytokine promotes the development of giant cells and formation
PLCH affects young people in the third and fourth decades
of granulomas. Elevated expression of the antiapoptotic protein,
of life, with no sex predominance. Approximately 90 to
Bcl-xL, within histiocytic granulomas maintains the pathogenic
95% of patients with PLCH are tobacco smokers (16, 17).
process (23).
Abbreviations: ARAF, A serine/threonine kinase; AKT, serine/threonine kinase;
In addition to inflammation, granuloma formation is
BRAF, B serine/threonine kinase; 2-CDA, 2-chloro-2’-deoxyadenosine; CNS, accompanied mPAP, mean pulmonary arterial presure; by
central nervous system; ERK, extracellular signal-regulated kinase; HRCT, remodeling of the lung parenchyma. Cystic destruction of the
High-resolution computed tomography; LAM, lymphangioleiomyomatosis; LC, lung is presumably caused by activation of metalloproteinases
Langerhans cell; LCH, Langerhans cell histiocytosis; MAPK, mitogen-activated
2 and 9, produced by dendritic cells, LCs, and monocytes.
protein kinase; MS-LCH- multisystem Langerhans cell histiocytosis; mTOR,
mechanistic target of rapamycin; P, phosphorylation; PIK, phosphatidylinositol Moreover, elevated expression of transforming growth factor beta
kinase; PIP-1, phosphatidylinositol monophosphate; PIP-2, phosphatidylinositol released by granuloma cells causes fibrotic lesions (12).
biphosphate; PLCH, pulmonary Langerhans cell histiocytosis; PTEN, phosphate There have been a number of investigations regarding the
and tensin homolog; SS-LCH single system Langerhans cell histiocytosis. pathogenesis of PLCH. Inflammatory cell accumulation and the
Frontiers in Medicine | www.frontiersin.org 2 March 2021 | Volume 7 | Article 582581
Radzikowska Update on PLCH
presence of LCs with dysfunctional apoptosis, as well as clonal Mutations in genes involved in the MAPK pathway related
proliferation, have been associated with the onset of PLCH. to precursors of distinct macrophage types (i.e., bone marrow or
Identification of the role of the RAS/MAPK signaling pathway yolk sac) result in the occurrence of an overlapping syndrome of
in the pathogenesis of LCH was a key discovery regarding the LCH and Erdheim–Chester disease or chronic myeloid leukemia.
pathogenetic mechanism of this disorder (24). This pathway Notably, PLCH was recently recognized as a neoplasm with a
transmits proliferative signals from the cell surface via the RAS strong inflammatory component (30).
pathway to phosphorylate MAPK and ERK, which transmit
signals to the nucleus. The MAPK pathway regulates the activities
of many enzymatic proteins and transcription factors. Activating CLINICAL PRESENTATION
mutations of the BRAF, ARAF, MAP2K1, N/K/HRAS, and
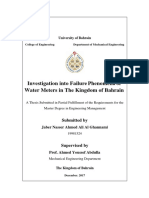
PIK3CA genes have been found in patients with PLCH (25– Respiratory Symptoms
27) (Figure 1). The BRAF V 600E mutations were found in Patients with PLCH exhibit dry cough (50–70%), reduced
50% of LCH pulmonary nodules and MAP2K1 in an additional exercise tolerance (40–80%), exertional dyspnea (40–87%),
20% of cases (26). Moreover, whole-exome sequencing analysis fatigue (50–80%), weight loss (20–30%), chest pain (10–30%),
revealed MAP2K1 mutations in seven of 21 BRAF-wild-type night sweats (10–20%), and fever (10–15%). Approximately
LCH biopsy tissue samples, but not in BRAF-mutant specimens 10–30% of affected patients are diagnosed following incidental
(5). The activation of ERK was detected in >90% of patients pneumothorax. Pneumothorax occurs during the course of
with LCH. In patients with multisystem LCH, mutation of the disease in 30–45% of affected patients (17, 31). Changes are found
BRAF V 600E gene may occur in myeloid cells; in patients with incidentally on routine chest X-rays without symptoms in 5–25%
single-system LCH, mutations may occur in cells originating of affected patients. Dyspnea at rest and characteristics of right-
from peripheral lesions (28). The single-cell analysis showed ventricular circulatory failure occur in the late stages of PLCH.
cellular, transcriptomic, and epigenomic heterogeneity among More than 10% of patients with PLCH develop pulmonary
LCH cells, which ware connected with the development of hypertension; it is not always related to the exacerbation of
LCH lesions. LCH cells share enrichment of genes involved in pulmonary lesions but may be due to the involvement of
interferon (IFN) signaling and antigen presentation, indicating pulmonary vessels that occurs during the course of the disease
the inflammatory nature of the disease. In addition, genes (9, 11). Pulmonary hypertension and dynamic hyperinflation
involved in cell cycle pathways and DNA repair were presented. are the most important factors that limit exercise capacity in
It is suggested that interindividual differences in subsets of LCH PLCH patients (32). Moderate or severe pulmonary hypertension
cells may be connected with clinical presentation of the disease. [mean pulmonary arterial pressure (mPAP) >35 mmHg] was
Validation of the differences in LCH subset composition in bulk revealed in 92% of the PLCH patients who presented for lung
RNA sequencing, immunohistochemistry, immunofluorescence transplantation (33).
imaging in a large cohort of LCH patients might be helpful in Between 25 and 50% of patients without pulmonary
patient management (29). symptoms at the time of presentation show symptoms related
FIGURE 1 | MEK-mitogen activated protein kinase–extracellular signal-regulated kinase (ERK) signaling cascade of the mitogen-activated protein kinase (MAPK)
pathway and phosphoinositide 3-kinase (PI3K)–AKT-serine/threonine protein kinase Akt pathway. Diagram of RAS protein activation.
Frontiers in Medicine | www.frontiersin.org 3 March 2021 | Volume 7 | Article 582581
Radzikowska Update on PLCH
to other organ involvement, such as polyuria–polydipsia (20– are spared (>90%). In children, both lungs are symmetrically
30%), bone pain (20–50%), and oral mucosa or skin lesions affected and lesions may be present in the lower lobes (14). In
(∼10%). Initial evaluation of patients with LCH requires whole- some patients, different degrees of pneumothorax are present. In
body assessment. Symptoms typically arise 6–20 months prior patients with PLCH, other radiological symptoms of smoking-
to recognition of the disorder; in some affected patients, the related diseases are often visible (e.g., emphysematous bullae or
diagnosis is established after many years of observation. Patients ground-glass opacities). Enlarged lymph nodes may be present
with spontaneous pneumothorax as an initial symptom of the in approximately 10% of affected patients. Signs of pulmonary
disease are reportedly younger, more frequently men, and exhibit hypertension, megalocardia, and enlarged pulmonary trunk are
greater respiratory impairment compared with those who do not observed in patients with advanced disease (35).
have pneumothorax (17).
Positron Emission Tomography
Radiological Findings Positron emission tomography with 18 F-fluorodeoxyglucose has
Chest Radiography limited value in the assessment of patients with PLCH. Only 20–
Standard chest radiography has limited value, as multiple lesions 25% of patients show higher 18 F-fluorodeoxyglucose uptake in
may be small. In patients with advanced disease, nodular, the lungs, particularly in thick-walled cysts and nodular lesions.
reticular, and cystic lesions are visible in the middle and upper Positron emission tomography is more sensitive than CT in terms
lung fields (Figure 2). Lung volumes are typically preserved but
may be diminished in patients with a history of pneumothorax
and pleurodesis. Enlargement of the hilar and mediastinal lymph
nodes is present in approximately 10% of affected patients (11).
Computed Tomography
High-resolution computed tomography (HRCT) plays a major
role in the diagnosis of PLCH (7, 34). The typical findings
are centrilobular nodules (frequently with a “tree-in-bud”
appearance), nodules with or without a lacuna, and initially
thick-walled cysts of various shapes (these may be isolated or
confluent with a “cloverleaf ” appearance) (Figures 3–5). As the
disease progresses, the cysts become larger and thin-walled.
Lesions have a characteristic distribution, with predominance in
the upper and middle parts of the lungs; the costophrenic angles
FIGURE 3 | High-resolution computed tomography (HRCT) scan of a
pulmonary Langerhans cell histiocytosis (PLCH) patient. Multiple intralobular
nodules, nodules with cavitations, and small nodular lesions in both lungs.
FIGURE 2 | X-ray film of a pulmonary Langerhans cell histiocytosis (PLCH) FIGURE 4 | High-resolution computed tomography (HRCT) scan of a
patient. Multiple reticular and nodular changes in the upper and middle parts pulmonary Langerhans cell histiocytosis (PLCH) patient. Multiple cystic lesions,
of both lungs, with an increase in lung volume. frequently confluent with bizarre shapes.
