You might also like
- 190 - Gestational Diabetes Mellitus AgogDocument16 pages190 - Gestational Diabetes Mellitus Agogjorge vergara100% (2)
- The Plot Against Asthma and Allergy PatientsDocument422 pagesThe Plot Against Asthma and Allergy PatientsAngelo100% (1)
- Oet Writing TipsDocument27 pagesOet Writing Tipsbjlk96% (47)
- Prescription Pattern and Glycaemic Control Using Glycated Haemoglobin in Type 2 Diabetic Patients A Cross-Sectional SurveyDocument9 pagesPrescription Pattern and Glycaemic Control Using Glycated Haemoglobin in Type 2 Diabetic Patients A Cross-Sectional SurveyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Clinical Review of Subcutaneous Semaglutide For ObesityDocument10 pagesClinical Review of Subcutaneous Semaglutide For ObesityGhygggNo ratings yet
- Clinical Pharmacy Therapeu - 2022 - Phillips - Clinical Review of Subcutaneous Semaglutide For ObesityDocument10 pagesClinical Pharmacy Therapeu - 2022 - Phillips - Clinical Review of Subcutaneous Semaglutide For ObesityArtyy ArtyyNo ratings yet
- Drug Literature ReviewDocument9 pagesDrug Literature Reviewabenezer g/kirstosNo ratings yet
- Clinical Effectiveness and Safety of Vildagliptin in With Type 2 DiabetesDocument8 pagesClinical Effectiveness and Safety of Vildagliptin in With Type 2 DiabetesSMEY204No ratings yet
- Gliclazide Metformin Study Type 2 Diabetes PatientsDocument7 pagesGliclazide Metformin Study Type 2 Diabetes PatientsLyka MahrNo ratings yet
- The Risk of Overt Diabetes Mellitus AmonDocument7 pagesThe Risk of Overt Diabetes Mellitus AmonΛΟΥΚΙΑ ΣΠΑΝΟΥNo ratings yet
- BMJ h6138 FullDocument10 pagesBMJ h6138 FullFede0No ratings yet
- tmp2475 TMPDocument7 pagestmp2475 TMPFrontiersNo ratings yet
- Vildagliptin Vs Sitagliptin (Lowering Glucose Fluctuation)Document8 pagesVildagliptin Vs Sitagliptin (Lowering Glucose Fluctuation)RaniNo ratings yet
- Temporary Changes in Clinical Guidelines of Gesta - 2020 - Diabetes - Metabolic PDFDocument4 pagesTemporary Changes in Clinical Guidelines of Gesta - 2020 - Diabetes - Metabolic PDFdianNo ratings yet
- Shamsi Et Al, 2013Document11 pagesShamsi Et Al, 2013larissa matosNo ratings yet
- 125 2018 Article 4728Document8 pages125 2018 Article 4728Luna Sofia Arias RojasNo ratings yet
- dmj-37-465Document10 pagesdmj-37-465sn4s7nyxcbNo ratings yet
- Bo Ahr En, Susan L. Johnson, Murray Stewart, Deborah T. Cirkel, Fred Yang, Caroline Perry, and Mark N. Feinglos, For The HARMONY 3 Study GroupDocument8 pagesBo Ahr En, Susan L. Johnson, Murray Stewart, Deborah T. Cirkel, Fred Yang, Caroline Perry, and Mark N. Feinglos, For The HARMONY 3 Study GroupTari SehatiNo ratings yet
- 2019 Clinical Practice Guidelines For Type 2 Diabetes Mellitus in KoreaDocument9 pages2019 Clinical Practice Guidelines For Type 2 Diabetes Mellitus in KoreaNana Rochmatun NazzilahNo ratings yet
- Diagnosing Dysglycemia in Adolescents With Polycystic Ovary Syndrome 2014 Journal of Adolescent HealthDocument6 pagesDiagnosing Dysglycemia in Adolescents With Polycystic Ovary Syndrome 2014 Journal of Adolescent HealthfujimeisterNo ratings yet
- Ass Knowledge and MaDocument1 pageAss Knowledge and MaB04-BALKIS SOLEHAHNo ratings yet
