You might also like
- Ethics Unit 2Document22 pagesEthics Unit 2SaniNo ratings yet
- Renal Nutrition and Diet in Kidney DiseaseDocument20 pagesRenal Nutrition and Diet in Kidney DiseaseWinnie AriolaNo ratings yet
- Nursing ResearchDocument21 pagesNursing ResearchMargareth SaquibalNo ratings yet
- Patient Self-Determination Act ReportDocument14 pagesPatient Self-Determination Act ReportDaniel RamirezNo ratings yet
- Generating Evidence For Clinical Nursing Practice PDFDocument39 pagesGenerating Evidence For Clinical Nursing Practice PDFTamanna VermaNo ratings yet
- Medicolegal NSGDocument45 pagesMedicolegal NSGIvy Nelly100% (1)
- Chapter 3 Equal Employment Opportunity - pptx1Document22 pagesChapter 3 Equal Employment Opportunity - pptx1Amir ContrerasNo ratings yet
- Nursing Care Management For A Patient With Schizophrenia and Generalized AnxietyDocument23 pagesNursing Care Management For A Patient With Schizophrenia and Generalized AnxietyKimberly Ann BoricanoNo ratings yet
- Research Proposal - (Monisha-20D1977)Document13 pagesResearch Proposal - (Monisha-20D1977)Moni 47No ratings yet
- Unit - VIII Communication and Utilization of Research Utilization of ResearchDocument21 pagesUnit - VIII Communication and Utilization of Research Utilization of ResearchSanchita MandalNo ratings yet
- Impact of Child Labor in The Society-Group 1.editedDocument4 pagesImpact of Child Labor in The Society-Group 1.editedRAEJEHL TIMCANGNo ratings yet
- Good Ethics and Moral Standing - A Qualitative Study of Aesthetic Leadership by Mannix M - Wilkes L - Daly J PDFDocument9 pagesGood Ethics and Moral Standing - A Qualitative Study of Aesthetic Leadership by Mannix M - Wilkes L - Daly J PDFJenny FernandezNo ratings yet
- Module 2 - Dynamics of The Aging ProcessDocument111 pagesModule 2 - Dynamics of The Aging ProcessAYTONA, JAMAICA F.No ratings yet
- Topic+3 Health+Sector+2023Document54 pagesTopic+3 Health+Sector+2023Fedelyn Mae Acaylar100% (1)
- Concept of Health DiseaseDocument73 pagesConcept of Health Diseaseshruti pachare100% (1)
- RetrieveDocument9 pagesRetrievebinabazighNo ratings yet
- To Severe Dementia in Long-Term CareDocument14 pagesTo Severe Dementia in Long-Term Care2gether fanmeet100% (1)
- Collaborative CareDocument16 pagesCollaborative CareArdhani IrfanNo ratings yet
- Referral Systems For HEWDocument39 pagesReferral Systems For HEWmohammed AminNo ratings yet
- Leadership: Chapter 3 - Skills ApproachDocument22 pagesLeadership: Chapter 3 - Skills ApproachHoussame NaimNo ratings yet
- Magnetic Resonance Imaging (Mri) : Submitted By: Vasvi Tomar Mba-Ha Iind SemesterDocument17 pagesMagnetic Resonance Imaging (Mri) : Submitted By: Vasvi Tomar Mba-Ha Iind SemesterVasviNo ratings yet
- 2 - Health Care Politics in Nursing...Document18 pages2 - Health Care Politics in Nursing...فيصل الاعرجNo ratings yet
- The Role of Nursing Homes in ACOsDocument4 pagesThe Role of Nursing Homes in ACOsrjg427No ratings yet
- Sam PDFDocument134 pagesSam PDFPunit Garg100% (2)
- Latest Document 1-1Document63 pagesLatest Document 1-1ijojo elizabethNo ratings yet
- Nchwa Hrsa Nursing ReportDocument22 pagesNchwa Hrsa Nursing ReportTarandam INo ratings yet
- 7 AHM Antibiotic PolicyDocument98 pages7 AHM Antibiotic PolicyfaisalNo ratings yet
- Eoc ManualDocument57 pagesEoc ManualAngelo Russel LazagaNo ratings yet
