You might also like
- Handbook of Drug Interaction and the Mechanism of InteractionFrom EverandHandbook of Drug Interaction and the Mechanism of InteractionRating: 1 out of 5 stars1/5 (1)
- Taking Medicines in Pregnancy: What’s Safe and What’s Not - What The Experts SayFrom EverandTaking Medicines in Pregnancy: What’s Safe and What’s Not - What The Experts SayNo ratings yet
- Pharmacokinetic in PregnancyDocument7 pagesPharmacokinetic in PregnancyPatrick AnthonyNo ratings yet
- Special Aspects ofDocument6 pagesSpecial Aspects ofNaldi SufriNo ratings yet
- Treatment of Antibiotics in Dogs and Cats During PregnancyDocument9 pagesTreatment of Antibiotics in Dogs and Cats During PregnancyNoe Moreno GumetaNo ratings yet
- Clinical Pharmacology 9-16Document31 pagesClinical Pharmacology 9-16mill otoiNo ratings yet
- Drugs Used During Pregnancy and LactationDocument21 pagesDrugs Used During Pregnancy and LactationHarsheethaNo ratings yet
- Neonatal pharmacology and pharmacokinetics overviewDocument8 pagesNeonatal pharmacology and pharmacokinetics overviewRafael Flores PintoNo ratings yet
- Pediatric Pharmacology - Dr. JangiDocument29 pagesPediatric Pharmacology - Dr. JangiBashar Khalil100% (1)
- Prenatal Pharmacology ConcernsDocument23 pagesPrenatal Pharmacology Concerns88AKKNo ratings yet
- CPT 2nd ChapDocument33 pagesCPT 2nd ChapTarun GuruvelliNo ratings yet
- DNI During LactationDocument3 pagesDNI During Lactationbashirkinza679No ratings yet
- Some Issues To Consider While Prescribing Medications For : Pregnant and Lactating PatientsDocument25 pagesSome Issues To Consider While Prescribing Medications For : Pregnant and Lactating PatientsKishor Bajgain100% (1)
- Respiratory DiseasesDocument65 pagesRespiratory DiseasesWamani Linus KirungiNo ratings yet
- Drugs in Pregnancy and Lactation 2021Document51 pagesDrugs in Pregnancy and Lactation 2021LU'LUIL MUNIROHNo ratings yet
- Paediatric Pharmacology TOTW 048 2007Document10 pagesPaediatric Pharmacology TOTW 048 2007Lora MyrickNo ratings yet
- Pharmacokinetics and pharmacodynamics of anaesthetic drugs in paediatricsDocument7 pagesPharmacokinetics and pharmacodynamics of anaesthetic drugs in paediatricsR KNo ratings yet
- Drug Therapy Across The LifespanDocument34 pagesDrug Therapy Across The LifespanJSeasharkNo ratings yet
- Unit IV Drugs Used in PregnancyDocument32 pagesUnit IV Drugs Used in PregnancySuvinder singh PannuNo ratings yet
- Drug Therapy in Pregnancy and LactationDocument13 pagesDrug Therapy in Pregnancy and LactationMydhilyNo ratings yet
- 5perinatal Pediatric PharmacologyDocument5 pages5perinatal Pediatric Pharmacologymkpkqc4j4hNo ratings yet
- Kuliah 3 Obat-Obat TeratogenikDocument38 pagesKuliah 3 Obat-Obat TeratogenikMuhammad AidilNo ratings yet
- Aspects of Pharmacology in The Neonatal FoalDocument26 pagesAspects of Pharmacology in The Neonatal FoalAristoteles Esteban Cine VelazquezNo ratings yet
- L-23 Drugs Used During Pregnancy and LactationDocument21 pagesL-23 Drugs Used During Pregnancy and LactationAadil AminNo ratings yet
- Breastfeeding & Psychiatric Medications - MGH Centerfor Women's Mental Health (2022)Document7 pagesBreastfeeding & Psychiatric Medications - MGH Centerfor Women's Mental Health (2022)José Antonio Alves VilelaNo ratings yet
- Pharmacokinetics of Anti-Epileptic DrugsDocument12 pagesPharmacokinetics of Anti-Epileptic Drugsrozina mulatNo ratings yet
- Clinical Pharmacy (Chapter 1) : Drug Use in Pregnancy & LactationDocument40 pagesClinical Pharmacy (Chapter 1) : Drug Use in Pregnancy & LactationAnonymous DgPsK0oQNo ratings yet
- Drug Use in Pregnancy: Understanding FDA Categories and Teratogenic RisksDocument7 pagesDrug Use in Pregnancy: Understanding FDA Categories and Teratogenic RisksciobotaruclaudiuNo ratings yet
- Pharmaceutics: Factors and Mechanisms For Pharmacokinetic Differences Between Pediatric Population and AdultsDocument20 pagesPharmaceutics: Factors and Mechanisms For Pharmacokinetic Differences Between Pediatric Population and AdultsRosa Gdp GarciaNo ratings yet
