You might also like
- Necropsy - Killer Whale NootkaDocument5 pagesNecropsy - Killer Whale NootkaThe Orca Project Corp100% (2)
- Past History. - The Physical Examination - Physical: Harry J - Cohen, and Paul J - Caivieron, New York, N. YDocument4 pagesPast History. - The Physical Examination - Physical: Harry J - Cohen, and Paul J - Caivieron, New York, N. YReza Alfitra MutiaraNo ratings yet
- Presenter: Dr. Nayana Senger Moderator: Dr. Santosh KumarDocument53 pagesPresenter: Dr. Nayana Senger Moderator: Dr. Santosh Kumarnaveena reddyNo ratings yet
- Kidney and Urinary System Anatomy&PhysiologyDocument52 pagesKidney and Urinary System Anatomy&PhysiologyAnonymous KsxN7vIQxbNo ratings yet
- PELVIC INJURIESDocument4 pagesPELVIC INJURIESAhmadNassrNo ratings yet
- Necropsy - Killer Whale ShawnDocument8 pagesNecropsy - Killer Whale ShawnThe Orca Project Corp100% (4)
- Understanding Pelvic Pain Through Basic NeuroanatomyDocument9 pagesUnderstanding Pelvic Pain Through Basic NeuroanatomyEladio García DelaMorenaNo ratings yet
- Abdominal PainDocument15 pagesAbdominal PainLina E. ArangoNo ratings yet
- The Biology of Emergency Medicine. JACEP. 1979 - 8-280-3Document4 pagesThe Biology of Emergency Medicine. JACEP. 1979 - 8-280-3Kenya Nicole CosteNo ratings yet
- Surgical Endoscopy: Laparoscopic Repair of Congenital Diaphragmatic Hernia in A 6-Month-Old ChildDocument3 pagesSurgical Endoscopy: Laparoscopic Repair of Congenital Diaphragmatic Hernia in A 6-Month-Old ChildApple IdeaNo ratings yet
- Treatment During Menstruation: .MtdressDocument2 pagesTreatment During Menstruation: .MtdressErik MirandaNo ratings yet
- Menstrual Edema With Intracranial Hypertension (Pseudotumor Cerebri)Document11 pagesMenstrual Edema With Intracranial Hypertension (Pseudotumor Cerebri)Pramudi DarmawanNo ratings yet
- Pulpitis AcutaDocument42 pagesPulpitis Acutajanko_ana100% (1)
- Getting The Support You Need.20140708.114148Document2 pagesGetting The Support You Need.20140708.114148bengalmenu9No ratings yet
- Notes On Anesthesia: Shywans - Surgeons Columbia University, New YorkDocument36 pagesNotes On Anesthesia: Shywans - Surgeons Columbia University, New Yorkmarina_shawkyNo ratings yet
- Differential Diagnosis DiscussionDocument13 pagesDifferential Diagnosis Discussionpriya sasirekhaNo ratings yet
- Communication Skills ExplainingDocument3 pagesCommunication Skills Explaining22Alyss22No ratings yet
- Journals J-Neurosurg 22 5 Article-p465-PreviewDocument2 pagesJournals J-Neurosurg 22 5 Article-p465-PreviewNiswaNo ratings yet
- Bedah. Apendisitis DR HerryDocument36 pagesBedah. Apendisitis DR HerryAnisa DoankNo ratings yet
- Approach To Acute Abdominal Pain: Robert Mcnamara,, Anthony J. DeanDocument15 pagesApproach To Acute Abdominal Pain: Robert Mcnamara,, Anthony J. DeanNataly VanesaNo ratings yet
- Specifics in Hom (EopathyDocument2 pagesSpecifics in Hom (EopathySohail LatifNo ratings yet
- Primary Review: Psoas Abscess: Case of The LiteratureDocument3 pagesPrimary Review: Psoas Abscess: Case of The LiteratureDung Tran HoangNo ratings yet