Frontiers in Medicine | www.frontiersin.org 4 March 2021 | Volume 7 | Article 582581
Radzikowska Update on PLCH
Bronchoscopy and Bronchoalveolar Lavage
Bronchoscopy is typically performed to exclude other disorders,
especially infections. The diagnostic value of transbronchial
biopsy is limited and estimated at 10–50% due to focal
distribution of lesions, despite the bronchiolocentric nature of
the disease (40, 41). Transbronchial biopsy is most useful in
patients with nodular lesions but in patients with cystic lesions
is associated with a high risk of pneumothorax. A new technique
for lung tissue sampling, cryobiopsy, yields a diagnosis in ∼70%
of patients with interstitial lung disease. The value of this technic
in PLCH is under evaluation because in only a few cases has
diagnosis of PLCH been established by cryobiopsy (42, 43). The
presence of >5% cells with CD1a expression in bronchoalveolar
lavage (BAL) fluid with a typical radiological pattern on chest
HRCT is specific for PLCH but is detected in only 0–25% of
affected patients (44). Auerswald et al. (45) noticed that all their
six patients with histologically proven histiocytosis displayed
more than 5% CD1-positive cells, but Torre and Harari (46)
FIGURE 5 | High-resolution computed tomography (HRCT) scan of a
were able to establish PLCH in four (25%) out of 16 patients
pulmonary Langerhans cell histiocytosis (PLCH) patient. Large confluent cystic on the basis of BAL assessment. Similarly, only three (38%)
lesions in both lungs. out of eight patients with PLCH presented by Baqir et al. (41)
and 10 (25%) out of 40 patients presented by Elia et al. (11)
in whom BAL was performed displayed the presence of CD1a-
positive cells over 5%. In our group of 38 patients with PLCH,
only in eight (21%) did BAL assessment have a diagnostic
of identifying bone lesions, particularly those that are subclinical,
value (47).
as well as those that involve lymph nodes, liver, spleen, or thyroid.
Positron emission tomography is reportedly sensitive for the
Lung Biopsy
assessment of early response to treatment and disease relapse
Open lung biopsy is the gold standard for a definitive diagnosis
(36, 37).
of PLCH. In patients with LCH confirmed by histological
examination of specimens obtained from other foci (e.g., skin,
Laboratory Tests mucosa, or bones), it is not necessary to confirm pulmonary
The results of laboratory tests are usually unremarkable. lesions (7).
However, patients with PLCH often show elevated levels of
serum inflammatory markers. Serum hyperosmolarity with lower Histological Examination
urine specific gravity and hypoosmolarity are observed in PLCH has a focal, bronchiolocentric localization. Initially,
patients with diabetes insipidus. Elevated serum levels of hepatic inflammation with eosinophilic granuloma formation occurs
enzymes and bilirubin are characteristic of liver involvement near small bronchi and bronchioles, destroying their walls; it
(7). Fluid phase biopsy is valuable for the assessment of exhibits varying degrees of extension into the adjacent lung
BRAF mutations in patients who are potential candidates for interstitium. Frequently, macrophages with dark inclusions are
targeted therapy. observed; these macrophages are characteristic of exposure
to inhaled fumes, mainly tobacco smoke. Nodules contain a
mixture of inflammatory cells, such as T cells, macrophages,
Pulmonary Function Testing monocytes, and LCs; these LCs are relatively large, with
Patients with PLCH exhibit various patterns of ventilation a pale, slightly eosinophilic cytoplasm and a convoluted
disorders. Initially, approximately 20% of affected patients have nucleus that exhibits a longitudinal crease resembling a coffee
normal values on pulmonary function tests. Obstruction with bean. Electron microscopic examination shows pentalammelar
hyperinflation is the main abnormality and can often be reversed structures (consisting of lectin) in the cytoplasm associated
to some degree. Restricted breathing is uncommon and mainly with the cell membrane; these so-called Birbeck granules are
affects individuals with recurrent pneumothorax and pleurodesis. characteristic of LCs. These structures can also be identified by
The most common abnormality is reduced diffusing capacity immunohistochemistry using antibodies against langerin (i.e.,
of the lungs for carbon monoxide, which is observed in CD207). LCs show CD1a expression, which is necessary for
approximately 70–90% of affected patients. The 6-min walk test diagnosis (24). The expression of S-100 protein is not specific
is a useful examination; desaturation during exercise is a sensitive but may be present. Inflammatory eosinophilic granulomas may
marker of lung impairment in patients with less advanced disease, be observed, depending on the stage of disease progression. The
and a reduced walking distance is observed in patients with central part of the nodule has a lacuna, which is presumably
advanced disease (17, 38, 39). a component of the remaining bronchiole lumen or the
Frontiers in Medicine | www.frontiersin.org 5 March 2021 | Volume 7 | Article 582581
Radzikowska Update on PLCH
effect of cytokine and metalloproteinase-mediated destruction. TABLE 1 | Diseases with a cystic pattern of lung lesions.
Subsequently, the inflammation regresses; however, fibrosis
• Pulmonary Langerhans cell histiocytosis
develops in the form of stellar scars or confluent cystic
• Lymphangioleiomyomatosis (LAM)
cavities in the fibrous ring. At this stage, LCs are absent. ◦
Sporadic LAM
In LCH lesions, LCs constitute 1–80% of cells (mean ∼8%) ◦
Tuberous sclerosis complex LAM
(3). Lung specimens from patients with PLCH may also show
• Birt–Hogg–Dubé syndrome
signs of other smoking-related diseases, such as bronchiolitis,
• Erdheim–Chester disease
desquamative interstitial pneumonia, respiratory bronchiolitis
• Lymphatic disorders
with accompanying interstitial lung disease, or emphysema.
In patients with advanced disease, the internal walls of both
◦
Lymphocytic interstitial pneumonia
arteries and veins are thickened, resulting in pulmonary
◦
Light-chain deposition disease
hypertension (48).
◦
Amyloidosis
◦
Hyper-IgE syndrome
Patients who qualify for targeted therapy must be tested for
• Genetic disorders
mutations in the BRAF, ARAS, NRAS, KRAS, and MAP2K genes ◦
Ehlers–Danlos syndrome
(5). Moreover, as a novel diagnostic technique for monitoring
◦
Neurofibromatosis
patients undergoing treatment with BRAF inhibitors, analysis of
◦
Marfan syndrome
BRAF V600E gene mutations in cell-free DNA in serum has been
◦
Proteus syndrome
implemented (49, 50).
• Congenital pulmonary airway malformations
• Infections
DIAGNOSIS ◦
Respiratory papillomatosis
◦
Staphylococcal pneumonia
Definite diagnosis of PLCH requires adequate clinical ◦
Pneumocystis jirovecii
presentation and the identification of LCs in biopsy specimens ◦
Endemic fungal diseases (coccidiomycosis, paragonimiasis)
that exhibit either CD207 (langerin) or CD1a.
• Emphysema
Probable diagnosis of PLCH relies on clinical presentation
• Alpha-1 antitrypsin deficiency
confirmed radiologically (characteristic cysts and nodules
• Post-traumatic pseudocysts
mainly observed in upper and middle lung fields on chest
• Pulmonary neoplasms
CT). Histological verification of all extrapulmonary lesions is ◦
Adenocarcinoma
recommended (7). ◦
Lymphoma
◦
Mesenchymal hamartoma
Differential Diagnosis ◦
Pleuropulmonary blastoma
Disorders that should be taken into account while diagnosing the
• Sarcomas
patients with cystic pulmonary lesions are presented in Table 1. ◦
Angio and osteosarcomas
In patients with nodular lesions, diseases such as neoplasms, ◦
Synovial cell sarcoma
sarcoidosis, hypersensitivity pneumonitis, and infections are in ◦
Leiomyosarcoma
the scope of differential diagnosis (7).
◦
Rhabdomyosarcoma
◦
Endometrial stromal sarcoma
TREATMENT ◦
Wilms tumor
◦
Ewing sarcoma
Treatment of LCH depends on the disease activity and affected • Metastatic tumors
organs, including lesions in critical organs and high-risk bones, ◦
Adenocarcinoma of genitourinary and gastrointestinal tract
as well as the degree of damage (Figure 6). ◦
Breast Cancer
◦
Cancers of the head and neck
Smoking Cessation
Because of the crucial role of tobacco smoke in the
development of PLCH, smoking cessation is the most
important recommendation for affected patients. In ∼50% is becoming a challenge for both patients and doctors [(52),
of patients with isolated PLCH, smoking cessation leads to personal observation].
partial regression and subsequent stabilization of the disorder
without immunosuppressive therapy (16, 51). However, patients Glucocorticosteroids
require systematic follow-up examinations because reactivation Systemic corticosteroid therapy has been advised for many
of the disease can occur in the lungs or other organs. Thus far, years; it has been reportedly associated with symptomatic,
no biological markers have been found to identify patients in radiological, and functional improvements. However, there
whom smoking cessation would be sufficient and patients in have been insufficient studies to determine the appropriate
whom the disease is likely to progress despite smoking cessation. corticosteroid dose and duration of treatment, as well as
Cessation of both cigarette smoking and marijuana smoking comparative studies with respect to smoking cessation. It is
Frontiers in Medicine | www.frontiersin.org 6 March 2021 | Volume 7 | Article 582581
Radzikowska Update on PLCH
five patients with PLCH; however, one of these patients exhibited
relapse. Pardanani et al. (62) and Adam et al. (63) in five and
seven patients with PLCH who received 2-CDA, respectively
reported over than 60% response rate.
Cladribine treatment in adult PLCH patients is a
subject of an ongoing phase II clinical trial (NCT01473797,
www.ClinicalTrials.gov). The most frequently observed severe
adverse event during the course of cladribine treatment is
cytopenia, whereas the most severe event associated with
vinblastine is neuropathy. For patients with disease progression
after cladribine treatment, salvage therapy is cytarabine
administered at a dose of 100 mg/m2 on five consecutive days
at 4-week intervals. Another phase II trial (NCT04121819,
www.ClinicalTrials.gov) to investigate the efficacy and safety of
cytarabine in adult patients with LCH is currently underway.
Notably, the preferred chemotherapeutic regimen in patients
with brain lesions is cytarabine and cladribine because both
drugs cross the blood–brain barrier.
