You might also like
- Update On Management of The Oral and Maxillofacial Surgery Patient On CorticosteroidsDocument12 pagesUpdate On Management of The Oral and Maxillofacial Surgery Patient On Corticosteroidsconstanza gormazNo ratings yet
- 58-2Document12 pages58-2NOUF ALDHALAANNo ratings yet
- 01 - 007 Corticosteroids in DentistryDocument3 pages01 - 007 Corticosteroids in DentistryplsssssNo ratings yet
- Adrenal JamaDocument5 pagesAdrenal JamadrsmritiNo ratings yet
- Perioperative Glucocorticoid ManagementDocument8 pagesPerioperative Glucocorticoid ManagementjuanpbagurNo ratings yet
- Adrenal Crisis - StatPearls - NCBI BookshelfDocument9 pagesAdrenal Crisis - StatPearls - NCBI BookshelfDhany karubuyNo ratings yet
- Atow 470 00Document7 pagesAtow 470 00rogelio cruzNo ratings yet
- Congenital Adrenal HyperplasiaDocument29 pagesCongenital Adrenal HyperplasiaMohan RaoNo ratings yet
- Perioperative Corticosteroid Administration: Adel M. Bassily-Marcus, MD - Andrew B. Leibowitz, MDDocument6 pagesPerioperative Corticosteroid Administration: Adel M. Bassily-Marcus, MD - Andrew B. Leibowitz, MDEka NovitasariNo ratings yet
- And Prevention of Thrombosis, 9th Ed: Antiplatelet Drugs: Antithrombotic TherapyDocument33 pagesAnd Prevention of Thrombosis, 9th Ed: Antiplatelet Drugs: Antithrombotic TherapyNube AzulNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptIgo MouraNo ratings yet
- Corticosteroids and Associated DiseasesDocument76 pagesCorticosteroids and Associated DiseasesALNAKINo ratings yet
- Dermatology: RoundsDocument6 pagesDermatology: RoundsPin Wijaya100% (1)
- Role of "Old" Pharmacological Agents in The Treatment of Cushing's SyndromeDocument9 pagesRole of "Old" Pharmacological Agents in The Treatment of Cushing's SyndromeErnesto Castañeda VargasNo ratings yet
- Congenital Adrenal Hyperplasia New Biomarkers and Adult TreatmentsDocument9 pagesCongenital Adrenal Hyperplasia New Biomarkers and Adult Treatmentsmiguel saba sabaNo ratings yet
- Antiplatelet DrugsDocument33 pagesAntiplatelet Drugsxander trujilloNo ratings yet
- Safety of Medications in Pediatric EndocrinologyDocument12 pagesSafety of Medications in Pediatric EndocrinologyandreNo ratings yet
- Methyl PrednisoloneDocument4 pagesMethyl PrednisoloneAnjar WijayadiNo ratings yet
- Week 5 Endokrin WO - Michael GeraldilDocument5 pagesWeek 5 Endokrin WO - Michael GeraldilMichael GNo ratings yet
- Stress Dose SteroidsDocument4 pagesStress Dose SteroidsTitien fitria sholihati100% (1)
- Approach To Patient With Glucocorticoid Induced Adrenal InsufficiencyDocument11 pagesApproach To Patient With Glucocorticoid Induced Adrenal InsufficiencyBHUENDOCRINE SRNo ratings yet
- Cushing TH 4Document13 pagesCushing TH 4syaymaNo ratings yet
- Pharmacology of Adrenocorticoids and Adrenocorticotropic AntagonistsDocument32 pagesPharmacology of Adrenocorticoids and Adrenocorticotropic AntagonistsJoyce VillanuevaNo ratings yet
- 655 FullDocument16 pages655 FullGhina nurulNo ratings yet
- Anti Platelet Drugs Accp 8th EdDocument37 pagesAnti Platelet Drugs Accp 8th EdmelvinpasayNo ratings yet
- Stuvia 3626880 Dental Management of the Medically Compromised Patient-56-69Document14 pagesStuvia 3626880 Dental Management of the Medically Compromised Patient-56-69hassan JwnsNo ratings yet
- Adrenal Senior 1Document12 pagesAdrenal Senior 1mohammad saifuddinNo ratings yet
