You might also like
- Running Head: Protein-Energy Malnutrition 1 Protein-Energy Malnutrition Name Institution Professor Course DateDocument7 pagesRunning Head: Protein-Energy Malnutrition 1 Protein-Energy Malnutrition Name Institution Professor Course DateJackson KasakuNo ratings yet
- 13 SureDocument11 pages13 SureSamuel Kyei-BoatengNo ratings yet
- Nutrition and Maternal Neonatal and Child Heal - 2015 - Seminars in PerinatoloDocument14 pagesNutrition and Maternal Neonatal and Child Heal - 2015 - Seminars in PerinatoloVahlufi Eka putriNo ratings yet
- 2012, Fetal DevDocument23 pages2012, Fetal DevCorina IoanaNo ratings yet
- Chapter 12. Protein-Energy Malnutrition: Causes and EpidemiologyDocument14 pagesChapter 12. Protein-Energy Malnutrition: Causes and EpidemiologyIrma KurniawatiNo ratings yet
- The Effect of Micronutrient Deficiencies On Child Growth - A Review of Results From Community-Based Supplementation TrialsDocument11 pagesThe Effect of Micronutrient Deficiencies On Child Growth - A Review of Results From Community-Based Supplementation TrialsBrachim AnsariNo ratings yet
- Frequency of Malnutrition Among Children Under 2 Years and Its Relationship With Inadequate Breast Feeding PracticeDocument3 pagesFrequency of Malnutrition Among Children Under 2 Years and Its Relationship With Inadequate Breast Feeding PracticeAndhika SatriyaNo ratings yet
- Folic Acid: Influence On The Outcome of Pregnancy: Theresa O Scholl and William G JohnsonDocument9 pagesFolic Acid: Influence On The Outcome of Pregnancy: Theresa O Scholl and William G JohnsonKeylLaNo ratings yet
- Malnutrition: Practice EssentialsDocument12 pagesMalnutrition: Practice EssentialsDejavuRizalNo ratings yet
- Abed,+1114 Impacts+of+Dietary+Supplements+and+Nutrient Rich+Food+for+Pregnant+Women+on+Birth+Weight+in+Sugh+El Chmis Alkhoms+-+LiDocument8 pagesAbed,+1114 Impacts+of+Dietary+Supplements+and+Nutrient Rich+Food+for+Pregnant+Women+on+Birth+Weight+in+Sugh+El Chmis Alkhoms+-+LiLydia LuciusNo ratings yet
- JFMK 02 00030Document10 pagesJFMK 02 00030wardahNo ratings yet
- Aspectos Importantes de La Nutrición en Niños Con CáncerDocument11 pagesAspectos Importantes de La Nutrición en Niños Con CáncerNadia DonosoNo ratings yet
- Kelompok 1 - Review ArtikelDocument14 pagesKelompok 1 - Review ArtikeladeliazettaNo ratings yet
- Lapkas Anak (Prof Dr. Hj. Bidasari)Document74 pagesLapkas Anak (Prof Dr. Hj. Bidasari)Maral Bimanti Febrilina100% (1)
- Weaning Foods 2006 PDFDocument25 pagesWeaning Foods 2006 PDFmaria ulfaNo ratings yet
- Improving Prenatal Nutrition in Developing CountriesDocument5 pagesImproving Prenatal Nutrition in Developing CountriesBenbelaNo ratings yet
- Adolescent Pregnancy and NutritionDocument7 pagesAdolescent Pregnancy and NutritioncaroNo ratings yet
- Nutrition (Micronutrients) in Child Growth and Development: A Systematic Review On Current Evidence, Recommendations and Opportunities For Further ResearchDocument15 pagesNutrition (Micronutrients) in Child Growth and Development: A Systematic Review On Current Evidence, Recommendations and Opportunities For Further ResearchRiley RilanNo ratings yet
- Malnutrition in Hospitalized ChildrenDocument5 pagesMalnutrition in Hospitalized ChildrenPutri Wulan SukmawatiNo ratings yet
- Navigating The Clinical Landscape of Severe Acute Malnutrition in India's Pediatric DemographicDocument10 pagesNavigating The Clinical Landscape of Severe Acute Malnutrition in India's Pediatric DemographicInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 2015 Embryos, DOHaD and David BarkerDocument7 pages2015 Embryos, DOHaD and David BarkerNguyễn Tiến HồngNo ratings yet
- 184-Article Text - 797-1-10-20151013Document5 pages184-Article Text - 797-1-10-20151013Bushra KainaatNo ratings yet
- Malnutrition PaperDocument10 pagesMalnutrition PaperSilma Safira IhyaNo ratings yet
- Wallace2021Document13 pagesWallace2021Ena EppirtaNo ratings yet
- Nutrients 15 02311Document14 pagesNutrients 15 02311Fauziah Furqanah SyamNo ratings yet
- Nutritional Requirements OverviewDocument6 pagesNutritional Requirements OverviewKoriaNo ratings yet
- Referencia 7. Santander 2021Document30 pagesReferencia 7. Santander 2021Erie RegaladoNo ratings yet
- Nutritional Support in Critically Ill Pediatric PatientDocument29 pagesNutritional Support in Critically Ill Pediatric PatientVibin K vNo ratings yet
- Diabetes in Pregnancy: The Complete Guide to ManagementFrom EverandDiabetes in Pregnancy: The Complete Guide to ManagementLisa E. MooreNo ratings yet
