You might also like
- Swiss Army Triplet 1Document2 pagesSwiss Army Triplet 1johnpwayNo ratings yet
- Protein Binding of DrugDocument22 pagesProtein Binding of DrugManikanta GupthaNo ratings yet
- Questions - Answer Bassam QQ 1Document14 pagesQuestions - Answer Bassam QQ 1Bassam SaifNo ratings yet
- Baby DedicationDocument3 pagesBaby DedicationLouriel Nopal100% (3)
- Present Perfect Simp ContDocument14 pagesPresent Perfect Simp ContLauGalindo100% (1)
- Drug Interaction Can Be Defined As TheDocument34 pagesDrug Interaction Can Be Defined As TheIstianah Es100% (1)
- Science9 Q4 Week2Document16 pagesScience9 Q4 Week2Maria Josie Lopez TumlosNo ratings yet
- نم هدمتعم و هعجارم اهنل اهب قوثوم لخادلاب تامولعملا Certified fromDocument20 pagesنم هدمتعم و هعجارم اهنل اهب قوثوم لخادلاب تامولعملا Certified fromMedhat EyadaNo ratings yet
- Prometric Questions-1 AnswersDocument45 pagesPrometric Questions-1 AnswersNina Grace Joy Marayag-Alvarez100% (1)
- Drug InteractionsDocument5 pagesDrug Interactionsvajkember100% (1)
- Clinical PharmacologDocument81 pagesClinical PharmacologSHILOTANo ratings yet
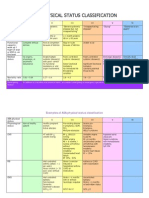
- ASADocument3 pagesASAMelisa Malik50% (2)
- Storage-Tanks Titik Berat PDFDocument72 pagesStorage-Tanks Titik Berat PDF'viki Art100% (1)
- 03 IGT-Influence of Codes Guidelines and Other Regulations On The Tunnel Design in AustriaDocument48 pages03 IGT-Influence of Codes Guidelines and Other Regulations On The Tunnel Design in AustriaSudarshan GadalkarNo ratings yet
- Handbook of Drug Interaction and the Mechanism of InteractionFrom EverandHandbook of Drug Interaction and the Mechanism of InteractionRating: 1 out of 5 stars1/5 (1)
- Pharmacology in Drug Discovery: Understanding Drug ResponseFrom EverandPharmacology in Drug Discovery: Understanding Drug ResponseNo ratings yet
- Plasma Protein BindingDocument2 pagesPlasma Protein BindingKavish ChhajedNo ratings yet
- Protein Binding of DrugsDocument17 pagesProtein Binding of DrugsPrasanna BabuNo ratings yet
- Interaksi Farmakokinetika DistribusiDocument3 pagesInteraksi Farmakokinetika DistribusijessicaNo ratings yet
- Protein Binding Effect On PKDocument8 pagesProtein Binding Effect On PKMaha AhmedNo ratings yet
- Revision KitDocument58 pagesRevision KitTracy MNo ratings yet
- Factors Contributing To Variability in Drug Pharmacokinetics. 11. Drug DistributionDocument9 pagesFactors Contributing To Variability in Drug Pharmacokinetics. 11. Drug DistributionStella WatkinsNo ratings yet
- Factors Contributing To Variability in Drug Pharmacokinetics. 11. Drug DistributionDocument9 pagesFactors Contributing To Variability in Drug Pharmacokinetics. 11. Drug DistributionStella WatkinsNo ratings yet
- Biopharmaceutics &pharmakinetics: Subject Code-604t Unit - 1Document27 pagesBiopharmaceutics &pharmakinetics: Subject Code-604t Unit - 1Babbu Singh GurjarNo ratings yet
- Drug InteractionsDocument43 pagesDrug InteractionsNinaNo ratings yet
- Assignment On Pharmacokinetic Drug Interaction: Teerthanker Mahaveer UniversityDocument8 pagesAssignment On Pharmacokinetic Drug Interaction: Teerthanker Mahaveer Universityt24008882No ratings yet
- Protein Binding of Drug: Page - 1 CMR College of Pharmacy, 2013Document18 pagesProtein Binding of Drug: Page - 1 CMR College of Pharmacy, 2013REDDYGAARI ABBAYINo ratings yet
- Age-Related Changes in Protein Binding of Drugs: Implications For TherapyDocument4 pagesAge-Related Changes in Protein Binding of Drugs: Implications For TherapyIlham Hilmi MutaqinNo ratings yet
- Protein BindingDocument15 pagesProtein Bindingyasmin lisana shidqiNo ratings yet
- Plasma Protein Binding of Drugs Advanced PharmacologyDocument2 pagesPlasma Protein Binding of Drugs Advanced PharmacologySANJAY K GOWDANo ratings yet
- DD - Quiz 2Document7 pagesDD - Quiz 2angelamnsrNo ratings yet
- Pharmacokinetics in Pregnancy 1: Matthew Dawes Philip J. ChowienczykDocument8 pagesPharmacokinetics in Pregnancy 1: Matthew Dawes Philip J. ChowienczykNandini GujjariNo ratings yet