- Corticosteroid Physiology and Principles of Therapy PDFDocument6 pagesCorticosteroid Physiology and Principles of Therapy PDFTriawan AdinataNo ratings yet
- New Drugs ArtritisDocument13 pagesNew Drugs ArtritisqfecrespoNo ratings yet
- Hipertension Secundaria Drogas y ToxinasDocument8 pagesHipertension Secundaria Drogas y ToxinasResti SyafitriNo ratings yet
- 6 - Predisposing Factors For Adrenal InsufficiencyDocument12 pages6 - Predisposing Factors For Adrenal InsufficiencyAlejandra RNo ratings yet
- Tanpa JudulDocument14 pagesTanpa JudulAsrapia HubaisyingNo ratings yet
- Side Effects of NSAIDsDocument8 pagesSide Effects of NSAIDsAlmas PrawotoNo ratings yet
- Systemic and Local Applications of Steroids in Endodontics: An Update ReviewDocument8 pagesSystemic and Local Applications of Steroids in Endodontics: An Update ReviewJorge OrbeNo ratings yet
- Ketoconazole in Cushing’s syndrome - Abrupt stopDocument10 pagesKetoconazole in Cushing’s syndrome - Abrupt stopadrew1086No ratings yet
- Corticosteroid Adverse Effects - StatPearls - NCBI BookshelfDocument12 pagesCorticosteroid Adverse Effects - StatPearls - NCBI Bookshelfantonio.mastrangelo.999No ratings yet
- Antithrombotic Drugs: Pharmacology and Implications For Dental PracticeDocument9 pagesAntithrombotic Drugs: Pharmacology and Implications For Dental PracticeMariana VLedezmaNo ratings yet
- Adrenocortical AgentsDocument14 pagesAdrenocortical AgentsFredie O HadjimudinNo ratings yet
- Perioperative Stress Response To Surgery and AnesthesiaDocument15 pagesPerioperative Stress Response To Surgery and AnesthesiaMalik IbrahimNo ratings yet
- Diagnosis and Management of Adrenal InsufficiencyDocument11 pagesDiagnosis and Management of Adrenal Insufficiencyinterna MANADONo ratings yet
- How to Safely Stop Glucocorticoid TherapyDocument5 pagesHow to Safely Stop Glucocorticoid TherapysimonchikNo ratings yet
- Hormonal Therapies in Septic Shock: Review ArticleDocument8 pagesHormonal Therapies in Septic Shock: Review ArticleJhon3xNo ratings yet
- Taking The Wrong Medication of Digoxin TabletsDocument3 pagesTaking The Wrong Medication of Digoxin TabletsMarfu'ah Mar'ahNo ratings yet
- FSR Physicians Protocol1Document32 pagesFSR Physicians Protocol1Nishtha SinghalNo ratings yet
- Síndrome de Cushing. Maybe Not So Uncommon of An Endocrine DiseaseDocument10 pagesSíndrome de Cushing. Maybe Not So Uncommon of An Endocrine DiseaseStephany Gutiérrez VargasNo ratings yet
- 6.28.10 Barnes Adrenal InsufficiencyDocument19 pages6.28.10 Barnes Adrenal InsufficiencySami OmerNo ratings yet
- Treatment of Acute GoutDocument38 pagesTreatment of Acute GoutAnoop PkNo ratings yet
- Gupisone 2Document9 pagesGupisone 2ahibba.03862No ratings yet
- Prescribed Drugs and Neurological Complications: K A Grosset, D G GrossetDocument7 pagesPrescribed Drugs and Neurological Complications: K A Grosset, D G GrossetdentsavvyNo ratings yet
- Adrenocortical AgentsDocument8 pagesAdrenocortical AgentsKarina Madriaga100% (1)
- USPI - Med Guide - Feldene - Piroxicam - CapsulesDocument15 pagesUSPI - Med Guide - Feldene - Piroxicam - CapsulesDini FarhatunnabilahNo ratings yet
- PIIS1053077018310437Document5 pagesPIIS1053077018310437andi rahmatNo ratings yet
- Role of Steroids in Critical Care PDFDocument3 pagesRole of Steroids in Critical Care PDFDr.Shilpa JohnNo ratings yet
- New Glucocorticoid FormulationDocument18 pagesNew Glucocorticoid FormulationAko KareemNo ratings yet
