You might also like
- The Preservation RhinoplastyDocument3 pagesThe Preservation RhinoplastyEvy Larousse33% (3)
- Georgia Habitats Lesson PlansDocument5 pagesGeorgia Habitats Lesson PlansBecky BrownNo ratings yet
- Zombieworld PlaytestDocument30 pagesZombieworld PlaytestWellameGranaNo ratings yet
- Heat Sink Capacity Mesurment in Inservice PipelineDocument13 pagesHeat Sink Capacity Mesurment in Inservice PipelineSomeshNo ratings yet
- 2019 Three Simple Steps For Refining Transcutaneous Lower Blepharoplasty For Aging EyelidsDocument15 pages2019 Three Simple Steps For Refining Transcutaneous Lower Blepharoplasty For Aging EyelidsDimitris RodriguezNo ratings yet
- Use of A Long Arm Gooseneck Smartphone Holder Optimizes Intraoperative PhotographyDocument6 pagesUse of A Long Arm Gooseneck Smartphone Holder Optimizes Intraoperative PhotographySushovan SahaNo ratings yet
- New Uses of Abobotulinumtoxina in AestheticsDocument14 pagesNew Uses of Abobotulinumtoxina in AestheticsJoãoNo ratings yet
- 2016 Report Mortality Fat GraftingDocument11 pages2016 Report Mortality Fat GraftingAntonio CardenasNo ratings yet
- Cerebral Embolism As A Result of Facial Filler Injections - A Literature ReviewDocument14 pagesCerebral Embolism As A Result of Facial Filler Injections - A Literature ReviewKerlida SantosNo ratings yet
- A New Device For Autologous Small Volume-CompressedDocument9 pagesA New Device For Autologous Small Volume-CompressedKikin RizkynnisaNo ratings yet
- Jurnal Mixed Method 2Document12 pagesJurnal Mixed Method 2RobertoNo ratings yet
- Osteosarcoma of The Jaw Classification Diagnosis A PDFDocument26 pagesOsteosarcoma of The Jaw Classification Diagnosis A PDFfirmansyahddsNo ratings yet
- IntJOrthodRehabil84129-8600318 022320Document8 pagesIntJOrthodRehabil84129-8600318 022320denizNo ratings yet
- Sjad 173Document28 pagesSjad 173cocooakNo ratings yet
- Canula+versos+agulha+em+cada Ver+2Document16 pagesCanula+versos+agulha+em+cada Ver+2raquelhxNo ratings yet
- Mediating Role of Body Mass Index in Knee Osteoarthritis: February 2017Document8 pagesMediating Role of Body Mass Index in Knee Osteoarthritis: February 2017Fatimatus Zahroh IchsanNo ratings yet
- Subcision IndicationsadversereactionsandpearlsDocument11 pagesSubcision Indicationsadversereactionsandpearls郭先薈No ratings yet
- Open Vs Closed VIP2Document11 pagesOpen Vs Closed VIP2Ahmad FareedNo ratings yet
- A Simple Technique To Measure The Volume of Removed Buccal FatDocument3 pagesA Simple Technique To Measure The Volume of Removed Buccal FatGuilherme GuerraNo ratings yet
- LL ALLUZIENCE Liquid Formulation of AbobotulinumtoxinA A 6-MonthDocument13 pagesLL ALLUZIENCE Liquid Formulation of AbobotulinumtoxinA A 6-MonthAnderson GomesNo ratings yet
- 1 s2.0 S1361841516300342 MainDocument17 pages1 s2.0 S1361841516300342 Mainzhujin1121No ratings yet
- Anexo 3Document15 pagesAnexo 3Bianca LongoNo ratings yet
- Regenerative Cells For Facial Surgery: Biofilling and BiocontouringDocument17 pagesRegenerative Cells For Facial Surgery: Biofilling and BiocontouringKTNo ratings yet