FIGURE 6 | Management of pulmonary Langerhans cell histiocytosis (PLCH). Clofarabine is another drug that is effective as salvage therapy
in children and is the subject of another ongoing phase II clinical
trial (NCT02425904). In addition, severe lung cystic lesions
and chemotherapy, particularly with concomitant corticosteroid
possible that some effects of therapy are due to smoking cessation, treatment, are predisposing factors to opportunistic infections,
rather than steroid treatment (10). In addition, relapse after particularly Pneumocystis jiroveci pneumonia. Grobost et al.
treatment is common (∼80%); long-term corticosteroid therapy (61) recommended that sulfamethoxazole/trimethoprim and
is associated with many (sometimes severe) adverse effects. valaciclovir prophylaxis should be administered during cessation
Therefore, this treatment is no longer recommended. However, of 2-CDA treatment, as well as for 6 months afterward.
inhaled corticosteroids may be useful for treatment of patients
with reversible obstruction (7).
Chemotherapy Targeted Therapies
Various chemotherapy regimens have been proposed for use in Vemurafenib and Other BRAF Inhibitors
children with LCH, but they have failed to show satisfactory The presence of mutations in genes involved in the MAPK
results in adults. The disease has a diverse clinical course pathways in patients with PLCH implies that targeted therapy
in adults, particularly in patients with isolated PLCH, and may be useful. Vemurafenib, a BRAF kinase inhibitor, is
many drugs are differently tolerated (53–55). Vinblastine, reportedly an effective treatment in patients with LCH (64, 65,
methotrexate, mercaptopurine, and etoposide have shown 70). However, this drug did not eliminate all LCs; discontinuation
benefits in some patients with multisystem LCH, but their of treatment resulted in disease progression. Diamond et al.
effects in patients with isolated PLCH are controversial (56). (67) reported the beneficial effects of vemurafenib in a group
A retrospective study involving a population of 35 adults with of 22 patients with Erdheim–Chester disease and four patients
LCH (17 patients with pulmonary involvement) treated with with LCH; these patients exhibited a 2-year progression-free
vinblastine and steroids showed a response rate of 70%; however, survival rate of 86% and an overall survival rate of 96%.
the relapse rate was 40% during the 5-year follow-up period (57). Notably, the patients with LCH showed a particularly good
No improvements in ventilation parameters due to vinblastine response. Bhatia et al. (68) reported a partial response in patients
treatment were observed in any patient. Cantu et al. (58) reported with refractory Erdheim–Chester disease overlapping with LCH
that vinblastine treatment was less effective than cladribine or during treatment with another BRAF inhibitor, dabrafenib.
cytarabine in adult patients with multifocal bone disease (28% Recently, Hazim et al. (66) presented results of treatment with
had pulmonary lesions). However, the effects of these treatments vemurafenib and dabrafenib in six adult patients with LCH.
on lung function parameters were not discussed. Recently, Néel Complete and partial responses were noticed in 30 and 50% of
et al. (59) reported an overall response rate of 91% in 22 patients patients, respectively (Table 2).
treated with cladribine; however, disease progression occurred in In a study of children with LCH performed in France, the
30% of these patients during the 5-year follow-up period. presence of BRAF mutations was associated with a weaker
Saven and Burian (60) reported that 2-chloro-2′ - response to first-line treatment (vinblastine and steroids) and
deoxyadenosine (2-CDA) had beneficial effects in 12 patients second-line treatment, as well as a higher proportion of
(six with lung involvement), affording an overall response rate of recurrence (65, 71). However, no correlations were found
75%. Grobost et al. (61) reported that cladribine (three or four between BRAF mutations, clinical presentation, and prognosis in
courses) improved pulmonary function parameters in four of adults (5).
Frontiers in Medicine | www.frontiersin.org 7 March 2021 | Volume 7 | Article 582581
Radzikowska Update on PLCH
TABLE 2 | Targeted therapies in LCH adult patients. time of the first ipsilateral recurrence and the overall number of
Study Trial Patients BRAF Time of Response
pneumothorax recurrences were similar after conservative and
inhibitor response thoracic surgical treatments. Pneumothorax recurrences may be
assessment linked with active disease (18). Notably, pleurodesis does not
Hyman (70) Phase 2 13 ECD Vemurafenib 2 months ORR-43%
constitute a contraindication for lung transplantation (7).
1 LCH
Diamond Phase 2 22 ECD Vemurafenib 2–40 months ORR-61% Treatment of Pulmonary Hypertension
et al. (67) 4 LCH
The progression of PLCH leads to the destruction of
Bhatia (68) Retrospective 7 ECD Dabrafenib 2–40 months ORR-
4 ECD/LCH 100%
lung parenchyma with elements of fibrosis, as well as the
Diamond Prospective 12 ECD Cobimetinib 12 months ORR-89% development of pulmonary hypertension. In a small proportion
et al. (69) 2 LCH of patients, those with stable ventilation parameters may exhibit
Hazim (66) Retrospective 6 LCH 3 Vemurafenib 4–27 months CR-33%
3 Dabrafenib PR-50%
pulmonary hypertension.
Oxygen treatment is the main recommendation for this
CR, complete response; ECD, Erdheim–Chester disease; LCH, Langerhans cell group of patients. Furthermore, drugs that lower pulmonary
histiocytosis; ORR, overall response rate; PR, partial response.
artery blood pressure (e.g., inhibitors of phosphodiesterase and
endothelin receptor, as well as prostacyclin) were shown to
have beneficial effects in patients with PLCH who exhibited
Mitogen-Activated Protein Kinase Inhibitors pulmonary hypertension (78). Also other small series of patients
Drugs that inhibit mitogen-activated kinase 1 (MEK1) and 2, and case reports presented beneficial effects of pulmonary
both downstream of BRAF, were shown to be beneficial in antihypertensive therapies; however, it is not proven as standard
patients with LCH who exhibited MAP2K1 deletion. Lorillion treatment and should be delivered in very experienced centers
et al. (72) reported a good response to trametinib. Cobimetinib, (79, 80).
a MEK1 and 2 inhibitor, was the subject of a clinical trial in
patients with various histiocytic disorders. All patients showed Lung Transplantation
a response to this treatment; the relapse rate was only 10% at 1 Lung transplantation is a salvage therapeutic option for patients
year (69). Studies regarding melanoma cells harboring mutations with features of respiratory failure and those developing
in genes involved in the MAPK pathway showed that dual pulmonary hypertension. The prognosis of patients undergoing
inhibition of BRAF and MEK was more effective and less toxic transplantation does not significantly differ from that of patients
than monotherapy with a BRAF inhibitor. Awada et al. (73) with other interstitial lung diseases. The 1-year survival rate is
reported beneficial results of this treatment in adult patients with 75%; notably, >50% of patients survive for 5 years. Patients with
multisystem LCH. Multiple clinical trials involving BRAF and multisystem LCH and lung involvement have a worse prognosis
other RAS pathway inhibitors in adults and children with LCH after transplantation, and recurrence of LCH in the transplanted
are currently underway (www.ClinicalTrials.gov). organ has been found in approximately 20% of affected patients
(33). Based on 87 transplant patients, Wajda et al. (81) reported
Tyrosine Kinase Inhibitors outcomes similar to those of prior studies; 1-year, 5-year, and 10-
Contradictory results have been reported regarding the effects year survival rates were 85, 49, and 22%, respectively. Moreover,
of imatinib treatment. Montella et al. (74) and Janku et al. the median survival was significantly better for women than for
(75) reported beneficial effects of this drug in a 37-year-old men (mean survival time, 9.3 vs. 3.9 years).
woman with multisystem LCH and in two adult patients with
multisystem LCH, respectively. However, the follow-up periods Follow-Up Examination
in these patients were both shorter than 2 years. In contrast, Patients with PLCH should undergo systematic follow-up
Wagner et al. (76) reported treatment failure in two patients examinations, initially performed after 3–4 months with
treated with imatinib. subsequent evaluations at intervals of 3–12 months, depending
on disease activity (7). HRCT is not necessary at every follow-up
Pneumothorax examination because it is not highly sensitive for evaluation of
Pneumothorax, as the first symptom of PLCH, is observed disease activity (34). Similarly, assessments of organs other than
in 10–30% of affected patients. In addition, these patients the lungs are not required; however, these evaluations should be
have a greater probability of pneumothorax recurrence (∼60%). performed in the event of new symptoms. Pulmonary function
Generally, 30–40% of patients develop this condition during tests are important in follow-up assessment of patients with
long-term observation. Moreover, this group often includes PLCH. Deterioration of exercise tolerance or the presence of new
young men who smoke fewer cigarettes and whose lung symptoms requires close examination. Participation in tobacco
function is more affected by the disease. These data support and marijuana cessation programs is highly recommended.
the recommendation that HRCT should be performed in all
patients with spontaneous pneumothorax to identify patients PROGNOSIS
with possible PLCH (17, 31, 77).
Pleurodesis should be recommended after the first episode The natural course and prognosis of PLCH are unpredictable
of pneumothorax. However, it was recently reported that the and variable. Spontaneous regression and/or stabilization of
Frontiers in Medicine | www.frontiersin.org 8 March 2021 | Volume 7 | Article 582581
Radzikowska Update on PLCH
the disease after smoking cessation, as well as the presence of Air Travel
addiction to substances other than tobacco in some patients, Patients with PLCH have a higher risk of pneumothorax during
results in loss to follow-up for many patients; this may influence air travel. However, the risk is not high; approximately 1%
survival assessment. However, patients with PLCH were reported of patients exhibit this condition, and no severe instances of
to exhibit lower mean survival compared to sex- and age- pneumothorax have been reported thus far (84).
matched members of the general population (7). Vassallo et al.