- Pharmacotherapy of The Dental Patient During Pregnancy and LactationDocument6 pagesPharmacotherapy of The Dental Patient During Pregnancy and Lactationfarmasi RSUD joharbaruNo ratings yet
- AGE AND DRUG DISPOSITION FACTORSDocument35 pagesAGE AND DRUG DISPOSITION FACTORSMalueth AnguiNo ratings yet
- Pregnancy & BreastfeedingDocument27 pagesPregnancy & BreastfeedingRobert Selvin MNo ratings yet
- Reproductive PharmacologyDocument3 pagesReproductive PharmacologyNamarNo ratings yet
- Interaksi Farmakokinetika DistribusiDocument3 pagesInteraksi Farmakokinetika DistribusijessicaNo ratings yet
- Individualization of Drug Dosage RegimenDocument34 pagesIndividualization of Drug Dosage RegimenPreethi Iyengar86% (7)
- 256 FullDocument7 pages256 FullAngga M RahmanNo ratings yet
- Drogas Embarazo y LactanciaDocument7 pagesDrogas Embarazo y LactanciaReyna HernándezNo ratings yet
- Drug Therapy in Neonates & InfantsDocument19 pagesDrug Therapy in Neonates & InfantsPearlNo ratings yet
- PEAK Drug Therapy During Pregnancy Implications For Dental PracticeDocument8 pagesPEAK Drug Therapy During Pregnancy Implications For Dental PracticeAmalia KautsariaNo ratings yet
- Pharmacokinetic in Pediatrics: and Implications For Drug TherapyDocument35 pagesPharmacokinetic in Pediatrics: and Implications For Drug TherapyW MegaNo ratings yet
- Pharmacokinetics in Special PopulationsDocument26 pagesPharmacokinetics in Special PopulationsAnkita banerjeeNo ratings yet
- 565-Article Text-2680-1-10-20230702Document7 pages565-Article Text-2680-1-10-20230702Yosep SembiringNo ratings yet
- Drug Used in Pregnancy (Autosaved)Document27 pagesDrug Used in Pregnancy (Autosaved)AlizaNo ratings yet
- Obat Pada Bayi Dan AnakDocument47 pagesObat Pada Bayi Dan AnakBrama AtmajaNo ratings yet
- Pharmacokinetics in PregnancyDocument10 pagesPharmacokinetics in PregnancyCyrel Alexandra I. DiolazoNo ratings yet
- Therapeutic Drug Monitoring Principles in The Neonate: Gideon KorenDocument6 pagesTherapeutic Drug Monitoring Principles in The Neonate: Gideon KorenGül BaktırNo ratings yet
- Drug Use During Pregnancy and LactationDocument93 pagesDrug Use During Pregnancy and Lactation2012100% (2)
- Age KineticsDocument73 pagesAge KineticstiruchanurNo ratings yet
- Drug Use During Pregnancy and LactationDocument45 pagesDrug Use During Pregnancy and LactationSayli GoreNo ratings yet
- Definitions: - PharmacokineticsDocument31 pagesDefinitions: - PharmacokineticsmebibegNo ratings yet
- Drugs in Pregnancy and LactationDocument7 pagesDrugs in Pregnancy and LactationAdria DiamanteNo ratings yet
- Trabajo Farmaco Quinto.Document4 pagesTrabajo Farmaco Quinto.sebastian yanezNo ratings yet
- Impact of the Intrauterine Environment on Future HealthDocument19 pagesImpact of the Intrauterine Environment on Future HealthAliNo ratings yet
- Changes in Maternal Physiology and Metabolism During Pregnancy Hormonal ChangesDocument9 pagesChanges in Maternal Physiology and Metabolism During Pregnancy Hormonal ChangesMuh AfdholNo ratings yet
- K-19 Obat-Obat Dalam Masa KehamilanDocument31 pagesK-19 Obat-Obat Dalam Masa KehamilanChristian Lumban GaolNo ratings yet
- Opioids A ReviewDocument19 pagesOpioids A ReviewAlan padilla sesma100% (1)
- Clinical Pharmacokinetics and Pharmacodynamics of Opioid Analgesics in Infants and ChildrenDocument20 pagesClinical Pharmacokinetics and Pharmacodynamics of Opioid Analgesics in Infants and ChildrenmaryNo ratings yet
- Variability in Drug ResponseDocument18 pagesVariability in Drug Responsehlouis8No ratings yet
- Drug InteractionsDocument43 pagesDrug InteractionsNinaNo ratings yet
- Pharmacokinetics in Pregnancy 1: Matthew Dawes Philip J. ChowienczykDocument8 pagesPharmacokinetics in Pregnancy 1: Matthew Dawes Philip J. ChowienczykNandini GujjariNo ratings yet