- Filler Rhinoplasty: Evidence, Outcomes, and ComplicationsDocument3 pagesFiller Rhinoplasty: Evidence, Outcomes, and ComplicationsАндрей ПетровNo ratings yet
- 1 4916194771602506025Document11 pages1 4916194771602506025Juliana BrunettoNo ratings yet
- Document 2Document10 pagesDocument 2iblNo ratings yet
- Gox 3 E291Document12 pagesGox 3 E291fer.bpjnNo ratings yet
- Implante Articulo 2Document5 pagesImplante Articulo 2alessandrachumbimuneNo ratings yet
- Jurnal New Mpkrs Luar NegriDocument12 pagesJurnal New Mpkrs Luar NegridiahNo ratings yet
- CriolipolizaDocument11 pagesCriolipolizaroxanaNo ratings yet
- Sjab 070Document11 pagesSjab 070Hải Dương MinhNo ratings yet
- A Systematic Review and Meta-Analysis of Hernia Sac Management in Laparoscopic Groin Hernia Mesh Repair: Reduction or Transection?Document11 pagesA Systematic Review and Meta-Analysis of Hernia Sac Management in Laparoscopic Groin Hernia Mesh Repair: Reduction or Transection?Andric Perez-OrtizNo ratings yet
- Dorsal Preservation The Push Down Technique ReasseDocument16 pagesDorsal Preservation The Push Down Technique Reassediego suescunNo ratings yet
- Double LayerCarotidStentWissgott2015Document7 pagesDouble LayerCarotidStentWissgott2015Nick NgoNo ratings yet
- Sjab 116Document8 pagesSjab 116Poramate PITAK-ARNNOPNo ratings yet
- The Preservation Rhinoplasty: A New Rhinoplasty RevolutionDocument2 pagesThe Preservation Rhinoplasty: A New Rhinoplasty RevolutionEdwin Barazorda VillegasNo ratings yet
- A New Suturing Method For Optimal Wound Healing: Technique and ExperienceDocument9 pagesA New Suturing Method For Optimal Wound Healing: Technique and Experiencenur safaatul lailaNo ratings yet
- International Wound Journal - 2022 - Lai - Research Trends On Platelet Rich Plasma in The Treatment of Wounds During 2002Document11 pagesInternational Wound Journal - 2022 - Lai - Research Trends On Platelet Rich Plasma in The Treatment of Wounds During 2002imedd science dataNo ratings yet
- Pan AsianconsensusDocument13 pagesPan AsianconsensusaldaNo ratings yet
- Hemostatic AgentsDocument18 pagesHemostatic AgentshariNo ratings yet
- Surgical Drains. What The Resident Needs To KnowDocument8 pagesSurgical Drains. What The Resident Needs To Knowginoahnna33No ratings yet
- Levy Myers 2016 Advancements in Next Generation SequencingDocument23 pagesLevy Myers 2016 Advancements in Next Generation SequencingCallum BirdNo ratings yet
- SJZ 050Document11 pagesSJZ 050vanessa_werbickyNo ratings yet
- Cryolipolysis: Clinical Best Practices and Other Nonclinical ConsiderationsDocument11 pagesCryolipolysis: Clinical Best Practices and Other Nonclinical ConsiderationsPriscilla MacedoNo ratings yet
- In Situ Forming Hydrogels Based On Chitosan ForDocument11 pagesIn Situ Forming Hydrogels Based On Chitosan ForЕгор ЛетовNo ratings yet
- Subcision For Atrophic Acne Scarring A Comprehensive Review of Surgical Instruments and Combinatorial TreatmentsDocument11 pagesSubcision For Atrophic Acne Scarring A Comprehensive Review of Surgical Instruments and Combinatorial TreatmentshilderhNo ratings yet
- Treatment Effectiveness of Frankel Function RegulaDocument13 pagesTreatment Effectiveness of Frankel Function RegulaSilvia Marcela RojasNo ratings yet