- 3.02 Medical Ethics Trans - Introduction To BioethicsDocument4 pages3.02 Medical Ethics Trans - Introduction To BioethicsRaquel ReyesNo ratings yet
- Ubc 2015 November Abizadeh JasminDocument200 pagesUbc 2015 November Abizadeh JasminJomer GonzalesNo ratings yet
- Professional ResponsibilityDocument2 pagesProfessional ResponsibilityAnnapurna DangetiNo ratings yet
- Legal, Ethical NursingDocument43 pagesLegal, Ethical NursingKwadwo AsareNo ratings yet
- Mental Health ActDocument20 pagesMental Health ActBiswas AruNo ratings yet
- HASTING CENTER The Privacy Rule That's NotDocument11 pagesHASTING CENTER The Privacy Rule That's NotIon Arrieta ValeroNo ratings yet
- Training Report On Regenerative Health and Nutrition For Nutriion OfficersDocument7 pagesTraining Report On Regenerative Health and Nutrition For Nutriion OfficersibnmamaniNo ratings yet
- Arba Minch Univerity College of Medicine and Health Sciences Department of Public HealthDocument56 pagesArba Minch Univerity College of Medicine and Health Sciences Department of Public HealthDibora AlemayehuNo ratings yet
- ProfessionalDocument55 pagesProfessionalrubycorazon_edizaNo ratings yet
- 3Document232 pages3Dipeshwari ThakreNo ratings yet
- IGNOU Block 1 Unit 6 Bio-Medical Waste Management & Infection ControlDocument20 pagesIGNOU Block 1 Unit 6 Bio-Medical Waste Management & Infection Controlerice.researchNo ratings yet
- Autonomy Vs BeneficenceDocument2 pagesAutonomy Vs Beneficencedr fikriNo ratings yet
- Cervicalpolyp 12345Document14 pagesCervicalpolyp 12345faikaoesmaniaNo ratings yet
- Human Rights in Healthcare IndustryDocument25 pagesHuman Rights in Healthcare IndustryNICKY SAMBONo ratings yet
- Research Study Tool Phototherapy enDocument25 pagesResearch Study Tool Phototherapy encarlos100% (1)
- EthicsDocument48 pagesEthicsTadesse Fenta100% (1)
- Better Outcomes: A Guide To Humanizing HealthcareDocument35 pagesBetter Outcomes: A Guide To Humanizing HealthcareCharlene KronstedtNo ratings yet
- Primary Health Care As An Approach To HealthDocument31 pagesPrimary Health Care As An Approach To HealthRea Andrea CuaresmaNo ratings yet
- Ethical GuidelinesDocument120 pagesEthical GuidelinesKunal PalNo ratings yet
- A Is Emergency CodeDocument7 pagesA Is Emergency CodeAkansha SharmaNo ratings yet
- The Code of Ethics For Registered Nurses in The PhilippinesDocument6 pagesThe Code of Ethics For Registered Nurses in The PhilippinesDarla SaulerNo ratings yet
- Design That Uses Ai To Overturn Stereotypes: Make Witches Wicked AgainDocument12 pagesDesign That Uses Ai To Overturn Stereotypes: Make Witches Wicked AgainAdam HansenNo ratings yet
- WHO WB Quality Health Services-EngDocument100 pagesWHO WB Quality Health Services-EngsofiabloemNo ratings yet
- Schizophrenia Patient GuideDocument14 pagesSchizophrenia Patient GuideDragutin PetrićNo ratings yet
- Ethics: 3 Descriptions of What Ethics Is All AboutDocument37 pagesEthics: 3 Descriptions of What Ethics Is All AboutRoseann FeleciaNo ratings yet
- Procedure On TracheostomyDocument14 pagesProcedure On Tracheostomymohamad dildarNo ratings yet
- Nursing Care Plan GuideDocument1 pageNursing Care Plan GuideTracy100% (1)
- Health Maintenance and Public HealthDocument72 pagesHealth Maintenance and Public HealthAhmad MakhloufNo ratings yet
- Perioperative Nursing ManualDocument101 pagesPerioperative Nursing ManualGabrielle MagdaraogNo ratings yet