- The Influence of Glucose Self-Monitoring On Glycaemic Control in Patients With Diabetes Mellitus in SudanDocument5 pagesThe Influence of Glucose Self-Monitoring On Glycaemic Control in Patients With Diabetes Mellitus in SudanZam-zam RsiNo ratings yet
- Vildagliptin A New Oral Treatment For Type 2Document12 pagesVildagliptin A New Oral Treatment For Type 2Andhi Fahrurroji100% (1)
- Factor Associated With Long-Term Control Blood Glucose Based On Hba1C Level in Type 2 Diabetes Mellitus PatientsDocument5 pagesFactor Associated With Long-Term Control Blood Glucose Based On Hba1C Level in Type 2 Diabetes Mellitus PatientsYuswandi Satya PermanaNo ratings yet
- Efficacy of Vildagliptin and Metformin Combination in Type II Diabetes Mellitus PatientsDocument4 pagesEfficacy of Vildagliptin and Metformin Combination in Type II Diabetes Mellitus PatientsDR.P.KALAI SELVINo ratings yet
- Efficacy and Safety of Pioglitazone Versus Glimepiride After Metformin and Alogliptin Combination TherapyDocument11 pagesEfficacy and Safety of Pioglitazone Versus Glimepiride After Metformin and Alogliptin Combination TherapyaldyNo ratings yet
- Effect of Metformin As Adjunct Therapy With Insulin in Adolescent Pakistani People With Type 1 DiabetesDocument4 pagesEffect of Metformin As Adjunct Therapy With Insulin in Adolescent Pakistani People With Type 1 DiabetesSundas EjazNo ratings yet
- Long-Term Efficacy and Safety of Ertugliflozin Monotherapy in Patients WithDocument23 pagesLong-Term Efficacy and Safety of Ertugliflozin Monotherapy in Patients WithPhạm DuyênNo ratings yet
- The Glucose-Lowering Efficacy of Sitagliptin in Obese Japanese Patients With Type 2 DiabetesDocument9 pagesThe Glucose-Lowering Efficacy of Sitagliptin in Obese Japanese Patients With Type 2 DiabetesJavier VillavicencioNo ratings yet
- Research ArticleDocument12 pagesResearch ArticleRodas GetachewNo ratings yet
- Original ArticleDocument10 pagesOriginal ArticlegistaluvikaNo ratings yet
- Gestationaldiabetes Mellitus: Emily D. Szmuilowicz,, Jami L. Josefson,, Boyd E. MetzgerDocument15 pagesGestationaldiabetes Mellitus: Emily D. Szmuilowicz,, Jami L. Josefson,, Boyd E. Metzgerjose ricardo escalante perezNo ratings yet
- Evaluation of The Effectiveness and Tolerability of Glicazide During RamadanDocument10 pagesEvaluation of The Effectiveness and Tolerability of Glicazide During RamadanAnonymous EAPbx6No ratings yet
- Metformin For GDMDocument7 pagesMetformin For GDMRoro WidyastutiNo ratings yet
- Self-monitoring blood glucose newly diagnosed type 2 diabetes patientsDocument7 pagesSelf-monitoring blood glucose newly diagnosed type 2 diabetes patientsAhmedaref EzrinNo ratings yet
- March 2019 1551446825 124Document3 pagesMarch 2019 1551446825 124Anjali Rahul AjmeriNo ratings yet
- Quality Improvement Project.Document7 pagesQuality Improvement Project.rhinoNo ratings yet
- Literature Review of Gestational Diabetes MellitusDocument7 pagesLiterature Review of Gestational Diabetes Mellitusc5rc7ppr100% (1)
- JurnalDocument3 pagesJurnalARINANo ratings yet
- Eficiencia y Tolerabilidad Glimepirida y MetfomrinaDocument7 pagesEficiencia y Tolerabilidad Glimepirida y MetfomrinaMarioA.VelascoCórdobaNo ratings yet