(9) observed a median survival of 12.5 years in adult patients with CONCLUSIONS
biopsy-proven PLCH.
Reduced spirometry parameters, low diffusing capacity 1. LCH is a rare disorder of unknown etiology caused by clonal
of the lungs for carbon monoxide, severe cystic lesions proliferation of geno- and phenotypically altered LCs.
detected on HRCT, low oxygen arterial pressure, older age, 2. It usually involves the bones, lungs, skin and pituitary,
pulmonary hypertension, and multisystem LCH are negative lymphopoietic organs (lymph nodes, liver, spleen, bone
prognostic factors. Moreover, a higher St. George’s Respiratory marrow), gastrointestinal tract, thyroid, CNS, and others.
Questionnaire (SGRQ) score and continued tobacco smoking 3. PLCH may be as follows: isolated, anticipating even for many
have negative impacts on survival. Tazi et al. (16) presented an years the occurrence of systemic changes, or from the very
early decline of pulmonary function parameters (over 15%) in beginning, the lungs may be one of the sites involved.
40% of newly diagnosed PLCH patients, but in only 10% of them, 4. Tobacco smoke is a crucial causative factor for PLCH.
progression of pulmonary lesions was noticed. Smoking cessation is the most vital recommendation.
Recently, severe lung involvement in children was recognized 5. Chest HRCT has an outstanding importance in PLCH
as a factor that substantially influences the course of the disease diagnosis. Pulmonary lesions are the following: centrilobular
and survival. Early administration of new targeted LCH therapies nodules, nodules with or without a central cavity, initially
and viral infection prophylaxis are suggested (14). thick-walled cysts of various shapes that may convolute,
Patients with PLCH also have a higher risk of forming the so-called clover leaves. The lesions are usually
infections; therefore, influenza and pneumococcal vaccines (>90%) sparing the costophrenic angles.
are recommended. 6. The definite diagnosis of PLCH is based on adequate
In addition, the presence of BRAF V600E mutations and clinical and radiological presentation and the identification
MS RO+ LCH in children was recognized as a factor that of LCs in the examined tissue samples showing in the
negatively influences prognosis (71), but in adults with PLCH, the immunohistochemistry the presence of one of the following
BRAF V600E mutation was not associated with LCH presentation antigens: CD207 (langerin), CD1a.
and outcome (5). 7. Treatment of LCH depends on extension of the disease.
LCH promotes the development of other neoplasms Currently, the preferred cytostatic treatment option
originating from the lymphatic and hematopoietic systems, includes cladribine or cytarabine. Lung transplantation
including LCH overlapping with chronic myelogenous leukemia. is recommended in patients with isolated PLCH with
In a group of 132 adult patients with LCH, Ma et al. (82) found respiratory insufficiency.
that 32% were diagnosed with additional neoplasms, mostly 8. PLCH patients have a lower mean survival than individuals
before [58%] and concurrently (21%) with LCH diagnosis. Lung of the same sex and age. Negative prognostic factors are age,
(18%), breast (18%), and colon (12%) cancers were the most tobacco smoking, severe obstruction, lowered PaO2 , a higher
frequently detected additional neoplasms. score in SGRQ, pulmonary hypertension, and multiple organ
involvement, particularly risk organs.
Pregnancy and Labor AUTHOR CONTRIBUTIONS
Pregnancy does not worsen the course of PLCH, but delivery by
cesarean section is recommended due to the enhanced likelihood The author confirms being the sole contributor of this work and
of pneumothorax (83). has approved it for publication.
REFERENCES 4. Roden AC, Hu X, Kip S, Parrilla Castellar ER, Rumilla KM, Vrana JA,
et al. BRAF V600E expression in langerhans cell histiocytosis: clinical
1. Emile JF, Abla O, Fraitag S, Horne A, Haroche J, Donadieu J. Revised and immunohistochemical study on 25 pulmonary and 54 extrapulmonary
classification of histiocytoses and neoplasms of the macrophage-dendritic cell cases. Am J Surg Pathol. (2014) 38:548–51. doi: 10.1097/PAS.0000000000
lineages. Blood. (2016) 127:2672–81. doi: 10.1182/blood-2016-01-690636 000129
2. Badalian-Very G, Vergilio JA, Degar BA, MacConaill LE, Brandner B, 5. Jouenne F, Chevret S, Bugnet E, Clappier E, Lorillon G,
Calicchio ML, et al. Recurrent BRAF mutations in langerhans cell Meignin V, et al. Genetic landscape of adult Langerhans
histiocytosis. Blood. (2010) 116:1919–23. doi: 10.1182/blood-2010-04-279083 cell histiocytosis with lung involvement. Eur Respir J. (2020)
3. Berres ML, Lim KP, Peters T, Price J, Takizawa H, Salmon H, et al. 55:1901190. doi: 10.1183/13993003.01190-2019
BRAF-V600E expression in precursor versus differentiated dendritic cells 6. Goyal G, Young JR, Koster MJ, Tobin WO, Vassallo R, Ryu JH. The mayo
defines clinically distinct LCH risk groups. J Exp Med. (2014) 211:669– clinic histiocytosis working group consensus statement for the diagnosis
83. doi: 10.1084/jem.20130977 and evaluation of adult patients with histiocytic neoplasms: erdheim-chester
Frontiers in Medicine | www.frontiersin.org 9 March 2021 | Volume 7 | Article 582581
Radzikowska Update on PLCH
disease, langerhans cell histiocytosis, rosai-dorfman disease. Mayo Clinic Proc. 50 cases. Human Pathol. (2016) 52:61–7. doi: 10.1016/j.humpath.201
(2019) 94:2054–71. doi: 10.1016/j.mayocp.2019.02.023 5.12.029
7. Girschikofsky M, Arico M, Castillo D, Chu A, Doberauer C, Fichter J. 26. Mourah S, How-Kit A, Meignin V, Gossot D, Lorillon G, Bugnet E, et al.
et al. Management of adult patients with langerhans cell histiocytosis: Recurrent NRAS mutations in pulmonary Langerhans cell histiocytosis. Eur
recommendations from an expert panel on behalf of Euro-Histio-Net. Respir J. (2016) 47:1785–96. doi: 10.1183/13993003.01677-2015
Orphanet J Rare Dis. (2013) 8:72. doi: 10.1186/1750-1172-8-72 27. Ozer E, Sevinc A, Ince D, Yuzuguldu R, Olgun N. BRAF V600E
8. Aricò M, Girschikofsky M, Généreau T, Klersy C, McClain K, Grois mutation: a significant biomarker for prediction of disease relapse in
N, et al. Langerhans cell histiocytosis in adults. Report from the pediatric langerhans cell histiocytosis. Pediatr Dev Pathol. (2019) 22:449–
International Registry of the Histiocyte Society. Eur J Cancer. (2003) 39:2341– 55. doi: 10.1177/1093526619847859
8. doi: 10.1016/s0959-8049(03)00672-5 28. Rodriguez-Galindo C, Allen CE. Langerhans cell histiocytosis. Blood. (2020)
9. Vassallo R, Ryu JH, Schroeder DR, Decker PA, Limper AH. Clinical outcomes 135:1319–31. doi: 10.1182/blood.2019000934
of pulmonary Langerhans’-cell histiocytosis in adults. N Eng J Med. (2002) 29. Halbritter F, Farlik M, Schwentner R, Jug G, Fortelny N, Schnöller T,
346:484–90. doi: 10.1056/NEJMoa012087 et al. Epigenomics and single-cell sequencing define a developmental
10. Schönfeld N, Dirks K, Costabel U, Loddenkemper R. Wissenschaftliche hierarchy in langerhans cell histiocytosis. Cancer Discovery. (2019) 9:1406–
Arbeitsgemeinschaft für die Therapie von Lungenkrankheiten. A prospective 21. doi: 10.1158/2159-8290.CD-19-0138
clinical multicentre study on adult pulmonary Langerhans’ cell histiocytosis. 30. Haroche J, Cohen-Aubart F, Rollins BJ, Donadieu J, Charlotte F, Idbaih A, et al.
Sarc Vasc Diffuse Lung Dis. (2012) 29:132–8. Available online at: https:// Histiocytoses: emerging neoplasia behind inflammation. Lancet Oncol. (2017)
mattioli1885journals.com/index.php/sarcoidosis/article/view/2508 18:e113–25. doi: 10.1016/S1470-2045(17)30031-1
11. Elia D, Torre O, Cassandro R, Caminati A, Harari S. Pulmonary Langerhans 31. Mendez JL, Nadrous HF, Vassallo R, Decker PA, Ryu JH. Pneumothorax
cell histiocytosis: a comprehensive analysis of 40 patients and literature review. in pulmonary Langerhans cell histiocytosis. Chest. (2004) 125:1028–
Eur J Int Med. (2015) 26:351–6. doi: 10.1016/j.ejim.2015.04.001 32. doi: 10.1378/chest.125.3.1028
12. Picarsic J, Jaffe R. Nosology and pathology of Langerhans cell 32. Heiden GI, Sobral JB, Freitas CSG, Pereira de Albuquerque AL, Salge JM,
histiocytosis. Hematol Oncol Clin North Am. (2015) 29:799– Kairalla RA, et al. Mechanisms of exercise limitation and prevalence of
82. doi: 10.1016/j.hoc.2015.06001 pulmonary hypertension in pulmonary langerhans cell histiocytosis. Chest.