- NURS 12 - ReviewerDocument8 pagesNURS 12 - ReviewerRina Lyzea PunongbayanNo ratings yet
- Elderly Services in Health CentersDocument73 pagesElderly Services in Health CentersHsk MiaoNo ratings yet
- The Evolution, Expansion, and Effectiveness of Community Health WorkersDocument24 pagesThe Evolution, Expansion, and Effectiveness of Community Health WorkersSHYRENE KAYE ALLADONo ratings yet
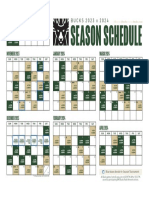
- The Bucks' 2023-24 Regular Season Schedule Is HereDocument1 pageThe Bucks' 2023-24 Regular Season Schedule Is HereAly ProutyNo ratings yet
- K-12 Referenda Passage Rates FallDocument4 pagesK-12 Referenda Passage Rates FallAly ProutyNo ratings yet
- 2023 ALICE ReportDocument30 pages2023 ALICE ReportAly ProutyNo ratings yet
- 2022.07.08 DKT 35 Redacted Amended ComplaintDocument168 pages2022.07.08 DKT 35 Redacted Amended ComplaintAly ProutyNo ratings yet
- Wisconsin Policy Forum: Higher Education Funding Stabilizes Overall, But Enrollment Still FallingDocument5 pagesWisconsin Policy Forum: Higher Education Funding Stabilizes Overall, But Enrollment Still FallingAly ProutyNo ratings yet
- Microsoft Fact Sheet March 28 2023Document1 pageMicrosoft Fact Sheet March 28 2023Aly ProutyNo ratings yet
- Wisconsin Poison Center's 2022 Annual ReportDocument5 pagesWisconsin Poison Center's 2022 Annual ReportAly ProutyNo ratings yet
- Violent Crime Plan Spring 2023Document45 pagesViolent Crime Plan Spring 2023TMJ4 NewsNo ratings yet
- More Schools Turn To Short-Term LicensesDocument4 pagesMore Schools Turn To Short-Term LicensesAly ProutyNo ratings yet
- Alzheimer's Facts and Figures 2023Document132 pagesAlzheimer's Facts and Figures 2023Aly ProutyNo ratings yet
- 3-3-23 REEC Appointees - 202303031318449812Document2 pages3-3-23 REEC Appointees - 202303031318449812Aly ProutyNo ratings yet
- 3-7-23 Racial and Ethnic Equity Commission ApplicationsDocument1 page3-7-23 Racial and Ethnic Equity Commission ApplicationsAly ProutyNo ratings yet
- Annual Report 2022: Meeting Our Most Important NeedsDocument36 pagesAnnual Report 2022: Meeting Our Most Important NeedsAly ProutyNo ratings yet
- BuiltToLast FullReportDocument42 pagesBuiltToLast FullReportAly ProutyNo ratings yet
- Wisconsin Office of Children's Mental Health 2022 Annual ReportDocument20 pagesWisconsin Office of Children's Mental Health 2022 Annual ReportTMJ4 NewsNo ratings yet
- Preeti Verma ColgDocument1 pagePreeti Verma ColgAbhinav PandeyNo ratings yet
- Present Sri C.RANGANNA, M.A, B.L., Project OfficerDocument21 pagesPresent Sri C.RANGANNA, M.A, B.L., Project Officermahesh babuNo ratings yet
- H2SDocument26 pagesH2SSameem Qaiser100% (1)
- Distilled Waters TestimonialsDocument219 pagesDistilled Waters TestimonialsBashu Poudel100% (1)
- Case Study: EMR SystemDocument1 pageCase Study: EMR SystemNikhil SatavNo ratings yet
- Test Questions CA1Document3 pagesTest Questions CA1Gemery Jade ArtatesNo ratings yet
- TASS Prevention: CIS Self-Study Lesson PlanDocument5 pagesTASS Prevention: CIS Self-Study Lesson Planjerimiah_manzonNo ratings yet
- All You Need To Know About Clips: AckermannDocument9 pagesAll You Need To Know About Clips: AckermannjulzcatNo ratings yet
- Checklist For Review of Floor Plans Level 1Document5 pagesChecklist For Review of Floor Plans Level 1jherica baltazarNo ratings yet
