You might also like
- C15 Engine: Electrical Circuit DiagramDocument12 pagesC15 Engine: Electrical Circuit DiagramPhil B.100% (1)
- 4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaDocument6 pages4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaProfesseur Christian DumontierNo ratings yet
- Marriage Issues-1Document21 pagesMarriage Issues-1Edward100% (1)
- The Final War by Judge Rutherford, 1932Document65 pagesThe Final War by Judge Rutherford, 1932sirjsslutNo ratings yet
- PHYSICS Engineering (BTech/BE) 1st First Year Notes, Books, Ebook - Free PDF DownloadDocument205 pagesPHYSICS Engineering (BTech/BE) 1st First Year Notes, Books, Ebook - Free PDF DownloadVinnie Singh100% (2)
- Inspected by QCP Approval 1-APC 1 - APC 2 - DAR 2 - DAR Al-Handeseh 3 - Negemco 4 - Vendor 5 - Third PartyDocument4 pagesInspected by QCP Approval 1-APC 1 - APC 2 - DAR 2 - DAR Al-Handeseh 3 - Negemco 4 - Vendor 5 - Third PartyAhmad DagamsehNo ratings yet
- 200+ TOP RADIOLOGY Online Quiz Questions - Exam Test 2023Document24 pages200+ TOP RADIOLOGY Online Quiz Questions - Exam Test 2023Ayub Alam100% (1)
- Synthesis Paper On Nuclear PPDocument3 pagesSynthesis Paper On Nuclear PPchristinekehyengNo ratings yet
- Outcomes Following LCL ReconstructionDocument7 pagesOutcomes Following LCL ReconstructionRaeni Dwi PutriNo ratings yet
- Nomura 2005 - Anatomical Analysis of The Medial Patellofemoral Ligament of The Knee, Especially The Femoral AttachmentDocument6 pagesNomura 2005 - Anatomical Analysis of The Medial Patellofemoral Ligament of The Knee, Especially The Femoral AttachmentThiago Sanchez Pires BuenoNo ratings yet
- Sener 2017Document9 pagesSener 2017Zachary DuongNo ratings yet
- Art3a10 10072fs00256-014-1842-5Document9 pagesArt3a10 10072fs00256-014-1842-5api-253958760No ratings yet
- Relation in SemiDocument8 pagesRelation in SemiLuisNo ratings yet
- Reoperation Rates After Fenestration For Lumbar Spinal Canal Stenosis: A 20-Year Period Survival Function Method AnalysisDocument7 pagesReoperation Rates After Fenestration For Lumbar Spinal Canal Stenosis: A 20-Year Period Survival Function Method AnalysisYusuf BrilliantNo ratings yet
- 1 s2.0 S1743919106600538 Main PDFDocument3 pages1 s2.0 S1743919106600538 Main PDFTarun MathurNo ratings yet
- Schottle 2007Document4 pagesSchottle 2007Lugh LugoNo ratings yet
- Anatomy of CF Lig. 2020Document5 pagesAnatomy of CF Lig. 2020Ahmed MortadaNo ratings yet
- Anatomy of IER Review 2016Document6 pagesAnatomy of IER Review 2016Ahmed MortadaNo ratings yet
- Magnetic Resonance Imagination of The Peroneus Longus Tendon After Anterior Cruciate Ligament ReconstructionDocument5 pagesMagnetic Resonance Imagination of The Peroneus Longus Tendon After Anterior Cruciate Ligament Reconstructionfebyan yohanesNo ratings yet
- OSRM ProximalDocument9 pagesOSRM ProximalÂngelo Rosso LlantadaNo ratings yet
- Lee 2021 2Document10 pagesLee 2021 2Aaron BNo ratings yet
- Kee MRI PDFDocument17 pagesKee MRI PDFNoura RoseNo ratings yet
- Pi Is 0363502317302241Document5 pagesPi Is 0363502317302241ashik MohamedNo ratings yet
- Kim Technique MCL and POLDocument5 pagesKim Technique MCL and POLManuel Vergillos LunaNo ratings yet
- Quantitative and Qualitative Assessment of Posterolateral Meniscal AnatomyDocument7 pagesQuantitative and Qualitative Assessment of Posterolateral Meniscal AnatomyNuno AlimanNo ratings yet
- Rosenbrg-Goss2020 Article AModifiedTechniqueOfTemporomanDocument10 pagesRosenbrg-Goss2020 Article AModifiedTechniqueOfTemporomanMarcela RibeiroNo ratings yet
- 2021 - Chronic Isolated Radial Head DislocationDocument9 pages2021 - Chronic Isolated Radial Head Dislocationjuan pablo aguirreNo ratings yet
- Acute Posterior Cruciate Ligament Injuries: Effect of Location, Severity, and Associated Injuries On Surgical ManagementDocument10 pagesAcute Posterior Cruciate Ligament Injuries: Effect of Location, Severity, and Associated Injuries On Surgical Managementshabrina nurafiatiNo ratings yet
- Radiograph StifleDocument9 pagesRadiograph Stifleandrea marigoNo ratings yet