13. Ronceray L, Pötschger U, Janka G, Gadner H, Minkov M, German Society for (2020) 158:2440–8. doi: 10.1016/j.chest.2020.05.609
Pediatric, Hematology, and Oncology, Langerhans Cell Histiocytosis Study, 33. Dauriat G, Mal H, Thabut G, Mornex JF, Bertocchi M, Tronc
Group. Pulmonary involvement in pediatric-onset multisystem langerhans F, et al. Lung transplantation for pulmonary langerhans’ cell
cell histiocytosis: effect on course and outcome. J Pediatr. (2012) 161:129– histiocytosis: a multicenter analysis. Transplantation. (2006)
33.e333. doi: 10.1016/j.jpeds.2011.12.035 81:746–50. doi: 10.1097/01.tp.0000200304.64613.af
14. Le Louet S, Barkaoui MA, Miron J, Galambrun C, Aladjidi N, Chastagner 34. Abbritti M, Mazzei MA, Bargagli E, Refini RM, Penza F, Perari MG,
P, et al. Childhood Langerhans cell histiocytosis with severe lung et al. Utility of spiral CAT scan in the follow-up of patients with
involvement: a nationwide cohort study. Orphanet J Rare Dis. (2020) pulmonary langerhans cell histiocytosis. Eur J Radiol. (2012) 81:1907–
15:241. doi: 10.1186/s13023-020-01495-5 12. doi: 10.1016/j.ejrad.2011.04.018
15. Goyal G, Shah MV, Hook CC, Wolanskyj AP, Call TG, Rech KL. 35. Kim HJ, Lee KS, Johkoh T, Tomiyama N, Lee HY, Han J, et al.
et al. Adult disseminated langerhans cell histiocytosis: incidence, racial Pulmonary Langerhans cell histiocytosis in adults: high-resolution CT-
disparities and long-term outcomes. Br J Haematol. (2018) 182:579– pathology comparisons and evolutional changes at CT. Eur Radiol. (2011)
81. doi: 10.1111/bjh.14818 21:1406–15. doi: 10.1007/s00330-011-2075-9
16. Tazi A, de Margerie C, Naccache JM, Fry S, Dominique S, Jouneau 36. Albano D, Bosio G, Giubbini R, Bertagna F. Role of 18 F-FDG PET/CT
S, et al. The natural history of adult pulmonary langerhans cell in patients affected by Langerhans cell histiocytosis. Jpn J Radiol. (2017)
histiocytosis: a prospective multicentre study. Orphanet J Rare Dis. (2015) 35:574–83. doi: 10.1007/s11604-017-0668-1
10:30. doi: 10.1186/s13023-015-0249-2 37. Obert J, Vercellino L, Van Der Gucht A, de Margerie-Mellon C,
17. Radzikowska E, Błasińska-Przerwa K, Wiatr E, Bestry I, Langfort R, Bugnet E, Chevret S, et al. 18 F-fluorodeoxyglucose positron emission
Roszkowski-Sliz K. Pneumothorax in patients with pulmonary langerhans cell tomography-computed tomography in the management of adult multisystem
histiocytosis. Lung. (2018) 196:715–20. doi: 10.1007/s00408-018-0155-1 Langerhans cell histiocytosis. Eur J Nucl Med Mol Imaging. (2017) 44:598–
18. Le Guen P, Chevret S, Bugnet E, de Margerie-Mellon C, Lorillon G, Seguin- 610. doi: 10.1007/s00259-016-3521-3
Givelet A, et al. Management and outcomes of pneumothorax in adult 38. Tazi A, Marc K, Dominique S, de Bazelaire C, Crestani B, Chinet
patients with langerhans cell histiocytosis. Orphanet J Rare Dis. (2019) T, et al. Serial computed tomography and lung function testing in
14:229. doi: 10.1186/s13023-019-1203-5 pulmonary Langerhans’ cell histiocytosis. Eur Respir J. (2012) 40:905–
19. Wang D, Cui L, Li ZG, Zhang L, Lian HY, Ma HH, et al. Clinical research 12. doi: 10.1183/09031936.00210711
of pulmonary langerhans cell histiocytosis in children. Chinese Med J. (2018) 39. Rolland-Debord C, Fry S, Giovannelli J, Langlois C, Bricout N, Aguilaniu B.
131:1793–8. doi: 10.4103/0366-6999.237400 Physiologic determinants of exercise capacity in pulmonary langerhans
20. Abla O, Rollins B, Ladisch S. Langerhans cell histiocytosis: progress and cell histiocytosis: a multidimensional analysis. PLoS ONE. (2017)
controversies. Br J Haematol. (2019) 187:559–62. doi: 10.1111/bjh.16099 12:e0170035. doi: 10.1371/journal.pone.0170035
21. Liu H, Osterburg AR, Flury J, Swank Z, McGraw DW, Gupta N, 40. Harari S, Torre O, Cassandro R, Taveira-DaSilva AM, Moss J. Bronchoscopic
et al. MAPK mutations and cigarette smoke promote the pathogenesis diagnosis of langerhans cell histiocytosis and lymphangioleiomyomatosis.
of pulmonary langerhans cell histiocytosis. JCI Insight. (2020) Respir Med. (2012) 106:1286–92. doi: 10.1016/j.rmed.2012.06.012
5:e132048. doi: 10.1172/jci.insight.132048 41. Baqir M, Vassallo R, Maldonado F, Yi ES, Ryu JH. Utility of bronchoscopy
22. Murakami I, Matsushita M, Iwasaki T, Kuwamoto S, Kato M, Nagata K, et al. in pulmonary Langerhans cell histiocytosis. J Bronch Intervent Pulm. (2013)
Interleukin-1 loop model for pathogenesis of langerhans cell histiocytosis. Cell 20:309–12. doi: 10.1097/LBR.0000000000000021
Comm Sig. (2015) 13:13. doi: 10.1186/s12964-015-0092-z 42. Fruchter O, Fridel L, El Raouf BA, Abdel-Rahman N, Rosengarten D, Kramer
23. Suri HS, Yi ES, Nowakowski GS, Vassallo R. Pulmonary langerhans cell MR. Histological diagnosis of interstitial lung diseases by cryo-transbronchial
histiocytosis. Orphanet J Rare Dis. (2012) 7:16. doi: 10.1186/1750-1172-7-16 biopsy. Respirology. (2014) 19:683–8. doi: 10.1111/resp.12296
24. Roden AC, Yi ES. Pulmonary langerhans cell histiocytosis: an update 43. Ravaglia C, Bonifazi M, Wells AU, Tomassetti S, Gurioli C, Piciucchi
from the pathologists’ perspective. Arch Pathol Lab Med. (2016) 140:230– S, et al. Safety and diagnostic yield of transbronchial lung cryobiopsy
40. doi: 10.5858/arpa.2015-0246-RA in diffuse parenchymal lung diseases: a comparative study versus video-
25. Alayed K, Medeiros LJ, Patel KP, Zuo Z, Li S, Verma S, et al. BRAF assisted thoracoscopic lung biopsy and a systematic review of the literature.
and MAP2K1 mutations in Langerhans cell histiocytosis: a study of Respiration. (2016) 91:215–27. doi: 10.1159/000444089
Frontiers in Medicine | www.frontiersin.org 10 March 2021 | Volume 7 | Article 582581
Radzikowska Update on PLCH
44. Lommatzsch M, Bratke K, Stoll P, Mülleneisen N, Prall F, Bier A, et al. 63. Adam Z, Szturz P, Vaníček J, Moulis M, Pour L, Krej,čí M, et al. Cladribine
Bronchoalveolar lavage for the diagnosis of pulmonary langerhans cell (2-chlorodeoxyadenosine) in frontline chemotherapy for adult Langerhans
histiocytosis. Respir Med. (2016) 119:168–74. doi: 10.1016/j.rmed.2016.09.004 cell histiocytosis: a single-center study of seven cases. Acta Oncol. (2013)
45. Auerswald U, Barth J, Magnussen H. Value of CD-1-positive cells in 52:994–1001. doi: 10.3109/0284186X.2012.716164
bronchoalveolar lavage fluid for the diagnosis of pulmonary histiocytosis X. 64. Haroche J, Cohen-Aubart F, Emile JF, Arnaud L, Maksud P, Charlotte
Lung. (1991) 169:305–9. doi: 10.1007/BF02714167 F, et al. Dramatic efficacy of vemurafenib in both multisystemic
46. Torre O, Harari S. The diagnosis of cystic lung diseases: a role for and refractory Erdheim-Chester disease and langerhans cell
bronchoalveolar lavage and transbronchial biopsy?. Respir Med. (2010) histiocytosis harboring the BRAF V600E mutation. Blood. (2013)
104(Suppl 1):S81–5. doi: 10.1016/j.rmed.2010.03.021 121:1495–500. doi: 10.1182/blood-2012-07-446286
47. Radzikowska E, Wiatr E, Błasińska-Przerwa K, Jeśkiewicz M, Langfort 65. Donadieu J, Larabi IA, Tardieu M, Visser J, Hutter C, Sieni E, et al.
R, Maksymiuk B, et al. Clinical features and outcome of adult patients Vemurafenib for refractory multisystem langerhans cell histiocytosis in
with pulmonary Langerhans cell histiocytosis. Eur Respir J. (2019) 54:PA children: an international observational study. J Clin Oncol. (2019) 37:2857–
3683. doi: 10.1183/13993003.congress-2019 65. doi: 10.1200/JCO.19.00456
48. Bois MC, May AM, Vassallo R, Jenkins SM, Yi ES, Roden AC. 66. Hazim AZ, Ruan GJ, Ravindran A, Abeykoon JP, Scheckel C, Vassallo R, et al.