- PXI Express Chassis 14/18-Slot Rack Mount Kits: Installation GuideDocument4 pagesPXI Express Chassis 14/18-Slot Rack Mount Kits: Installation GuideDomenico DomyNo ratings yet
- A New Approach To The Deposition of Elemental Boron and Boron-Based Coatings by Pulsed Magnetron Sputtering of Loosely Packed Boron Powder TargetsDocument6 pagesA New Approach To The Deposition of Elemental Boron and Boron-Based Coatings by Pulsed Magnetron Sputtering of Loosely Packed Boron Powder TargetsyouamareNo ratings yet
- Parenteral Fluid Therapy: Types of Intravenous SolutionDocument18 pagesParenteral Fluid Therapy: Types of Intravenous SolutionKathleen Joy Costales Magtanong100% (1)
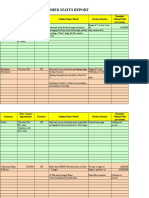
- Customer Status Update Report 27th January 2015 ColourDocument20 pagesCustomer Status Update Report 27th January 2015 ColourmaryNo ratings yet
- L&T Type 2 Co-Ordination Selection ChartsDocument48 pagesL&T Type 2 Co-Ordination Selection Chartsrdeepak99100% (7)
- Section 6 - Diagnostic ProceduresDocument13 pagesSection 6 - Diagnostic Proceduresanon_152488453100% (1)
- Herbivoría y Cristales de CaOxDocument33 pagesHerbivoría y Cristales de CaOxBrain LongwoodNo ratings yet
- Woody Plant Seed Manual - CompleteDocument1,241 pagesWoody Plant Seed Manual - CompleteJonas Sandell100% (1)
- European Commission: The Traineeships OfficeDocument3 pagesEuropean Commission: The Traineeships Officenasrine hachimNo ratings yet
- Program Pakan Budidaya Lele: Farm Pond Code AREA (m2) Stocking Date Stocking Amount DensityDocument6 pagesProgram Pakan Budidaya Lele: Farm Pond Code AREA (m2) Stocking Date Stocking Amount DensityChevienrenaldy SamsuNo ratings yet
- Approximate Methods For The Estimation of Muskingum Flood Routing ParametersDocument12 pagesApproximate Methods For The Estimation of Muskingum Flood Routing Parameterssherif ashrafNo ratings yet
- Creative 2nd QuarterDocument6 pagesCreative 2nd QuarterJanice CordovaNo ratings yet
- PhotosynthesisDocument30 pagesPhotosynthesisAngela CanlasNo ratings yet
- The DriversDocument277 pagesThe DriversADENIKE JOHNSONNo ratings yet
- Coding deCoding class insightsDocument18 pagesCoding deCoding class insightsShalabh Vikram SahuNo ratings yet
- Y10 ICT End of TermDocument7 pagesY10 ICT End of TermIvy Atuhairwe BisoborwaNo ratings yet
- BIG-IP Access Policy Manager CustomizationDocument118 pagesBIG-IP Access Policy Manager CustomizationDhananjai SinghNo ratings yet
- Social Responsibility and Managerial Ethics (Principles of Management)Document35 pagesSocial Responsibility and Managerial Ethics (Principles of Management)Reader94% (16)
- Boutique HotelsDocument61 pagesBoutique Hotelsnour alkhateeb100% (1)
- ClinicalOpiateWithdrawalScale PDFDocument2 pagesClinicalOpiateWithdrawalScale PDFRajamanitiNo ratings yet
- Unit 14 Food Storage: StructureDocument13 pagesUnit 14 Food Storage: StructureRiddhi KatheNo ratings yet
- Valvula Contrabalance CBV1 10 S O A 30Document21 pagesValvula Contrabalance CBV1 10 S O A 30Judith Daza SilvaNo ratings yet
- The Biology of Vascular Epiphytes Zotz 2016 PDFDocument292 pagesThe Biology of Vascular Epiphytes Zotz 2016 PDFEvaldo Pape100% (1)
- Kma 252 Exam 18 NewstyleDocument19 pagesKma 252 Exam 18 NewstyleSebin GeorgeNo ratings yet
- Karsten Fatur - "Sagas of The Solanaceae: Speculative Ethnobotanical Perspectives On The Norse Berserkers" (2019)Document8 pagesKarsten Fatur - "Sagas of The Solanaceae: Speculative Ethnobotanical Perspectives On The Norse Berserkers" (2019)Before AfterNo ratings yet
- Comparatives Board GameDocument2 pagesComparatives Board GameNathalie Alejandra Patiño LópezNo ratings yet
- Vehicle Speed Control Using RF CommunicationDocument20 pagesVehicle Speed Control Using RF CommunicationRaina John100% (2)
- ResearchDocument44 pagesResearchGwend MemoracionNo ratings yet
- TZMmanual PDFDocument8 pagesTZMmanual PDFccardenas3907No ratings yet
- Cardio Fitt Pin PostersDocument5 pagesCardio Fitt Pin Postersapi-385952225No ratings yet