- Pelvis Perineum Cases 04Document5 pagesPelvis Perineum Cases 04Uloko ChristopherNo ratings yet
- Nerve Nerve Nerve Nerve Entrapment Entrapment Syndromes (Nes) Syndromes (Nes)Document52 pagesNerve Nerve Nerve Nerve Entrapment Entrapment Syndromes (Nes) Syndromes (Nes)teshaleNo ratings yet
- EMRAP 2018 06 June Vol.18Document20 pagesEMRAP 2018 06 June Vol.18DrewChapmanNo ratings yet
- Spondilitis TB - Canny Denny - Stase RMDocument13 pagesSpondilitis TB - Canny Denny - Stase RMAnonymous U9KX2cMNo ratings yet
- Anesthesia Notes on Respiration and Airway ObstructionDocument36 pagesAnesthesia Notes on Respiration and Airway ObstructionAnil SathyadasNo ratings yet
- Necropsy - Killer Whale KilroyDocument10 pagesNecropsy - Killer Whale KilroyThe Orca Project Corp100% (1)
- Unit13 Anatomy MCQsDocument50 pagesUnit13 Anatomy MCQsAsadullah Yousafzai100% (2)
- Long-Term Results of Lateral Internal Sphincterotomy For Chronic Anal Fissure With Particular Reference To Incidence of Fecal IncontinenceDocument5 pagesLong-Term Results of Lateral Internal Sphincterotomy For Chronic Anal Fissure With Particular Reference To Incidence of Fecal IncontinenceMetin AzaNo ratings yet
- Jama 1898 72440590004001aDocument5 pagesJama 1898 72440590004001aNilsonMarianoFilhoNo ratings yet
- Ściąga AnfDocument1 pageŚciąga AnfKasia ManżukNo ratings yet
- Louis Kuhne - Facial Diagnosis (1897)Document105 pagesLouis Kuhne - Facial Diagnosis (1897)Școala Solomonară / The Solomonary School100% (2)
- A Mistaken Case of Tension Pneumothorax: Michael Joseph NewmanDocument4 pagesA Mistaken Case of Tension Pneumothorax: Michael Joseph NewmanAmalia FirdhaNo ratings yet
- Case Study DoneDocument4 pagesCase Study DoneYash RamawatNo ratings yet
- Hernia Uterine Inguinale: An Uncommon Cause of Pelvic Pain in The Adult Female PatientDocument4 pagesHernia Uterine Inguinale: An Uncommon Cause of Pelvic Pain in The Adult Female PatientJeje MoNo ratings yet
- Brain and lung injuries comparedDocument1 pageBrain and lung injuries comparedAgungBudiPamungkasNo ratings yet
- AdvancedSuggestionNeuroinduction 10284212Document419 pagesAdvancedSuggestionNeuroinduction 10284212jurebieNo ratings yet
- Louis Kuhne - Facial Diagnosis (1897)Document105 pagesLouis Kuhne - Facial Diagnosis (1897)Școala Solomonară / The Solomonary School100% (6)
- Case Report: Perforated Duodenal Diverticulum With Subtle Pneumoretroperitoneum On Abdominal X-RayDocument4 pagesCase Report: Perforated Duodenal Diverticulum With Subtle Pneumoretroperitoneum On Abdominal X-RayNoviaRiadyNo ratings yet
- Protocol - Lymphangioleiomyomatosis (HCC 02242023)Document15 pagesProtocol - Lymphangioleiomyomatosis (HCC 02242023)Brian OlajeNo ratings yet
- Pt. Name: A.J.C Age: 65 Sex: M Date of Birth: October 22, 1953 Pre-Operation Diagnosis: Indirect Inguinal Hernia, Left, Reducible Incomplete Operation Perform: Mesh Hernioplasty LeftDocument16 pagesPt. Name: A.J.C Age: 65 Sex: M Date of Birth: October 22, 1953 Pre-Operation Diagnosis: Indirect Inguinal Hernia, Left, Reducible Incomplete Operation Perform: Mesh Hernioplasty LeftEden Marie FranciscoNo ratings yet