- Medial Elbow Anatomy A Paradigm Shift For UCL Injury Prevention and ManagementDocument11 pagesMedial Elbow Anatomy A Paradigm Shift For UCL Injury Prevention and ManagementAlberto GallariniNo ratings yet
- Realignment Surgery For Malunited Ankle Fracture: Clinical ArticleDocument5 pagesRealignment Surgery For Malunited Ankle Fracture: Clinical ArticleGio VandaNo ratings yet
- Infleunce of Group Function Canine Guidance On Elevator MuscleDocument8 pagesInfleunce of Group Function Canine Guidance On Elevator MuscleHossam BarghashNo ratings yet
- Lateral Uka Survivorship Short To MidtermDocument5 pagesLateral Uka Survivorship Short To Midtermapi-267962692No ratings yet
- (MRI) Medial Patellar LigamentsDocument11 pages(MRI) Medial Patellar LigamentsyNo ratings yet
- Management of Injuries To The Medial PatellofemoralDocument9 pagesManagement of Injuries To The Medial Patellofemorallite.trawler-0xNo ratings yet
- P ('t':'3', 'I':'669333659') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document6 pagesP ('t':'3', 'I':'669333659') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)deadcorpsesNo ratings yet
- 167 2016 Article 4272Document18 pages167 2016 Article 4272asmaNo ratings yet
- The Anterolateral Complex of The Knee: A Pictorial EssayDocument6 pagesThe Anterolateral Complex of The Knee: A Pictorial EssayLISETTE TRICIA MALIPERONo ratings yet
- Intramedullary Control of Distal Femoral Resection Results in Precise Coronal Alignment in TKADocument7 pagesIntramedullary Control of Distal Femoral Resection Results in Precise Coronal Alignment in TKAAsmed El SalugNo ratings yet
- The Distance of The Gluteal Nerve in Relation To Anatomical LandmarksDocument7 pagesThe Distance of The Gluteal Nerve in Relation To Anatomical LandmarksValentín ThomasNo ratings yet
- Acl Recon With BPT GraftDocument6 pagesAcl Recon With BPT Graftpaper coe medanNo ratings yet
- Stabilization of Distal Humerus Fractures by Precontoured Bi-Condylar Plating in A 90-90 PatternDocument5 pagesStabilization of Distal Humerus Fractures by Precontoured Bi-Condylar Plating in A 90-90 PatternmayNo ratings yet
- Comparison of The Modified Transtibial Technique, Anteromedial Portal Technique and Outside-In Technique in ACL ReconstructionDocument8 pagesComparison of The Modified Transtibial Technique, Anteromedial Portal Technique and Outside-In Technique in ACL ReconstructionJahid HasanNo ratings yet
- Artigo ClamshellDocument15 pagesArtigo ClamshellbritocirurgiadamaoNo ratings yet
- Joa0208 0309 PDFDocument8 pagesJoa0208 0309 PDFSanditya FadliNo ratings yet
- 4 in 1 Quadricepsplasty For Fixed and Habitual DisDocument8 pages4 in 1 Quadricepsplasty For Fixed and Habitual DisMinh ChíNo ratings yet
- Anatomy Biomechanics Lateral Side Knee Surgical ImplicationsDocument8 pagesAnatomy Biomechanics Lateral Side Knee Surgical ImplicationsFasilNigusseNo ratings yet
- 26 Ijss Mar Oa26 - 2019Document5 pages26 Ijss Mar Oa26 - 2019Ravikiran NandirajuNo ratings yet
- Treatment of Condylar Fractures With An Intraoral ApproachDocument26 pagesTreatment of Condylar Fractures With An Intraoral Approachdhiraj.2367No ratings yet
- 3 PBDocument8 pages3 PBfabian hernandez medinaNo ratings yet
- BODPUODocument8 pagesBODPUOMiguel AradaNo ratings yet
- 1999 AhnDocument7 pages1999 Ahnosama-alaliNo ratings yet
- Fitmore Hip StemDocument3 pagesFitmore Hip StemCarmen IulianaNo ratings yet
- 5099 Extraordinary MeridiansDocument7 pages5099 Extraordinary MeridiansitayNo ratings yet
- Art:10.1186/1756 0500 7 569Document6 pagesArt:10.1186/1756 0500 7 569Fuioaga Codrin-PaulNo ratings yet
- Changes in The Loading of Tibial Articular Cartilage Following Medial Meniscectomy: A Finite Element Analysis StudyDocument7 pagesChanges in The Loading of Tibial Articular Cartilage Following Medial Meniscectomy: A Finite Element Analysis StudylenbertiNo ratings yet
- 264 2010 Article 1052Document6 pages264 2010 Article 1052thisisangieNo ratings yet