- Protein Binding of Drugs: Page - 1 CMR College of Pharmacy, 2013Document20 pagesProtein Binding of Drugs: Page - 1 CMR College of Pharmacy, 2013REDDYGAARI ABBAYINo ratings yet
- NONlinear PKDocument5 pagesNONlinear PKbournvilleeaterNo ratings yet
- Assingment of PharmacologyDocument9 pagesAssingment of PharmacologyAbdiwahab AbdirasakNo ratings yet
- Protein BindingDocument22 pagesProtein BindingDeepakNo ratings yet
- PregnancyDocument16 pagesPregnancyMydhilyNo ratings yet
- Farmacologia em Cães GeriátricosDocument12 pagesFarmacologia em Cães GeriátricosRafaela RodriguesNo ratings yet
- PharmacokineticsDocument2 pagesPharmacokineticsMihaela Toma100% (1)
- Chapter 2Document13 pagesChapter 2simbaiNo ratings yet
- Protein Binding: Dr. Abid Yousaf, PHDDocument23 pagesProtein Binding: Dr. Abid Yousaf, PHDSalman KhanNo ratings yet
- Mechanism of Protein Binding of Drug To ReceptorsDocument7 pagesMechanism of Protein Binding of Drug To ReceptorsZubiya SiddiquiNo ratings yet
- Review Article Dose-Dependent Pharmacokinetics: Experimental Observations and Theoretical ConsiderationsDocument31 pagesReview Article Dose-Dependent Pharmacokinetics: Experimental Observations and Theoretical Considerationsירדן לויןNo ratings yet
- I0003 3006 58 1 31 PDFDocument11 pagesI0003 3006 58 1 31 PDFGaby ValenzuelaNo ratings yet
- HIPOALBUMINADocument4 pagesHIPOALBUMINAPedroCordovageNo ratings yet
- Protein Binding: Naila Abbasi Assistant Professor Department of PharmacyDocument50 pagesProtein Binding: Naila Abbasi Assistant Professor Department of PharmacyMuhammad MursaleenNo ratings yet
- Of Complex Formation With Proteins Is Called As Protein Binding of DrugsDocument16 pagesOf Complex Formation With Proteins Is Called As Protein Binding of DrugsDeepak duaNo ratings yet
- CU SHAH - Refresher Course - 02-10-2016 FinalDocument38 pagesCU SHAH - Refresher Course - 02-10-2016 FinalParthMairNo ratings yet
- Jurna BSADocument7 pagesJurna BSAIna SuciNo ratings yet
- Drug DistributionDocument8 pagesDrug DistributionBriana NdayisabaNo ratings yet
- Pharmacokinetic: Herni SupraptiDocument76 pagesPharmacokinetic: Herni SupraptiveniNo ratings yet
- Distribution of Drug AssignmentDocument9 pagesDistribution of Drug AssignmentHammadraza MustafaiNo ratings yet
- Protein-Drug BindingDocument28 pagesProtein-Drug BindingManveer. SinghNo ratings yet
- Pharmacokinetic in PregnancyDocument7 pagesPharmacokinetic in PregnancyPatrick AnthonyNo ratings yet
- Xenobiotics BCH 421 Kwasu 2Document16 pagesXenobiotics BCH 421 Kwasu 2idriscognitoleadsNo ratings yet
- Pharmacokinetics and Metabolic Drug InteractionsDocument16 pagesPharmacokinetics and Metabolic Drug InteractionsNelson LombanaNo ratings yet
- What Is Drug Interaction?: Drug-Drug Drug-Food Drug-Plant Drug-Alcohol Drug-Disease Drug-LaboratoryDocument6 pagesWhat Is Drug Interaction?: Drug-Drug Drug-Food Drug-Plant Drug-Alcohol Drug-Disease Drug-LaboratoryQuách Việt HoàngNo ratings yet
- Protein Binding of DrugsDocument29 pagesProtein Binding of Drugstry.vishaldhamole78No ratings yet
- Drug - Drug Int2Document35 pagesDrug - Drug Int2alishba100% (2)
- Australian Prescriber (1988) Bioavailability and First Past ClearanceDocument3 pagesAustralian Prescriber (1988) Bioavailability and First Past Clearance1234chocoNo ratings yet
- Protein Drug BindingDocument26 pagesProtein Drug BindingBandita DattaNo ratings yet
- Bioavailability and Bioequivalence. Therapeutic Drug MonitoringDocument3 pagesBioavailability and Bioequivalence. Therapeutic Drug MonitoringJoel MathewNo ratings yet
- PHARMACOLOGYDocument12 pagesPHARMACOLOGYhassangarba6464No ratings yet
- Bioavailability and First Pass ClearanceDocument3 pagesBioavailability and First Pass ClearanceMergu Bala RajuNo ratings yet
- 41-46 TEXTBOOK The Asam Essentials of Addiction MedicineDocument7 pages41-46 TEXTBOOK The Asam Essentials of Addiction MedicineErlanNo ratings yet