- The Dangers of Going To BedDocument2 pagesThe Dangers of Going To BedtheintrepiddodgerNo ratings yet
- Durai 2009Document1 pageDurai 2009indrimeiriskaNo ratings yet
- ArticleDocument3 pagesArticleИванАтанасовNo ratings yet
- Raglands Adrenal Test PDFDocument5 pagesRaglands Adrenal Test PDFwxcvbnnbvcxwNo ratings yet
- Grawitz TumorDocument3 pagesGrawitz TumorIrma D'amoreNo ratings yet
- Pedsinreview 2021005196Document4 pagesPedsinreview 2021005196Claudio MontiNo ratings yet
- ConservativeDocument4 pagesConservativeRifky Budi TriyatnoNo ratings yet
- BCR 2021 246101Document4 pagesBCR 2021 246101chidiebere peter echiehNo ratings yet
- Benefits of Sarvangasana Pose and Its VariationsDocument4 pagesBenefits of Sarvangasana Pose and Its VariationsTest4DNo ratings yet
- Temporal Sphenoidal Line: T4 Gall BladderDocument3 pagesTemporal Sphenoidal Line: T4 Gall Bladdertaichi7No ratings yet
- SpA Axial NEJMDocument12 pagesSpA Axial NEJMSofia SimpertigueNo ratings yet
- Supra Spin at UsDocument3 pagesSupra Spin at UsmarindadaNo ratings yet
- Jurnal THTDocument46 pagesJurnal THTShida ZakariaNo ratings yet
- A Treatise on the Incubus, or Night-Mare, Disturbed Sleep, Terrific Dreams and Nocturnal VisionsFrom EverandA Treatise on the Incubus, or Night-Mare, Disturbed Sleep, Terrific Dreams and Nocturnal VisionsNo ratings yet
- Were TheDocument2 pagesWere TheivanNo ratings yet
- Annals of Emergency Medicine Volume 27 Issue 4 1996 (Doi 10.1016 - s0196-0644 (96) 70229-9) William H Cordell - Renal ColicDocument3 pagesAnnals of Emergency Medicine Volume 27 Issue 4 1996 (Doi 10.1016 - s0196-0644 (96) 70229-9) William H Cordell - Renal ColicivanNo ratings yet
- Abstracts: 1 4 8 / 1 5 2 1 Annals of Emergency Medicine 2 1: 1 2 December 1992Document1 pageAbstracts: 1 4 8 / 1 5 2 1 Annals of Emergency Medicine 2 1: 1 2 December 1992ivanNo ratings yet
- BiomolBiomed Manuscript TemplateDocument10 pagesBiomolBiomed Manuscript TemplateivanNo ratings yet
- Passmedicine Mcqs-Surgical and Musculoskeletal ProblemsDocument346 pagesPassmedicine Mcqs-Surgical and Musculoskeletal ProblemsMohammad Saleh100% (1)
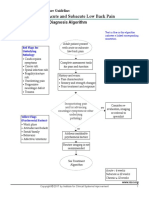
- Jurnal Low Back Pain PDFDocument5 pagesJurnal Low Back Pain PDFFikar AxlrosesNo ratings yet
- Trauma and OrthopedicsDocument134 pagesTrauma and OrthopedicsAdebisiNo ratings yet
- Mulligan Mobilization Versus Stretching On The Management of Piriformis Syndrome A Comparative StudyDocument6 pagesMulligan Mobilization Versus Stretching On The Management of Piriformis Syndrome A Comparative StudyInternational Journal of PhysiotherapyNo ratings yet
- Caudal Epidural InjectionDocument6 pagesCaudal Epidural InjectionRS BaptisNo ratings yet
- 12 Physical Education CH 3 Yoga Lifestyle PDFDocument8 pages12 Physical Education CH 3 Yoga Lifestyle PDFSaumyaNo ratings yet