- Anatomic Posterolateral Corner ReconstructionDocument10 pagesAnatomic Posterolateral Corner Reconstructionethan.dumontNo ratings yet
- #PENTING Bell1983Document7 pages#PENTING Bell1983Octapaedi SoetomoNo ratings yet
- MPFL Rehab ProtocolDocument18 pagesMPFL Rehab ProtocolharyskawdNo ratings yet
- Tecnica LapradeDocument5 pagesTecnica LapradeThiagoNo ratings yet
- Quantitative and Descriptive Analysis of The Meniscotibial Ligament in Human CorpsesDocument3 pagesQuantitative and Descriptive Analysis of The Meniscotibial Ligament in Human CorpsesSaifuddin HaswareNo ratings yet
- Iwanaga 2017Document5 pagesIwanaga 2017zj7n2rhtb4No ratings yet
- Liu 2019Document7 pagesLiu 2019Aulia Siti NuraininNo ratings yet
- Assessment of The Anterior Talofibular Ligament Thickness 2017 Journal of MeDocument5 pagesAssessment of The Anterior Talofibular Ligament Thickness 2017 Journal of MeRyana Fitriana IINo ratings yet
- 2016 Article 9341 PDFDocument8 pages2016 Article 9341 PDFJulenda CintarinovaNo ratings yet
- Dislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementFrom EverandDislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementNigel Shaun MatthewsNo ratings yet
- Rohini 24928786475Document12 pagesRohini 24928786475aswinvirat84No ratings yet
- Statement of Purpose For Studying MechatronicsDocument2 pagesStatement of Purpose For Studying MechatronicsBivash NiroulaNo ratings yet
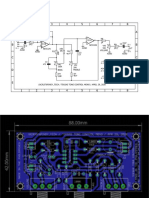
- Teksas Tone Control MonoDocument17 pagesTeksas Tone Control MonoRhenz TalhaNo ratings yet
- Symbolism and Color in Folk ArtDocument11 pagesSymbolism and Color in Folk ArtshandryssNo ratings yet
- Honey Python TestingDocument2 pagesHoney Python Testinger.honeyraj2016No ratings yet
- A 234 - A 234M - 17 PDFDocument9 pagesA 234 - A 234M - 17 PDFأسامة وحيد الدين رمضانNo ratings yet
- ENGR 260 - Circuits and Devices: COURSE SYLLABUS - Spring 2015Document4 pagesENGR 260 - Circuits and Devices: COURSE SYLLABUS - Spring 2015saintNo ratings yet
- Martinal LEO - Product RangeDocument6 pagesMartinal LEO - Product RangeAdamMitchellNo ratings yet
- Attachment - Statement HP 2023 January Cyan, Magenta, Yellow, and BlackDocument2 pagesAttachment - Statement HP 2023 January Cyan, Magenta, Yellow, and BlackWayan PartaNo ratings yet
- Gec-Tcw Prelims GlobalizationDocument4 pagesGec-Tcw Prelims GlobalizationClarynce MojadoNo ratings yet
- RFL Week 1 DinnersDocument10 pagesRFL Week 1 DinnersMorris TruckingNo ratings yet
- Paddy SeedsDocument8 pagesPaddy SeedsgvrnaiduNo ratings yet
- Simple Clean Minimalist Ancient Egypt History Class Presentation A4 Lands - 20231116 - 143549 - 0000Document9 pagesSimple Clean Minimalist Ancient Egypt History Class Presentation A4 Lands - 20231116 - 143549 - 0000carlajanebaribaraleriaNo ratings yet
- Dee Mandala InfoMemoDocument27 pagesDee Mandala InfoMemoSheetalkumarNo ratings yet
- Moonshot Beer Summary of Rec 2Document4 pagesMoonshot Beer Summary of Rec 2Hassan AhmadNo ratings yet
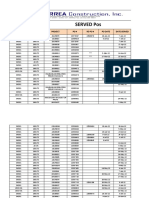
- Served POsDocument21 pagesServed POsYay DumaliNo ratings yet
- Chapter - I (Electrical Safety)Document30 pagesChapter - I (Electrical Safety)Hunter HarshaNo ratings yet
- Lecture 7 Rock ExcavationDocument24 pagesLecture 7 Rock ExcavationMoiz Ahmed KapadiaNo ratings yet
- Mimaki CJV-150 PDFDocument146 pagesMimaki CJV-150 PDFKisgyörgy ZoltánNo ratings yet
- Cambridge Assessment International Education: Geography 0460/12 October/November 2019Document19 pagesCambridge Assessment International Education: Geography 0460/12 October/November 2019Miguel Oubiña SánchezNo ratings yet
- Caritas vs. Avarice: The Embroiled Church and Empire: John Michael PotvinDocument16 pagesCaritas vs. Avarice: The Embroiled Church and Empire: John Michael PotvinJohn PotvinNo ratings yet
- Transformation of Coordinates PDFDocument2 pagesTransformation of Coordinates PDFMa Ella Mae LogronioNo ratings yet
- Abstract CV: Maharani Retna Duhita, M.SC.,PHD - Med.ScDocument39 pagesAbstract CV: Maharani Retna Duhita, M.SC.,PHD - Med.ScnanaNo ratings yet