- Diabetes and Clinical Research: ClinmedDocument4 pagesDiabetes and Clinical Research: ClinmedHerybert KiiNo ratings yet
- Was This A Randomized Controlled Trial (RCT) and Was It Appropriate So?Document29 pagesWas This A Randomized Controlled Trial (RCT) and Was It Appropriate So?lordizzatNo ratings yet
- Scientific Advisory Committee Opinion Paper 23: 1. BackgroundDocument5 pagesScientific Advisory Committee Opinion Paper 23: 1. BackgroundNatia DemetradzeNo ratings yet
- 17 ShaofangDocument4 pages17 Shaofangiriartenela14No ratings yet
- SITAGLIPTINDocument15 pagesSITAGLIPTINOnon EssayedNo ratings yet
- Comparison of Efficacy and Safety Profile of Empagliflozin Versus Dapagliflozin As Add On Therapy in Type 2 Diabetic PatientsDocument6 pagesComparison of Efficacy and Safety Profile of Empagliflozin Versus Dapagliflozin As Add On Therapy in Type 2 Diabetic Patientsthomas albertNo ratings yet
- Scheen 2010Document10 pagesScheen 2010Lyka MahrNo ratings yet
- Dia Care-2007-Moore-S209-13Document5 pagesDia Care-2007-Moore-S209-13salijanstarNo ratings yet
- 1-Definition Epidemiology and Classification of Diabetes in Children and Adolescents PDFDocument14 pages1-Definition Epidemiology and Classification of Diabetes in Children and Adolescents PDFFrancys Sierra FariasNo ratings yet
- Ajtr0014 4757Document20 pagesAjtr0014 4757Eyal RobinsonNo ratings yet
- Diagnosis and Treatment of Gestational Diabetes: Scientific Impact Paper No. 23Document6 pagesDiagnosis and Treatment of Gestational Diabetes: Scientific Impact Paper No. 23Ane DamayantiNo ratings yet
- Wjarr 2022 1252Document9 pagesWjarr 2022 1252Eduardo Luis Flores QuispeNo ratings yet
- Metformin For Diabetes Prevention: Insights Gained From The Diabetes Prevention Program/Diabetes Prevention Program Outcomes StudyDocument11 pagesMetformin For Diabetes Prevention: Insights Gained From The Diabetes Prevention Program/Diabetes Prevention Program Outcomes StudyRosa Villanueva CarrascoNo ratings yet
- Tan, 2022Document8 pagesTan, 2022Mirilláiny AnacletoNo ratings yet
- Obesity Reviews 2020 Chadda GLP1 Agonists For Obesity and Type 2 Diabetes in Children Systematic Review andDocument10 pagesObesity Reviews 2020 Chadda GLP1 Agonists For Obesity and Type 2 Diabetes in Children Systematic Review andTaniaNo ratings yet
- Towards A Global Consensus On GDM Diagnosis Light at The End of The TunnelDocument5 pagesTowards A Global Consensus On GDM Diagnosis Light at The End of The TunnelYuliana NaviaNo ratings yet
- Clinical StudyDocument13 pagesClinical StudyNovia QomariahNo ratings yet
- Gestational Diabetes Mellitus DiagnosedDocument5 pagesGestational Diabetes Mellitus DiagnosedMutia AgustriaNo ratings yet
- 47 Manuscript 226 5 10 20210811Document6 pages47 Manuscript 226 5 10 20210811Dikri NurfazrinNo ratings yet
- Efficacy and Safety of Biosimilar Glargine-IMGDocument8 pagesEfficacy and Safety of Biosimilar Glargine-IMGSiddiq MohammedNo ratings yet
- Dexcom G6 CGM System Performance in Pregnant WomenDocument5 pagesDexcom G6 CGM System Performance in Pregnant WomenRizqi Fauzi Nurul AwalinNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- Vildagliptin Effectiveness and Safety in T2DM Patients in Real-World SettingsDocument5 pagesVildagliptin Effectiveness and Safety in T2DM Patients in Real-World SettingsSMEY204No ratings yet