- Pharmacokinetics of Anti-Epileptic Drugs and Their Clinical SignificanceDocument12 pagesPharmacokinetics of Anti-Epileptic Drugs and Their Clinical Significancerozina mulatNo ratings yet
- Dexamethasone Suppression TestDocument3 pagesDexamethasone Suppression TestMelisa MalikNo ratings yet
- MultidrugDocument3 pagesMultidrugMelisa MalikNo ratings yet
- Cardiac GlycosideDocument1 pageCardiac GlycosideMelisa MalikNo ratings yet
- Storage DevicesDocument2 pagesStorage DevicesMelisa MalikNo ratings yet
- COMPASSDocument3 pagesCOMPASSMelisa MalikNo ratings yet
- Bryan Guy Adams OC OBC FRPSDocument3 pagesBryan Guy Adams OC OBC FRPSMelisa MalikNo ratings yet
- Michael BoltonDocument4 pagesMichael BoltonMelisa MalikNo ratings yet
- Analysis of Serum Lipid Profile in Cholelithiasis PatientsDocument9 pagesAnalysis of Serum Lipid Profile in Cholelithiasis PatientsMelisa MalikNo ratings yet
- All I Am Thingking ofDocument1 pageAll I Am Thingking ofMelisa MalikNo ratings yet
- Stay With MeDocument1 pageStay With MeMelisa MalikNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaMelisa MalikNo ratings yet
- Super Duper Love by Joss StoneDocument2 pagesSuper Duper Love by Joss StoneMelisa MalikNo ratings yet
- Yu ZbornikDocument511 pagesYu ZbornikВладимирРакоњацNo ratings yet
- UpdateJul2007 3julDocument10 pagesUpdateJul2007 3julAnshul SinghNo ratings yet
- Effects of Corneal Scars and Their Treatment With Rigid Contact Lenses On Quality of VisionDocument5 pagesEffects of Corneal Scars and Their Treatment With Rigid Contact Lenses On Quality of VisionJasmine EffendiNo ratings yet
- Chudamani Women Expecting ChangeDocument55 pagesChudamani Women Expecting ChangeMr AnantNo ratings yet
- Chapter 1 INTRODUCTION TO LITERATUREDocument4 pagesChapter 1 INTRODUCTION TO LITERATUREDominique TurlaNo ratings yet
- School Activity Calendar - Millsberry SchoolDocument2 pagesSchool Activity Calendar - Millsberry SchoolSushil DahalNo ratings yet
- ManualDocument24 pagesManualCristian ValenciaNo ratings yet
- Unit 3: Theories and Principles in The Use and Design of Technology Driven Learning LessonsDocument5 pagesUnit 3: Theories and Principles in The Use and Design of Technology Driven Learning Lessons서재배No ratings yet
- Simple Enzymes Kinetics and Kinetics ModelDocument14 pagesSimple Enzymes Kinetics and Kinetics ModelSidra-tul MuntahaNo ratings yet
- 2017LR72 - SUMMARY REPORT Final 03052020Document72 pages2017LR72 - SUMMARY REPORT Final 03052020Dung PhamNo ratings yet
- The Philippine GovernmentDocument21 pagesThe Philippine GovernmentChristel ChuchipNo ratings yet
- 2nd Second Sun of Advent (B)Document4 pages2nd Second Sun of Advent (B)Max PolakNo ratings yet
- Materials Management - 1 - Dr. VP - 2017-18Document33 pagesMaterials Management - 1 - Dr. VP - 2017-18Vrushabh ShelkarNo ratings yet
- HPSC HCS Exam 2021: Important DatesDocument6 pagesHPSC HCS Exam 2021: Important DatesTejaswi SaxenaNo ratings yet
- Chapter 9Document28 pagesChapter 9Aniket BatraNo ratings yet
- Dummy 13 Printable Jointed Figure Beta FilesDocument9 pagesDummy 13 Printable Jointed Figure Beta FilesArturo GuzmanNo ratings yet
- Essay On Stem CellsDocument4 pagesEssay On Stem CellsAdrien G. S. WaldNo ratings yet
- Gandhi and The Non-Cooperation MovementDocument6 pagesGandhi and The Non-Cooperation MovementAliya KhanNo ratings yet
- Monster Hunter: World - Canteen IngredientsDocument5 pagesMonster Hunter: World - Canteen IngredientsSong HoeNo ratings yet
- Ass AsDocument23 pagesAss AsMukesh BishtNo ratings yet
- CBC DrivingDocument74 pagesCBC DrivingElonah Jean ConstantinoNo ratings yet
- Review Course 2 (Review On Professional Education Courses)Document8 pagesReview Course 2 (Review On Professional Education Courses)Regie MarcosNo ratings yet
- Arc Hydro - Identifying and Managing SinksDocument35 pagesArc Hydro - Identifying and Managing SinkskbalNo ratings yet