- Clinical Review: Controversies in Corticosteroid Use For SepsisDocument9 pagesClinical Review: Controversies in Corticosteroid Use For SepsisDesy ApridiantyNo ratings yet
- Deflazacort Training Manual OverviewDocument10 pagesDeflazacort Training Manual Overviewanupdr_cNo ratings yet
- Anticoagulation Guidelines JMDocument32 pagesAnticoagulation Guidelines JMMichael HuntNo ratings yet
- Prescribing Review July Sept 08 NSAIDsDocument7 pagesPrescribing Review July Sept 08 NSAIDsSonia RogersNo ratings yet
- Adrenal Insufficiency in The Intensive Care Unit: Samir El Ansary Icu Professor Ain Shams CairoDocument49 pagesAdrenal Insufficiency in The Intensive Care Unit: Samir El Ansary Icu Professor Ain Shams CairoGebby MamuayaNo ratings yet
- Addison’s Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandAddison’s Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- UntitledyuiDocument13 pagesUntitledyuiFadi Al HajjiNo ratings yet
- Untitled 234Document9 pagesUntitled 234Fadi Al HajjiNo ratings yet
- Update On Management of The Oral and Maxillofac - 2022 - Oral and MaxillofacialDocument8 pagesUpdate On Management of The Oral and Maxillofac - 2022 - Oral and MaxillofacialFadi Al HajjiNo ratings yet
- Socket Preservation For The General PractitionerDocument11 pagesSocket Preservation For The General PractitionerFadi Al HajjiNo ratings yet
- 123 UntitledDocument13 pages123 UntitledFadi Al HajjiNo ratings yet
- Decision Making for Thyroid Nodule Diagnosis and ManagementDocument15 pagesDecision Making for Thyroid Nodule Diagnosis and ManagementFadi Al HajjiNo ratings yet
- DownloadDocument16 pagesDownloadFadi Al HajjiNo ratings yet
- Nerve Evaluation Protocol 2014Document40 pagesNerve Evaluation Protocol 2014Fadi Al HajjiNo ratings yet
- 08-The Heritability of Malocclusion-Part 2 The Influence of Genetics in Malocclusion PDFDocument9 pages08-The Heritability of Malocclusion-Part 2 The Influence of Genetics in Malocclusion PDFFadi Al Hajji100% (1)
- Pediatric Neck Masses PDFDocument12 pagesPediatric Neck Masses PDFMaria Alejandra AtencioNo ratings yet
- Proliferative Verrucous Leukoplakia: Report of A Case With Characteristic Long-Term ProgressionDocument6 pagesProliferative Verrucous Leukoplakia: Report of A Case With Characteristic Long-Term ProgressionFadi Al HajjiNo ratings yet
- 08-The Heritability of Malocclusion-Part 2 The Influence of Genetics in Malocclusion PDFDocument9 pages08-The Heritability of Malocclusion-Part 2 The Influence of Genetics in Malocclusion PDFFadi Al Hajji100% (1)
- ISOMS - Illinois Society of Oral and Maxillofacial SurgeonsDocument5 pagesISOMS - Illinois Society of Oral and Maxillofacial SurgeonsFadi Al HajjiNo ratings yet
- Bai Tap Tieng Anh Lop 8 Unit 7 Environmental Protection Global SuccessDocument8 pagesBai Tap Tieng Anh Lop 8 Unit 7 Environmental Protection Global Successngtrmm1No ratings yet
- Electric Tool Parts List: Air Compressor 2007 - 04 - 02 Model EC 119 (E3)Document3 pagesElectric Tool Parts List: Air Compressor 2007 - 04 - 02 Model EC 119 (E3)Ivan GallegosNo ratings yet
- Math10 Q2 Mod24 WritingtheEquationofaCircleandDeterminingtheCenterandRadiusofaCircle V3-1Document19 pagesMath10 Q2 Mod24 WritingtheEquationofaCircleandDeterminingtheCenterandRadiusofaCircle V3-1Bridget SaladagaNo ratings yet
- Those Who Serve - Stephen Melillo (Score)Document22 pagesThose Who Serve - Stephen Melillo (Score)Fernando RamiresNo ratings yet