- Indirect Composite Restorations Luted With Two Different Procedures: A Ten Years Follow Up Clinical TrialDocument7 pagesIndirect Composite Restorations Luted With Two Different Procedures: A Ten Years Follow Up Clinical TrialAndre Setiawan HalimNo ratings yet
- Surgical Drains What The Resident Needs To KnowDocument8 pagesSurgical Drains What The Resident Needs To Knowshaimaa shehabNo ratings yet
- High Definition Body Sculpting ArtDocument2 pagesHigh Definition Body Sculpting ArtmdwilliamsNo ratings yet
- Canthopexy Evaluation - Anny SubillagaDocument2 pagesCanthopexy Evaluation - Anny SubillagaAnny SubillagaNo ratings yet
- Chappuisetal 2017JDRDocument10 pagesChappuisetal 2017JDRxiaoxin zhangNo ratings yet
- Iej 09 127Document5 pagesIej 09 127Mona AwadNo ratings yet
- Centenoetal 2018 PDFDocument12 pagesCentenoetal 2018 PDFAbcdefNo ratings yet
- A Systematic Review On The Effect of Mechanical Stretch On Hypertrophic Scars After Burn InjuriesDocument9 pagesA Systematic Review On The Effect of Mechanical Stretch On Hypertrophic Scars After Burn Injuriesrizk86No ratings yet
- Annals of SurgeryDocument12 pagesAnnals of SurgeryNada GhammemNo ratings yet
- The Umbilical Benz Incision For Reduced Port Surgery in Pediatric PatientsDocument6 pagesThe Umbilical Benz Incision For Reduced Port Surgery in Pediatric PatientsMarcelo BarberoNo ratings yet
- A PEG-Based Hydrogel For Effective Wound Care ManaDocument10 pagesA PEG-Based Hydrogel For Effective Wound Care ManaThe Music PortalNo ratings yet
- Structure Rhinoplasty Vol.3Document948 pagesStructure Rhinoplasty Vol.3drtechnoNo ratings yet
- JAnaesthClinPharmacol35529-6780889 185008Document7 pagesJAnaesthClinPharmacol35529-6780889 185008Yoga WibowoNo ratings yet
- Kan Et Al-2018-Periodontology 2000Document17 pagesKan Et Al-2018-Periodontology 2000Van nguyen hongNo ratings yet
- Two Years' Outcome of Thread Lifting With Absorbable Barbed PDO Threads: Innovative Score For Objective and Subjective AssessmentDocument11 pagesTwo Years' Outcome of Thread Lifting With Absorbable Barbed PDO Threads: Innovative Score For Objective and Subjective AssessmentMichele CarvalhoNo ratings yet
- Anatomy of The Middle Temporal Vein: Implications For Skull-Base and Craniofacial Reconstruction Using Free FlapsDocument10 pagesAnatomy of The Middle Temporal Vein: Implications For Skull-Base and Craniofacial Reconstruction Using Free FlapsPhạm Nhật HoàngNo ratings yet
- Novel Anatomical Proposal For Botulinum NeurotoxinDocument9 pagesNovel Anatomical Proposal For Botulinum NeurotoxinPhạm Nhật HoàngNo ratings yet
- Thần kinhDocument8 pagesThần kinhPhạm Nhật HoàngNo ratings yet
- Tập huâns dinh dưỡng lâm sàngDocument71 pagesTập huâns dinh dưỡng lâm sàngPhạm Nhật HoàngNo ratings yet
- Liposuction HandbookDocument16 pagesLiposuction HandbookPhạm Nhật HoàngNo ratings yet
- Scientific Approaches For Impurity Profiling in New Pharmaceutical Substances and Its Products-An OverviewDocument18 pagesScientific Approaches For Impurity Profiling in New Pharmaceutical Substances and Its Products-An OverviewsrichainuluNo ratings yet