- Amcsecondary Amenorrhea Gynecology WorkbookDocument2 pagesAmcsecondary Amenorrhea Gynecology WorkbookSMEY204No ratings yet
- Vildagliptin Effectiveness and Safety in T2DM Patients in Real-World SettingsDocument5 pagesVildagliptin Effectiveness and Safety in T2DM Patients in Real-World SettingsSMEY204No ratings yet
- Presentation SlidesDocument8 pagesPresentation SlidesSMEY204No ratings yet
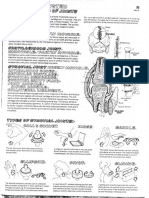
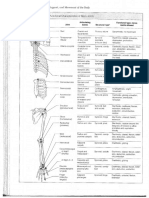
- Notes On Joints of The BodyDocument19 pagesNotes On Joints of The BodySMEY204No ratings yet
- Joints Picture ofDocument1 pageJoints Picture ofSMEY204No ratings yet
- Sentence Analogies 1Document1 pageSentence Analogies 1Deea EaNo ratings yet
- PP Ulcere de La CorneeDocument31 pagesPP Ulcere de La CorneeSMEY204No ratings yet
- The Polar BearDocument2 pagesThe Polar BearSMEY204No ratings yet
- Joints Sample Pop QuizDocument2 pagesJoints Sample Pop QuizSMEY204No ratings yet
- Chapter 22 SpleenDocument69 pagesChapter 22 SpleenMACON824100% (1)
- Joints Old Test SampleDocument5 pagesJoints Old Test SampleSMEY204No ratings yet
- 1 Anatomy & Physiology of Eye For Ophthalmic NursesDocument124 pages1 Anatomy & Physiology of Eye For Ophthalmic NursesSMEY204100% (1)
- Anatomy PDFDocument4 pagesAnatomy PDFSMEY204No ratings yet
- Blood On Ice in The Artic Is Not A Sign of DeathDocument1 pageBlood On Ice in The Artic Is Not A Sign of DeathSMEY204No ratings yet
- Chapter 13 PharynxDocument40 pagesChapter 13 PharynxSMEY204No ratings yet
- Chapter 14 EsophagusDocument48 pagesChapter 14 EsophagusSMEY204No ratings yet
- Brulure Oculaire: By: DR To Chhun SengDocument22 pagesBrulure Oculaire: By: DR To Chhun SengSMEY204No ratings yet
- Brulure Oculaire: By: DR To Chhun SengDocument22 pagesBrulure Oculaire: By: DR To Chhun SengSMEY204No ratings yet
- Chapter 2 Thoracic Wall and Pleurae PDFDocument40 pagesChapter 2 Thoracic Wall and Pleurae PDFSMEY204No ratings yet
- Chapter 18 Large Intestine and AnorectumDocument159 pagesChapter 18 Large Intestine and AnorectumSMEY204No ratings yet
- Chapter 1 NeckDocument125 pagesChapter 1 NeckMACON824No ratings yet
- Chapter 10 Peritoneium, Omenta, and InternalDocument62 pagesChapter 10 Peritoneium, Omenta, and InternalSMEY204No ratings yet
- Chapter 10 Peritoneium, Omenta, and InternalDocument62 pagesChapter 10 Peritoneium, Omenta, and InternalSMEY204No ratings yet
- Jamorama Chord BookDocument76 pagesJamorama Chord BookJamie Chan JieminNo ratings yet
- Chapter 3 Breast PDFDocument35 pagesChapter 3 Breast PDFSMEY204No ratings yet
- Mask LTR 6.16 PDF No HLDocument14 pagesMask LTR 6.16 PDF No HLJoshua LingNo ratings yet
- Archaeus 4Document107 pagesArchaeus 4terrythecensorNo ratings yet
- Post-Partum HemorrhageDocument15 pagesPost-Partum Hemorrhageapi-257029163No ratings yet
- Guide Adult Neurological ObservationDocument20 pagesGuide Adult Neurological ObservationSimon S. KledenNo ratings yet