- Core Stability Origins and FunctionDocument4 pagesCore Stability Origins and FunctionWhisperer BowenNo ratings yet
- Bogduk 2009Document3 pagesBogduk 2009Borys100% (1)
- Clinical Rheumatology by Rohini HandaDocument7 pagesClinical Rheumatology by Rohini HandaMafe CastroNo ratings yet
- Subacute Low Back PainDocument49 pagesSubacute Low Back Painsayid najibullahNo ratings yet
- Yamamoto New Scalp AcupunctureDocument4 pagesYamamoto New Scalp AcupunctureMaria Agustina Flores de Seguela100% (1)
- Correct Gua Sha Sequence and TechniqueDocument36 pagesCorrect Gua Sha Sequence and TechniqueNilton Benfatti100% (10)
- Risk Factors of Low Back Pain Among Filipino Male Air-Conditioned Bus DriversDocument67 pagesRisk Factors of Low Back Pain Among Filipino Male Air-Conditioned Bus DriversyajtripackNo ratings yet
- Minor Ailments During PregnancyDocument47 pagesMinor Ailments During PregnancyDiablo GoliathNo ratings yet
- Low Back Pain Anatomy, Imaging, and DiagnosisDocument67 pagesLow Back Pain Anatomy, Imaging, and DiagnosiswildanmalikNo ratings yet
- Ayurveda BrochureDocument9 pagesAyurveda BrochurePartheebanNo ratings yet
- 15 - Peripheral Neurology of The Lower LimbDocument15 pages15 - Peripheral Neurology of The Lower Limbdaacad muuminNo ratings yet
- Opposition To Motion For Sanctions Under Rule 11 Thomas Keenan Vs Beyel Brothers Inc PDFDocument12 pagesOpposition To Motion For Sanctions Under Rule 11 Thomas Keenan Vs Beyel Brothers Inc PDFmbellvue100% (1)
- Ankylosing Spondylitis and HomoeopathyDocument12 pagesAnkylosing Spondylitis and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Office Furniture Design According To A Human Anthropometric DataDocument6 pagesOffice Furniture Design According To A Human Anthropometric DataarchinmayNo ratings yet
- Introduction to the Life Energy System and Tuning Fork TherapyDocument8 pagesIntroduction to the Life Energy System and Tuning Fork TherapyAngel Malzone100% (1)
- Indonesian Rheumatology Association Recommendations for Diagnosis and Management of Axial Spondyloarthritis 2021Document15 pagesIndonesian Rheumatology Association Recommendations for Diagnosis and Management of Axial Spondyloarthritis 2021Rahmanu ReztaputraNo ratings yet
- P - R Saq Summary Jeff 2019Document12 pagesP - R Saq Summary Jeff 2019Nick-Hugh Sean WisdomNo ratings yet
- Revision 1.Document9 pagesRevision 1.Sebayari RiosNo ratings yet
- Thusharalal ThesisDocument238 pagesThusharalal ThesisPankaj SinghNo ratings yet
- 9 The Stretching Debate'Document2 pages9 The Stretching Debate'АлексNo ratings yet
- PEMF Therapy For Pain and InflammationDocument21 pagesPEMF Therapy For Pain and InflammationPhilNo ratings yet
- Torticolis OdtDocument25 pagesTorticolis OdtAndreea CimpoiNo ratings yet
- Publicity - Materials ISCP Booklet PDFDocument14 pagesPublicity - Materials ISCP Booklet PDFcarlosfisioNo ratings yet
- Spinous Process Tenderness Syndrome - A Newly Discovered DisorderDocument2 pagesSpinous Process Tenderness Syndrome - A Newly Discovered DisorderMichele MarengoNo ratings yet