Morphometric study of pulmonary arterial changes in pulmonary Efficacy of BRAF-inhibitor therapy in BRAFV600E -mutated adult langerhans
langerhans cell histiocytosis. Arch Pathol Lab Med. (2018) cell histiocytosis. Oncologist. (2020) 25:1001–4. doi: 10.1002/onco.13541
142:929–37. doi: 10.5858/arpa.2017-0463-OA 67. Diamond EL, Subbiah V, Lockhart AC, Blay JY, Puzanov I. Chau,
49. Thierry A, Mouliere F, El Messaoudi S, Mollevi C, Lopez-Crapez E, Rolet et al. Vemurafenib for BRAF V600-mutant erdheim-chester disease and
F, et al. Clinical validation of the detection of KRAS and BRAF mutations langerhans cell histiocytosis: analysis of data from the histology-independent,
from circulating tumor DNA. Nat Med. (2014) 20:430–5. doi: 10.1038/ phase 2, open-label VE-BASKET study. JAMA Oncol. (2018) 4:384–
nm.3511 8. doi: 10.1001/jamaoncol.2017.5029
50. Héritier S, Hélias-Rodzewicz Z, Lapillonne H, Terrones N, Garrigou 68. Bhatia A, Ulaner G, Rampal R, Hyman DM, Abdel-Wahab O, Durham
S, Normand C. Circulating cell-free BRAFV600E as a biomarker in BH, et al. Single-agent dabrafenib for BRAFV600E -mutated histiocytosis.
children with Langerhans cell histiocytosis. Br J Haemat. (2017) 178:457– Haematologica. (2018) 103:e177–80. doi: 10.3324/haematol.2017.1
67. doi: 10.1111/bjh.14695 85298
51. Lorillon G, Tazi A. How i manage pulmonary langerhans cell histiocytosis. Eur 69. Diamond EL, Durham BH, Ulaner GA, Drill E, Buthorn J, Ki M, et al. Efficacy
Respir Rev. (2017) 26:170070. doi: 10.1183/16000617.0070-2017 of MEK inhibition in patients with histiocytic neoplasms. Nature. (2019)
52. Shaw B, Borchers M, Zander D, Gupta N. Pulmonary langerhans 567:521–4. doi: 10.1038/s41586-019-1012-y
cell histiocytosis. Sem Respir Critical Care Med. (2020) 41:269– 70. Hyman DM, Puzanov I, Subbiah V, Faris JE, Chau I, Blay JY, et al.
79. doi: 10.1055/s-0039-1700996 Vemurafenib in multiple nonmelanoma Cancers with BRAF V600 Mutations.
53. Derenzini E, Fina MP, Stefoni V, Pellegrini C, Venturini F, Broccoli N Engl J Med. (2015) 373:726–36. doi: 10.1056/NEJMoa1502309
A. et al. MACOP-B regimen in the treatment of adult Langerhans cell 71. Héritier S, Emile JF, Barkaoui MA, Thomas C, Fraitag S, Boudjemaa S,
histiocytosis: experience on seven patients. Ann Oncol. (2010) 21:1173– et al. BRAF mutation correlates with high-risk langerhans cell histiocytosis
8. doi: 10.1093/annonc/mdp455 and increased resistance to first-line therapy. J Clin Oncol. (2016) 34:3023–
54. Duan MH, Han X, Li J, Zhang W, Zhu TN, Han B, et al. Comparison of 30. doi: 10.1200/JCO.2015.65.9508
vindesine and prednisone and cyclophosphamide, etoposide, vindesine, 72. Lorillon G, Jouenne F, Baroudjian B, de Margerie-Mellon C, Vercellino L,
and prednisone as first-line treatment for adult Langerhans cell Meignin V, et al. Response to trametinib of a pulmonary langerhans cell
histiocytosis: a single-center retrospective study. Leukemia Res. (2016) histiocytosis harboring a MAP2K1 deletion. Am J Respir Crit Care Med. (2018)
42:43–6. doi: 10.1016/j.leukres.2016.01.012 198:675–8. doi: 10.1164/rccm.201802-0275LE
55. Morimoto A, Shimazaki C, Takahashi S, Yoshikawa K, Nishimura R, Wakita 73. Awada G, Seremet T, Fostier K, Everaert H, Neyns B. Long-
H, et al. Therapeutic outcome of multifocal langerhans cell histiocytosis in term disease control of Langerhans cell histiocytosis using
adults treated with the special c regimen formulated by the Japan LCH combined BRAF and MEK inhibition. Blood Adv. (2018)
study group. Int J Hematol. (2013) 97:103–8. doi: 10.1007/s12185-012- 2:2156–8. doi: 10.1182/bloodadvances.201802178
1245-0 74. Montella L, Insabato L, Palmieri G. Imatinib mesylate for
56. Ng Wing Tin S, Martin-Duverneuil N, Idbaih A, Garel C, Ribeiro M, Parker cerebral Langerhans’-cell histiocytosis. NEJM. (2004) 351:1034–
JL, et al. Efficacy of vinblastine in central nervous system Langerhans cell 5. doi: 10.1056/NEJM200409023511022
histiocytosis: a nationwide retrospective study. Orphanet J Rare Dis. (2011) 75. Janku F, Amin HM, Yang D, Garrido-Laguna I, Trent JC, Kurzrock R.
6:83. doi: 10.1186/1750-1172-6-83 Response of histiocytoses to imatinib mesylate: fire to ashes. J Clin Oncol.
57. Tazi A, Lorillon G, Haroche J, Neel A, Dominique S, Aouba A, (2010) 28:e633–e636. doi: 10.1200/JCO.2010.29.9073
et al. Vinblastine chemotherapy in adult patients with langerhans cell 76. Wagner C, Mohme H, Krömer-Olbrisch T, Stadler R, Goerdt S,
histiocytosis: a multicenter retrospective study. Orphanet J Rare Dis. (2017) Kurzen H. Langerhans cell histiocytosis: treatment failure with
12:95. doi: 10.1186/s13023-017-0651-z imatinib. Arch Derm. (2009) 145:949–50. doi: 10.1001/archdermatol.20
58. Cantu MA, Lupo PJ, Bilgi M, Hicks MJ, Allen CE, McClain KL. Optimal 09.164
therapy for adults with langerhans cell histiocytosis bone lesions. PLoS ONE. 77. Gupta N, Langenderfer D, McCormack FX, Schauer DP, Eckman MH. Chest
(2012) 7:e43257. doi: 10.1371/journal.pone.0043257 computed tomographic image screening for cystic lung diseases in patients
59. Néel A, Artifoni M, Fontenoy AM, Tessoulin B, Lorillon G, Cohen-Aubart F, with spontaneous pneumothorax is cost effective. Ann Am Thorac Soc. (2017)
et al. Long-term efficacy and safety of 2CdA (cladribine) in extra-pulmonary 14:17–25. doi: 10.1513/AnnalsATS.201606-459OC
adult-onset Langerhans cell histiocytosis: analysis of 23 cases from the French 78. Le Pavec J, Lorillon G, Jaïs X, Tcherakian C, Feuillet S, Dorfmüller
Histiocytosis Group and systematic literature review. Br J Haemtol. (2020) P, et al. Pulmonary langerhans cell histiocytosis-associated pulmonary
189:869–78. doi: 10.1111/bjh.16449 hypertension: clinical characteristics and impact of pulmonary arterial
60. Saven A, Burian C. Cladribine activity in adult Langerhans-cell histiocytosis. hypertension therapies. Chest. (2012) 142:1150–7. doi: 10.1378/chest.1
Blood. (1999) 93:4125–30. 1-2490
61. Grobost V, Khouatra C, Lazor R, Cordier JF, Cottin V. Effectiveness of 79. May A, Kane G, Yi E, Frantz R, Vassallo R. Dramatic and sustained
cladribine therapy in patients with pulmonary langerhans cell histiocytosis. responsiveness of pulmonary langerhans cell histiocytosis-associated
Orphanet J Rare Dis. (2014) 9:191. doi: 10.1186/s13023-014-0191-8 pulmonary hypertension to vasodilator therapy. Respir Med Case Rep. (2014)
62. Pardanani A, Phyliky RL, Li CY, Tefferi A. 2-Chlorodeoxyadenosine therapy 14:13–5. doi: 10.1016/j.rmcr.2014.11.005
for disseminated Langerhans cell histiocytosis. Mayo Clin Proc. (2003) 78:301– 80. Nemoto K, Oh-Ishi S, Inui T, Nakazawa M, Hyodo K, Nakajima M,
6. doi: 10.4065/78.3.301 et al. Long-term improvement during tadalafil therapy in a patient
Frontiers in Medicine | www.frontiersin.org 11 March 2021 | Volume 7 | Article 582581
Radzikowska Update on PLCH
with pulmonary hypertension secondary to pulmonary langerhans cell 84. Singla A, Kopras EJ, Gupta N. Spontaneous pneumothorax and air travel
histiocytosis. Respir Med Case Rep. (2016) 18:54–7. doi: 10.1016/j.rmcr.201 in pulmonary Langerhans cell histiocytosis: a patient survey. Respir Invest.
6.04.008 (2019) 57:582–9. doi: 10.1016/j.resinv.2019.07.004
81. Wajda N, Zhu Z, Jandarov R, Dilling DF, Gupta N. Clinical
outcomes and survival following lung transplantation in patients Conflict of Interest: The author declares that the research was conducted in the
with pulmonary Langerhans cell histiocytosis. Respirology. (2020) absence of any commercial or financial relationships that could be construed as a
25:644–50. doi: 10.1111/resp.13671 potential conflict of interest.