- Clinico-Aetiological Profile of Pancytopenia in Paediatric PracticeDocument4 pagesClinico-Aetiological Profile of Pancytopenia in Paediatric PracticeDesi AdiyatiNo ratings yet
- Glossary of Patient SafetyDocument352 pagesGlossary of Patient SafetyEman ShalabyNo ratings yet
- FDA Warning Letter 3 2010Document2 pagesFDA Warning Letter 3 2010Nalini RajamannanNo ratings yet
- PDA Dental ChartDocument2 pagesPDA Dental ChartzrinaNo ratings yet
- Date Performed: Final Grade: Clinical Instructor: Administering Eye Medication DefinitionDocument3 pagesDate Performed: Final Grade: Clinical Instructor: Administering Eye Medication Definitionhjl padillaNo ratings yet
- People vs. Ventura, G.R. No. L-15079Document5 pagesPeople vs. Ventura, G.R. No. L-15079Ina Villarica100% (1)
- The Allergenicity of Genetically Modi Fied Foods From Genetically Engineered CropsDocument12 pagesThe Allergenicity of Genetically Modi Fied Foods From Genetically Engineered Cropsben mayNo ratings yet
- RPS Hospital Ranchi Total Marks - 30 Question Paper Set - 1Document7 pagesRPS Hospital Ranchi Total Marks - 30 Question Paper Set - 1Tanisha Singh100% (1)
- Iwq 0 K J98 V 8 KFPV 5 W 4 ZH 5 Z Q08 NJ Cy 30 PPBAo MXX 4 LDocument243 pagesIwq 0 K J98 V 8 KFPV 5 W 4 ZH 5 Z Q08 NJ Cy 30 PPBAo MXX 4 Lmaleknour2000No ratings yet
- Infantile AutismDocument1 pageInfantile Autismapi-260339450No ratings yet
- Spastic Diplegic Cerebral PalsyDocument43 pagesSpastic Diplegic Cerebral PalsyRachel GardnerNo ratings yet
- Cytometry Part B Clinical - 2020 - Illingworth - International Guidelines For The Flow Cytometric Evaluation of PeripheralDocument28 pagesCytometry Part B Clinical - 2020 - Illingworth - International Guidelines For The Flow Cytometric Evaluation of PeripheralUcha PrasetyoNo ratings yet
- Chapter 38: Cardiovascular Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument7 pagesChapter 38: Cardiovascular Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Patient Medication SheetDocument1 pagePatient Medication SheetYang YangNo ratings yet
- Relationship Between Patients' Knowledge and Medication Adherence Among Patients With HypertensionDocument8 pagesRelationship Between Patients' Knowledge and Medication Adherence Among Patients With HypertensionWina MariaNo ratings yet
- Paul Farmer, Pioneer of Global Health, Dies at 62Document3 pagesPaul Farmer, Pioneer of Global Health, Dies at 62ALFINo ratings yet
- 9 Top Benefits of KarakkayaDocument4 pages9 Top Benefits of KarakkayaAcharla SatyanarayanaNo ratings yet
- Assessment of Antiangiogenic Properties of Mallotus SPDocument6 pagesAssessment of Antiangiogenic Properties of Mallotus SPSheila GarciaNo ratings yet
- Non Sterile Dressing ChangeDocument2 pagesNon Sterile Dressing ChangePam West0% (1)
- Investigation and Treatment of Surgical JaundiceDocument38 pagesInvestigation and Treatment of Surgical JaundiceUjas PatelNo ratings yet
- RSD 4Document12 pagesRSD 4GopakumarNo ratings yet
- Breathing Control: Pistol@tenrings - Co.ukDocument1 pageBreathing Control: Pistol@tenrings - Co.ukmanfromgladNo ratings yet
- CDFDocument76 pagesCDFmishra.nagendra7311No ratings yet
- Unconsciousness: Law and MedicineDocument10 pagesUnconsciousness: Law and MedicineDhivya GaneshNo ratings yet