- Disaster ManagementDocument38 pagesDisaster ManagementIntan RensiskaNo ratings yet
- WACS Radiology Training Accredited CentresDocument8 pagesWACS Radiology Training Accredited CentresAnonymous 9QxPDp100% (1)
- 2.home Based Palliative Care2-Dr. Hendri Pangestu, SpAn KICDocument18 pages2.home Based Palliative Care2-Dr. Hendri Pangestu, SpAn KICRuki HartawanNo ratings yet
- PaediatricTuina Elisa RossiDocument7 pagesPaediatricTuina Elisa Rossideemoney3100% (1)
- Hemodialysis Access 2017Document359 pagesHemodialysis Access 2017Eddie Muñoz100% (1)
- 3 - Taping Technique ProtocolDocument65 pages3 - Taping Technique ProtocolAlexis Nacionales AguinaldoNo ratings yet
- Module 4 Nursing ProcessDocument14 pagesModule 4 Nursing ProcessArjay Cuh-ingNo ratings yet
- Internal Environemntal Analysis and Competitive Advantage: Minakshi Gautam Assistant Professor IIHMR, DelhiDocument52 pagesInternal Environemntal Analysis and Competitive Advantage: Minakshi Gautam Assistant Professor IIHMR, DelhiDrnuzhat FatemaNo ratings yet
- Public Letter To Gov. Cuomo From DOJDocument2 pagesPublic Letter To Gov. Cuomo From DOJJeffrey DunetzNo ratings yet
- Soal Sepsis 0807 Blok7Document2 pagesSoal Sepsis 0807 Blok7Suryadi VOoNo ratings yet
- Firefly Phototherapy BrochureDocument6 pagesFirefly Phototherapy BrochurePhạm ThịnhNo ratings yet
- Second Serious Case Overview Report Relating To Peter Connelly Dated March 2009Document74 pagesSecond Serious Case Overview Report Relating To Peter Connelly Dated March 2009Beverly TranNo ratings yet
- Naskah Health TeachingDocument5 pagesNaskah Health Teachingsukma asriNo ratings yet
- Reaction Paper Ferry DisasterDocument1 pageReaction Paper Ferry DisastermegastupefyNo ratings yet
- Procedure For Reimbursement CasesDocument3 pagesProcedure For Reimbursement CasesImtiazNo ratings yet
- Kel 5 Roleplay Diabetes MellitusDocument4 pagesKel 5 Roleplay Diabetes MellitusDesma LindaNo ratings yet
- Corpus Tasks Achievement Test 3 (Units 9-12) : How Have You Made A Difference?Document2 pagesCorpus Tasks Achievement Test 3 (Units 9-12) : How Have You Made A Difference?Luis Gerardo PérezNo ratings yet
- Departure 5Document8 pagesDeparture 5Donela Joy AbellanoNo ratings yet
- Economies of Scale in HealthDocument22 pagesEconomies of Scale in HealthRavia SharmaNo ratings yet
- Our Lady of Lourdes V CapanzanaDocument18 pagesOur Lady of Lourdes V CapanzanaSteph RubiNo ratings yet
- SR Epic Optime Consultant in USA Resume Linda MandersDocument3 pagesSR Epic Optime Consultant in USA Resume Linda MandersLindaManders2No ratings yet
- The Meth Lunches: Food and Longing in an American CityFrom EverandThe Meth Lunches: Food and Longing in an American CityRating: 5 out of 5 stars5/5 (5)
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfFrom EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfRating: 5 out of 5 stars5/5 (36)
- Workin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherFrom EverandWorkin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherNo ratings yet
- High-Risers: Cabrini-Green and the Fate of American Public HousingFrom EverandHigh-Risers: Cabrini-Green and the Fate of American Public HousingNo ratings yet
- The Great Displacement: Climate Change and the Next American MigrationFrom EverandThe Great Displacement: Climate Change and the Next American MigrationRating: 4.5 out of 5 stars4.5/5 (32)
- Heartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthFrom EverandHeartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthRating: 4 out of 5 stars4/5 (269)
- Hillbilly Elegy: A Memoir of a Family and Culture in CrisisFrom EverandHillbilly Elegy: A Memoir of a Family and Culture in CrisisRating: 4 out of 5 stars4/5 (4284)
- Poor Economics: A Radical Rethinking of the Way to Fight Global PovertyFrom EverandPoor Economics: A Radical Rethinking of the Way to Fight Global PovertyRating: 4.5 out of 5 stars4.5/5 (263)
- Same Kind of Different As Me Movie Edition: A Modern-Day Slave, an International Art Dealer, and the Unlikely Woman Who Bound Them TogetherFrom EverandSame Kind of Different As Me Movie Edition: A Modern-Day Slave, an International Art Dealer, and the Unlikely Woman Who Bound Them TogetherRating: 4 out of 5 stars4/5 (686)
- Heartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthFrom EverandHeartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthRating: 4 out of 5 stars4/5 (188)
- Nickel and Dimed: On (Not) Getting By in AmericaFrom EverandNickel and Dimed: On (Not) Getting By in AmericaRating: 4 out of 5 stars4/5 (186)
- The Mole People: Life in the Tunnels Beneath New York CityFrom EverandThe Mole People: Life in the Tunnels Beneath New York CityRating: 3.5 out of 5 stars3.5/5 (190)
- Nickel and Dimed: On (Not) Getting By in AmericaFrom EverandNickel and Dimed: On (Not) Getting By in AmericaRating: 3.5 out of 5 stars3.5/5 (197)
- Fucked at Birth: Recalibrating the American Dream for the 2020sFrom EverandFucked at Birth: Recalibrating the American Dream for the 2020sRating: 4 out of 5 stars4/5 (173)
- Life at the Bottom: The Worldview That Makes the UnderclassFrom EverandLife at the Bottom: The Worldview That Makes the UnderclassRating: 5 out of 5 stars5/5 (30)
- Who Really Owns Ireland: How we became tenants in our own land - and what we can do about itFrom EverandWho Really Owns Ireland: How we became tenants in our own land - and what we can do about itNo ratings yet
- Not a Crime to Be Poor: The Criminalization of Poverty in AmericaFrom EverandNot a Crime to Be Poor: The Criminalization of Poverty in AmericaRating: 4.5 out of 5 stars4.5/5 (37)
- Out of the Red: My Life of Gangs, Prison, and RedemptionFrom EverandOut of the Red: My Life of Gangs, Prison, and RedemptionNo ratings yet
- This Is Ohio: The Overdose Crisis and the Front Lines of a New AmericaFrom EverandThis Is Ohio: The Overdose Crisis and the Front Lines of a New AmericaRating: 4 out of 5 stars4/5 (37)
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfFrom EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfRating: 4 out of 5 stars4/5 (126)
- How the Poor Can Save Capitalism: Rebuilding the Path to the Middle ClassFrom EverandHow the Poor Can Save Capitalism: Rebuilding the Path to the Middle ClassRating: 5 out of 5 stars5/5 (6)
- Superclass: The Global Power Elite and the World They Are MakingFrom EverandSuperclass: The Global Power Elite and the World They Are MakingRating: 3.5 out of 5 stars3.5/5 (33)
- The Great Displacement: Climate Change and the Next American MigrationFrom EverandThe Great Displacement: Climate Change and the Next American MigrationRating: 4 out of 5 stars4/5 (19)
- Skimmed: Breastfeeding, Race, and InjusticeFrom EverandSkimmed: Breastfeeding, Race, and InjusticeRating: 5 out of 5 stars5/5 (1)