82. Ma J, Laird JH, Chau KW, Chelius MR, Lok BH, Yahalom J. Langerhans cell
histiocytosis in adults is associated with a high prevalence of hematologic Copyright © 2021 Radzikowska. This is an open-access article distributed under the
and solid malignancies. Cancer Med. (2019) 8:58–66. doi: 10.1002/ca terms of the Creative Commons Attribution License (CC BY). The use, distribution
m4.1844 or reproduction in other forums is permitted, provided the original author(s) and
83. Radzikowska E, Wiatr E, Franczuk M, Bestry I, Roszkowski-Sli,z K. Lung the copyright owner(s) are credited and that the original publication in this journal
function in pregnancy in langerhans cell histiocytosis. Adv Exp Med Biol. is cited, in accordance with accepted academic practice. No use, distribution or
(2018) 1023:73–83. doi: 10.1007/5584_2017_72 reproduction is permitted which does not comply with these terms.
Frontiers in Medicine | www.frontiersin.org 12 March 2021 | Volume 7 | Article 582581
You might also like
- Shaw - Seminars in Respiratory and Critical Care Medicine 2020Document11 pagesShaw - Seminars in Respiratory and Critical Care Medicine 2020rrralexandrescuNo ratings yet
- Histiocytosis and The Nervous System: From Diagnosis To Targeted TherapiesDocument14 pagesHistiocytosis and The Nervous System: From Diagnosis To Targeted TherapiesLuís PachecoNo ratings yet
- Paediatric Pulmonary Langerhans Cell Histiocytosis ReviewDocument9 pagesPaediatric Pulmonary Langerhans Cell Histiocytosis Reviewgiant nitaNo ratings yet
- TaziDocument14 pagesTazirrralexandrescuNo ratings yet
- Langerhans Cell HistiocytosisDocument7 pagesLangerhans Cell HistiocytosisDarwin ElguiraNo ratings yet
- Recent Advances in Langerhans Cell HistiDocument11 pagesRecent Advances in Langerhans Cell HistiThanasis PapatheodorouNo ratings yet
- GHID European HistiocitozaDocument11 pagesGHID European HistiocitozaCarmen IlarieNo ratings yet
- Atypical Cellular Disorders: Kenneth L. Mcclain, Yasodha Natkunam, and Steven H. SwerdlowDocument14 pagesAtypical Cellular Disorders: Kenneth L. Mcclain, Yasodha Natkunam, and Steven H. SwerdlowhemendreNo ratings yet
- JURNALDocument10 pagesJURNALLuses Shantia HaryantoNo ratings yet
- BJR 20160221Document9 pagesBJR 20160221Wulan HachycuiNo ratings yet
- Knaap-Bugiani2017 Article LeukodystrophiesAProposedClassDocument32 pagesKnaap-Bugiani2017 Article LeukodystrophiesAProposedClassNATALIA MARTINEZ CORDOBANo ratings yet
- Immune Mechanisms Linking Metabolic Injury To in Ammation and Fibrosis in Fatty Liver Disease - Novel Insights Into Cellular Communication CircuitsDocument25 pagesImmune Mechanisms Linking Metabolic Injury To in Ammation and Fibrosis in Fatty Liver Disease - Novel Insights Into Cellular Communication Circuitsdr. Nur'aini HasanNo ratings yet
- Fimmu 11 591741Document25 pagesFimmu 11 591741dineshkumaryadav39423No ratings yet
- Langerhans-Cell Histiocytosis: Review ArticleDocument13 pagesLangerhans-Cell Histiocytosis: Review ArticleHanifah ArroziNo ratings yet
- Imun Copd 2019Document12 pagesImun Copd 2019Amilia FrayantyNo ratings yet
- Pulmonary Fibrosis in Sytemic Sclerosis Diagnosis and ManagementDocument5 pagesPulmonary Fibrosis in Sytemic Sclerosis Diagnosis and ManagementAnthoNo ratings yet
- Avances en LESDocument8 pagesAvances en LESFranciscoJoseNo ratings yet
- New Concepts in The Immunopathogenesis of Multiple SclerosisDocument11 pagesNew Concepts in The Immunopathogenesis of Multiple Sclerosisaedes_agNo ratings yet
- Systemic Sclerosis: Michael Hughes, Yannick Allanore, Christopher P. Denton, Marco Matucci-CerinicDocument10 pagesSystemic Sclerosis: Michael Hughes, Yannick Allanore, Christopher P. Denton, Marco Matucci-CerinicJosé Javier Morales NúñezNo ratings yet
- Histiocytic SarcomaDocument8 pagesHistiocytic SarcomadanishNo ratings yet
- Sepsis-Pathophysiology and Therapeutic ConceptsDocument22 pagesSepsis-Pathophysiology and Therapeutic ConceptsJuan ZamoraNo ratings yet
- ANA TestDocument9 pagesANA TestNena_mileyNo ratings yet
- Jurnal EBM A3Document12 pagesJurnal EBM A3koko satriaNo ratings yet
- Microparticulas ArdsDocument18 pagesMicroparticulas ArdsARELHI ROSARIO GARCIA MONROYNo ratings yet
- Pure Vulvar Langerhans Cell Histiocytosis A Case Report and Literature ReviewDocument8 pagesPure Vulvar Langerhans Cell Histiocytosis A Case Report and Literature ReviewqdvtairifNo ratings yet
- Hematologic Changes in SepsisDocument16 pagesHematologic Changes in SepsisnisaNo ratings yet
- A 56 Year Old Woman With Multiple Pulmonary CystsDocument8 pagesA 56 Year Old Woman With Multiple Pulmonary CystsAchmad Dodi MeidiantoNo ratings yet
- Chronic Lymphocytic LeukemiaFrom EverandChronic Lymphocytic LeukemiaMichael HallekNo ratings yet
- Pathogenic Cellular and Molecular Mediators in Lupus NephritisDocument18 pagesPathogenic Cellular and Molecular Mediators in Lupus NephritisYo MeNo ratings yet
- 368 FullDocument10 pages368 FullIrvin MarcelNo ratings yet
- Seminar: Michael Hallek, Tait D Shanafelt, Barbara EichhorstDocument13 pagesSeminar: Michael Hallek, Tait D Shanafelt, Barbara Eichhorstlengers poworNo ratings yet
- manuscript_232Document9 pagesmanuscript_232Shelin AmandaNo ratings yet
- Kikuchi-Fujimoto Disease: Adhikari RCDocument5 pagesKikuchi-Fujimoto Disease: Adhikari RCRam Chandra AdhikariNo ratings yet
- In Ammation and Atherosclerosis: Signaling Pathways and Therapeutic InterventionDocument24 pagesIn Ammation and Atherosclerosis: Signaling Pathways and Therapeutic InterventionZahroNo ratings yet
- Nihms 1813067Document34 pagesNihms 1813067Marlyn SuciningtiasNo ratings yet
- Lupus 1Document9 pagesLupus 1karina hernandezNo ratings yet
- BioFactors - 2023 - Lopes - Erythrocytes Surface Properties and Stiffness Predict Survival and Functional Decline in ALSDocument14 pagesBioFactors - 2023 - Lopes - Erythrocytes Surface Properties and Stiffness Predict Survival and Functional Decline in ALSAna Catarina De Oliveira Da Silv LaborinhoNo ratings yet
- Tumor Cell Interaction with Lymphatic Vessels in Cancer Progression and MetastasisDocument10 pagesTumor Cell Interaction with Lymphatic Vessels in Cancer Progression and MetastasisChetan PatilNo ratings yet
- Langerhans Cell Histiocytosis Literature Review and Descriptive Analysis of Oral ManifestationsDocument4 pagesLangerhans Cell Histiocytosis Literature Review and Descriptive Analysis of Oral ManifestationsafmzamdswsfksxNo ratings yet
- Review: K. Osterbur, F.A. Mann, K. Kuroki, and A. DeclueDocument11 pagesReview: K. Osterbur, F.A. Mann, K. Kuroki, and A. DeclueMill Jan CruzNo ratings yet
- Journal Reading - Progressive Multiple SclerosisDocument20 pagesJournal Reading - Progressive Multiple SclerosisMuhammad Imam NoorNo ratings yet
- Review One Year in Review 2017: Systemic Lupus ErythematosusDocument11 pagesReview One Year in Review 2017: Systemic Lupus ErythematosusAmany RadwanNo ratings yet
- El Glucocalix en La SepsisDocument8 pagesEl Glucocalix en La SepsisAndrea GaytánNo ratings yet
- Chediak-Higashi Syndrome: Jerry Kaplan, Ivana de Domenico and Diane Mcvey WardDocument8 pagesChediak-Higashi Syndrome: Jerry Kaplan, Ivana de Domenico and Diane Mcvey WardMagaly AngelbaeNo ratings yet
- Urowitz 2017Document13 pagesUrowitz 2017Aldo Emir M. SarabiaNo ratings yet
- Laryngeal Involvement in Connective Tissue DisordersDocument8 pagesLaryngeal Involvement in Connective Tissue DisordersIvan DarioNo ratings yet
- Thoracic Involvement in Generalised Lymphatic Anomaly (Or Lymphangiomatosis)Document8 pagesThoracic Involvement in Generalised Lymphatic Anomaly (Or Lymphangiomatosis)Angel FloresNo ratings yet
- Vasculitis LeucocitoclásticaDocument11 pagesVasculitis LeucocitoclásticaLaura Daniela MurilloNo ratings yet
- Gupta Part 2Document13 pagesGupta Part 2rrralexandrescuNo ratings yet
- Pulmonary Hypertension Advances in Pathogenesis and TreatmentDocument12 pagesPulmonary Hypertension Advances in Pathogenesis and Treatmentbdalcin5512No ratings yet