- Capacitive Touch Sensing, MSP430™ Slider and Wheel Tuning GuideDocument18 pagesCapacitive Touch Sensing, MSP430™ Slider and Wheel Tuning GuideFábio Carvalho FurtadoNo ratings yet
- #5class-8 (Cordova) Chapter-6 SCIENCE Coal and PetroleumDocument2 pages#5class-8 (Cordova) Chapter-6 SCIENCE Coal and PetroleumVivek PatidarNo ratings yet
- 986.33 Mesofilos Aerobios-PetrifilmDocument1 page986.33 Mesofilos Aerobios-PetrifilmBleidy NieblesNo ratings yet
- LNG Vessels and Their Bunkering - North America: Sean BondDocument18 pagesLNG Vessels and Their Bunkering - North America: Sean BondMaximNo ratings yet
- Price List Lang Technovation 02072019Document5 pagesPrice List Lang Technovation 02072019api-541004165No ratings yet
- 23 Section I GW Glasses Window System and MirrorsDocument58 pages23 Section I GW Glasses Window System and Mirrorsamir8100No ratings yet
- RTC Invoice 2965 Gj29es2223100505Document1 pageRTC Invoice 2965 Gj29es2223100505Alok PandeyNo ratings yet
- Etoricoxib Decreases Subchondrial Bone MassDocument9 pagesEtoricoxib Decreases Subchondrial Bone MassQuímica y FarmaciaNo ratings yet
- CAS circuit analysis simulationDocument9 pagesCAS circuit analysis simulationIan MejiaNo ratings yet
- Mobile C Arm PortfolioDocument6 pagesMobile C Arm PortfolioAri ReviantoNo ratings yet
- STK6712BMK4: Unipolar Fixed-Current Chopper-Type 4-Phase Stepping Motor DriverDocument11 pagesSTK6712BMK4: Unipolar Fixed-Current Chopper-Type 4-Phase Stepping Motor DriverGerardo WarmerdamNo ratings yet
- A 3-Channel Monopulse Tracking Receiver System Using Commercial Off-The-Shelf EquipmentDocument9 pagesA 3-Channel Monopulse Tracking Receiver System Using Commercial Off-The-Shelf EquipmentJean-Hubert DelassaleNo ratings yet
- Coastal Wall FinalDocument8 pagesCoastal Wall Finalapi-508287240No ratings yet
- Lecture Drugs in Sport - NotesDocument14 pagesLecture Drugs in Sport - NotesDavid FornitoNo ratings yet
- CS601 - Machine Learning - Unit 2 - Notes - 1672759753Document14 pagesCS601 - Machine Learning - Unit 2 - Notes - 1672759753mohit jaiswalNo ratings yet
- Id Card SoftwareDocument6 pagesId Card SoftwareAlli RaniNo ratings yet
- Skies of Arcadia - Lists (Cham, Moonfish, Discoveries)Document9 pagesSkies of Arcadia - Lists (Cham, Moonfish, Discoveries)123142asdadNo ratings yet
- Lightweight Slab Shoring System - ROYALFRAME50Document6 pagesLightweight Slab Shoring System - ROYALFRAME50Renji Delos ReyesNo ratings yet
- Abandonship Drill and LSA Training With Newly Join CrewDocument3 pagesAbandonship Drill and LSA Training With Newly Join CrewSashNo ratings yet
- Neuro Exam ReviewDocument6 pagesNeuro Exam ReviewDianne Flores100% (2)
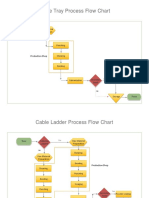
- Process Flow ChartDocument4 pagesProcess Flow Chartchacko chiramalNo ratings yet
- Humidity Chamber Tek For Fruiting BRF Cakes - Mushroom Cultivation - Shroomery Message BoardDocument15 pagesHumidity Chamber Tek For Fruiting BRF Cakes - Mushroom Cultivation - Shroomery Message BoardABIYA UNIVERSENo ratings yet
- Drug Treatment of AnemiaDocument6 pagesDrug Treatment of Anemiavingul2006No ratings yet
- Astronomy at The Frontiers of ScienceDocument380 pagesAstronomy at The Frontiers of ScienceΜαρια100% (1)
- LG Rotary Compressor GuideDocument32 pagesLG Rotary Compressor Guideวรศิษฐ์ อ๋อง33% (3)
- Unit 5 Grammar HFDocument7 pagesUnit 5 Grammar HFMilán Benjámin ZámbóNo ratings yet