- Datasheet - 74LS283 - Somador Binário Completo de 4 BitsDocument7 pagesDatasheet - 74LS283 - Somador Binário Completo de 4 BitsLucas CarvalhoNo ratings yet
- Brewers Pallette PosterDocument1 pageBrewers Pallette PosterAnonymous hP6ab2D1ppNo ratings yet
- Algebra I m5 Topic B Lesson 6 TeacherDocument13 pagesAlgebra I m5 Topic B Lesson 6 TeacherjxhroyNo ratings yet
- Baremos Sexual Desire Inventory MEN WomenDocument1 pageBaremos Sexual Desire Inventory MEN WomenGabriNo ratings yet
- Moors Sovereign Dollarium 500 Gold Backed Dollarium PicautoDocument2 pagesMoors Sovereign Dollarium 500 Gold Backed Dollarium Picautoakil kemnebi easley elNo ratings yet
- 2b. TESDA-OP-CO-01-F14 TOOLSDocument2 pages2b. TESDA-OP-CO-01-F14 TOOLSRommel SelgaNo ratings yet
- Class XL (The Portrait of A Lady)Document7 pagesClass XL (The Portrait of A Lady)tmoNo ratings yet
- Soal DescriptiveDocument4 pagesSoal DescriptiveLuh SetiawatiNo ratings yet
- Industrial Training Sample Report of Last YearDocument42 pagesIndustrial Training Sample Report of Last YearKetan NikamNo ratings yet
- GFB V2 - VNT Boost Controller: (Part # 3009)Document2 pagesGFB V2 - VNT Boost Controller: (Part # 3009)blumng100% (1)
- Stresses in Large Horizontal Cylindrical Pressure Vessels On Two Saddle Supports - Zick (1951) OriginalDocument11 pagesStresses in Large Horizontal Cylindrical Pressure Vessels On Two Saddle Supports - Zick (1951) OriginalBryan Pérez PérezNo ratings yet
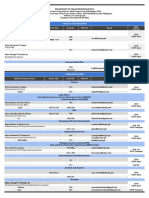
- Updated DOTr Directory As of 29 October 2021Document9 pagesUpdated DOTr Directory As of 29 October 2021Twinkle MiguelNo ratings yet
- Design and Modeling of Zvs Resonantsepic Converter For High FrequencyapplicationsDocument8 pagesDesign and Modeling of Zvs Resonantsepic Converter For High FrequencyapplicationsMohamed WarkzizNo ratings yet
- Idioms & PhrasesDocument4 pagesIdioms & PhrasesHimadri Prosad RoyNo ratings yet
- Língua Inglesa: Reported SpeechDocument3 pagesLíngua Inglesa: Reported SpeechPatrick AlmeidaNo ratings yet
- ISKRA Letak MC3xx 2016 Ver.4.0 2016.compressedDocument6 pagesISKRA Letak MC3xx 2016 Ver.4.0 2016.compressedmelanitisNo ratings yet
- Reglas Digitales Mitutoyo Scale Units Linear ScalesDocument31 pagesReglas Digitales Mitutoyo Scale Units Linear ScalesAngelmambrinNo ratings yet
- Polynesian MigrationsDocument2 pagesPolynesian Migrationskinneyjeffrey100% (1)
- CSCI101 - Lab08 - Functions Zewail CityDocument4 pagesCSCI101 - Lab08 - Functions Zewail CityMahmoud Ahmed 202201238No ratings yet
- Writing Good PI ObjectivesDocument42 pagesWriting Good PI Objectivesfrankiepaul06No ratings yet
- Thin Film DepositionDocument34 pagesThin Film Depositionsenthil100% (2)
- RfI SB Listening ScriptsDocument18 pagesRfI SB Listening ScriptsKate PolissyaNo ratings yet
- Le - 2 Sep. 2019: Reçuclt/Cih/IthDocument18 pagesLe - 2 Sep. 2019: Reçuclt/Cih/IthAlero ViteNo ratings yet
- 100 IC CircuitsDocument34 pages100 IC CircuitselektrorwbNo ratings yet
- Distance Relay BasicsDocument58 pagesDistance Relay Basicsaalamz93_854917254100% (1)
- Ste FannyDocument17 pagesSte FannyElmer DE LA CruzNo ratings yet