- ALS - The Complex Path To Precision MedicineDocument9 pagesALS - The Complex Path To Precision MedicineAurelia Sartika TongkuNo ratings yet
- Role of liver sinusoidal endothelial cells in non-alcoholic fatty liver diseaseDocument14 pagesRole of liver sinusoidal endothelial cells in non-alcoholic fatty liver diseaseHainner Steven Huaman BacilioNo ratings yet
- Bookshelf NBK553857Document12 pagesBookshelf NBK553857Sanda Škrinjarić-CincarNo ratings yet
- ICU Rounds: Pulmonary Leukostasis as a Complication of LeukemiaDocument6 pagesICU Rounds: Pulmonary Leukostasis as a Complication of LeukemiaPratita Jati PermatasariNo ratings yet
- Baluk2008 PDFDocument12 pagesBaluk2008 PDFBidisha ChakrabortyNo ratings yet
- Xanthomas: Clinical and Pathophysiological RelationsDocument9 pagesXanthomas: Clinical and Pathophysiological RelationsAurora Zaldivar GamboaNo ratings yet
- Author: Section Editor: Deputy Editor:: Pathogenesis of Systemic Sclerosis (Scleroderma)Document24 pagesAuthor: Section Editor: Deputy Editor:: Pathogenesis of Systemic Sclerosis (Scleroderma)zakiNo ratings yet
- Mecanismo Inmune en La HTADocument10 pagesMecanismo Inmune en La HTAClau TomNo ratings yet
- Lancet-Leucemia Linfocitica CronicaDocument14 pagesLancet-Leucemia Linfocitica CronicaMr. LNo ratings yet
- Kidney Involvement in Systemic Sclerosis JUL 2022Document15 pagesKidney Involvement in Systemic Sclerosis JUL 2022Diego Ignacio González MárquezNo ratings yet
- Accessory Breasts: A Historical PerspectiveDocument4 pagesAccessory Breasts: A Historical Perspectivegiant nitaNo ratings yet
- Breast 8Document5 pagesBreast 8giant nitaNo ratings yet
- Heterogeneous Imaging Features of Aspergillosis at F FDG Pet/CtDocument11 pagesHeterogeneous Imaging Features of Aspergillosis at F FDG Pet/Ctgiant nitaNo ratings yet
- Breast 2Document10 pagesBreast 2giant nitaNo ratings yet
- Breast 1Document2 pagesBreast 1giant nitaNo ratings yet
- Breast 11Document5 pagesBreast 11giant nitaNo ratings yet
- BCR 2015 210918Document3 pagesBCR 2015 210918giant nitaNo ratings yet
- Breast 10Document12 pagesBreast 10giant nitaNo ratings yet
- Imaging Features of Extrapulmonary Tuberculosis in ChildrenDocument9 pagesImaging Features of Extrapulmonary Tuberculosis in Childrengiant nitaNo ratings yet
- Transplantology 02 00011Document9 pagesTransplantology 02 00011giant nitaNo ratings yet
- AspergillosisDocument12 pagesAspergillosisgiant nitaNo ratings yet
- Central Nervous System TuberculosisDocument16 pagesCentral Nervous System TuberculosisntnquynhproNo ratings yet
- Blaser 2015Document12 pagesBlaser 2015giant nitaNo ratings yet
- GTN 3Document12 pagesGTN 3giant nitaNo ratings yet
- Imaging Lung Manifestations HIV/AIDSDocument17 pagesImaging Lung Manifestations HIV/AIDSgiant nitaNo ratings yet
- Ali 2Document7 pagesAli 2giant nitaNo ratings yet
- DD Osteogenesis ImperfectaDocument5 pagesDD Osteogenesis Imperfectagiant nitaNo ratings yet
- GTN 6Document13 pagesGTN 6giant nitaNo ratings yet
- Paediatric TB Treatment LandscapeDocument11 pagesPaediatric TB Treatment Landscapegiant nitaNo ratings yet
- Narita 2014Document1 pageNarita 2014giant nitaNo ratings yet
- Radiographic Features of Osteogenesis ImperfectaDocument14 pagesRadiographic Features of Osteogenesis Imperfectafakhriyyatur rahmi mNo ratings yet
- Gestational Trophoblastic Disease Current.22Document16 pagesGestational Trophoblastic Disease Current.22nando8396100% (1)
- LCH 1Document8 pagesLCH 1giant nitaNo ratings yet
- Breast Sutton 1Document9 pagesBreast Sutton 1giant nitaNo ratings yet
- LCH 2Document10 pagesLCH 2giant nitaNo ratings yet
- Cranium 3Document26 pagesCranium 3giant nitaNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument11 pagesBest Practice & Research Clinical Obstetrics and GynaecologyMetharisaNo ratings yet
- Referensi CTDocument1 pageReferensi CTgiant nitaNo ratings yet
- Realiability of Digital Micromirror Device Final VersionDocument13 pagesRealiability of Digital Micromirror Device Final VersionRaj MistryNo ratings yet
- Pityriasis Versicolor: Avoiding Pitfalls in Disease Diagnosis and TherapyDocument3 pagesPityriasis Versicolor: Avoiding Pitfalls in Disease Diagnosis and TherapypanduNo ratings yet
- Risk Management Framework and ProcessDocument16 pagesRisk Management Framework and ProcessIuliana T.No ratings yet
- Brown Creative Vintage Rustic Motivational Quote PosterDocument1 pageBrown Creative Vintage Rustic Motivational Quote PosterRafunzel Pe BandoquilloNo ratings yet
- Investigation Into Failure Phenomena of Water Meter in The Kingdom of BahrainDocument118 pagesInvestigation Into Failure Phenomena of Water Meter in The Kingdom of BahrainJabnon NonjabNo ratings yet
- Hospital Ship Feasibility StudyDocument10 pagesHospital Ship Feasibility StudyRhona JhoyNo ratings yet
- Evangelion Cruel Angels Thesis - Moonbase AlphaDocument5 pagesEvangelion Cruel Angels Thesis - Moonbase Alphasionothewil1977100% (1)
- 1994 - Non Wood Plant Fibre - Literarture Review - US - fplgtr80 PDFDocument148 pages1994 - Non Wood Plant Fibre - Literarture Review - US - fplgtr80 PDFSrinivas AyyalasomayajulaNo ratings yet
- Guía BaccettiDocument11 pagesGuía BaccettiPercy Andree Bayona GuillermoNo ratings yet
- The Nazi Master PlanDocument28 pagesThe Nazi Master PlanFolad109No ratings yet
- 10th Magnetic Effects of Currents MCQ-1Document1 page10th Magnetic Effects of Currents MCQ-1jots2100% (1)
- United States Court of Appeals, Fourth CircuitDocument4 pagesUnited States Court of Appeals, Fourth CircuitScribd Government DocsNo ratings yet
- Iep2014 15Document22 pagesIep2014 15api-245317729No ratings yet
- Personal Development PlanDocument10 pagesPersonal Development PlanNg Thị Kh ThiệnNo ratings yet
- Cse ReviewerDocument23 pagesCse ReviewerJerome Jumalon AlayonNo ratings yet
- Dokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFDocument2 pagesDokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFPayal SethiNo ratings yet
- Mama and Mommy and Me in The Middle Press ReleaseDocument2 pagesMama and Mommy and Me in The Middle Press ReleaseCandlewick Press0% (1)
- Moon Landing ConspiracyDocument17 pagesMoon Landing ConspiracyElianeSalamNo ratings yet
- Emerald Emerging Markets Case Studies: Article InformationDocument25 pagesEmerald Emerging Markets Case Studies: Article InformationHannah CastroNo ratings yet
- Handout 2Document3 pagesHandout 2Cale CynthiaNo ratings yet
- Prediction of Hospital Admission Using Machine LearningDocument9 pagesPrediction of Hospital Admission Using Machine LearningTRIAD TECHNO SERVICESNo ratings yet
- OTC 17236 The New API RP 2A, 22 Edition Tubular Joint Design PracticeDocument0 pagesOTC 17236 The New API RP 2A, 22 Edition Tubular Joint Design PracticeKrutarth Purohit0% (1)
- Income Tax and GST PDFDocument152 pagesIncome Tax and GST PDFAdharsh EsNo ratings yet
- Anthony Andreas Vass, Barbara Harrison Social Work Competences Core Knowledge, Values and SkillsDocument248 pagesAnthony Andreas Vass, Barbara Harrison Social Work Competences Core Knowledge, Values and SkillsAhmad Syifa100% (2)
- Using ABAQUS to Reduce Tire Belt Edge StressesDocument10 pagesUsing ABAQUS to Reduce Tire Belt Edge StressesGautam SharmaNo ratings yet
- Environmental Sustainability Assessment of An Academic Institution in Calamba CityDocument29 pagesEnvironmental Sustainability Assessment of An Academic Institution in Calamba CityAmadeus Fernando M. PagenteNo ratings yet
- Customer Preferences For Restaurant Technology InnovationsDocument22 pagesCustomer Preferences For Restaurant Technology InnovationsDeepankar SinghNo ratings yet
- Selection of Hazard Evaluation Techniques PDFDocument16 pagesSelection of Hazard Evaluation Techniques PDFdediodedNo ratings yet
- Operations Management Service ExcellenceDocument18 pagesOperations Management Service ExcellenceParth PatelNo ratings yet
- How Film Elements Build TensionDocument2 pagesHow Film Elements Build TensionBangga ErizalNo ratings yet