- Chapter 2Document7 pagesChapter 2Mick MickeyNo ratings yet
- Office of The SecretaryDocument19 pagesOffice of The Secretarykiteli mendozaNo ratings yet
- Dm2020-0092 Interim Nutritional Guidelines For Women of Reproductive Age WRADocument9 pagesDm2020-0092 Interim Nutritional Guidelines For Women of Reproductive Age WRARiza Joy DABALOSNo ratings yet
- Articol Programare EpigeneticaDocument15 pagesArticol Programare EpigeneticaDiana-Elena ComandasuNo ratings yet
- Nutritional Status of Pregnant Women and Newborns in A Secondary Referral Health Care Setting of IndiaDocument16 pagesNutritional Status of Pregnant Women and Newborns in A Secondary Referral Health Care Setting of Indiaerin desweniNo ratings yet
- Endocrine Management PwsDocument10 pagesEndocrine Management PwsMohammad JoharNo ratings yet
- Obs PresentationDocument19 pagesObs PresentationAliNo ratings yet
- Iqbal. 2019. Zinc and Probiotic SupplementationDocument12 pagesIqbal. 2019. Zinc and Probiotic Supplementationintan wahyuNo ratings yet
- Black DKK, 2013Document25 pagesBlack DKK, 2013Yurina HirateNo ratings yet
- A S F C S: Nimal Ourced Oods and Hild TuntingDocument18 pagesA S F C S: Nimal Ourced Oods and Hild Tuntingchandra dewiNo ratings yet
- Vaccine: CommentaryDocument9 pagesVaccine: CommentaryJoseloNo ratings yet
- Nelson's Hour - 58-60Document51 pagesNelson's Hour - 58-60Josselle Sempio CalientaNo ratings yet
- Republic of The Philippines Tamag, Vigan City 2700 Ilocos SurDocument8 pagesRepublic of The Philippines Tamag, Vigan City 2700 Ilocos SurJewel Ramos GalinatoNo ratings yet
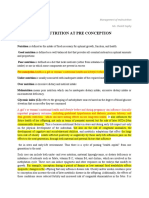
- Unit 2-Malnutrition at Pre ConceptionDocument9 pagesUnit 2-Malnutrition at Pre ConceptionSophy ChelotiNo ratings yet
- Nutrients: Acute Malnutrition in Children: Pathophysiology, Clinical EDocument9 pagesNutrients: Acute Malnutrition in Children: Pathophysiology, Clinical ERimNo ratings yet
- Malnutrition: Practice EssentialsDocument13 pagesMalnutrition: Practice EssentialsIda WilonaNo ratings yet
- Pack Alimentacion Clin in Perin 14Document194 pagesPack Alimentacion Clin in Perin 14Paz BustosNo ratings yet
- Cme Reviewarticle: Current Concepts of Maternal NutritionDocument14 pagesCme Reviewarticle: Current Concepts of Maternal NutritionAllan V. MouraNo ratings yet
- Nutritional Sta-WPS OfficeDocument8 pagesNutritional Sta-WPS OfficeAfolabi Horlarmilekan AbdulbasitNo ratings yet
- Update On Child Malnutrition Jan 2017Document31 pagesUpdate On Child Malnutrition Jan 2017AashnaNo ratings yet
- Amosu, A.M., Et Al.. A Study of The Nutritional Status of Under-5 Children of Low-Income EarnersDocument8 pagesAmosu, A.M., Et Al.. A Study of The Nutritional Status of Under-5 Children of Low-Income EarnersYayatRuslanNo ratings yet
- Adult Sequelae of Intrauterine Growth RestrictionDocument6 pagesAdult Sequelae of Intrauterine Growth RestrictionAnca AdamNo ratings yet
- Principles of Feeding The Preterm InfantDocument12 pagesPrinciples of Feeding The Preterm InfantPatrick nyawiraNo ratings yet
- The Epidemiology of Global Micronutrient Deficiencies by Regan Bailey Et AlDocument13 pagesThe Epidemiology of Global Micronutrient Deficiencies by Regan Bailey Et AlCecilia AcuinNo ratings yet
- TangDocument16 pagesTangEvelynNo ratings yet
- Safety and Efficacy of Supplements in Pregnancy: Lead ArticleDocument14 pagesSafety and Efficacy of Supplements in Pregnancy: Lead ArticleShahd AmjadNo ratings yet
- Research ReviewDocument4 pagesResearch ReviewLiikascypherNo ratings yet
- Nutrition During LactationDocument5 pagesNutrition During LactationAyesha Snbcan008No ratings yet
- Nursing Management: Nutritional Problems (Chapter 40) : MalnutritionDocument2 pagesNursing Management: Nutritional Problems (Chapter 40) : MalnutritionPrince K. TaileyNo ratings yet
- Practical Dietary Management of Protein Energy Malnutrition in Young Children With Cow's Milk Protein AllergyDocument8 pagesPractical Dietary Management of Protein Energy Malnutrition in Young Children With Cow's Milk Protein AllergyCarlos CuadrosNo ratings yet
- Effects of Cashew NutDocument9 pagesEffects of Cashew Nutsilvio da costa guerreiroNo ratings yet
- InflamaciónDocument12 pagesInflamaciónDaniNo ratings yet
- Wilson 2017Document13 pagesWilson 2017DaniNo ratings yet
- 1-S2.0-S0889159107000864-Main 12.03.12 P. M.Document6 pages1-S2.0-S0889159107000864-Main 12.03.12 P. M.DaniNo ratings yet
- Cambodia Tut CT SinusespdfDocument5 pagesCambodia Tut CT SinusespdfDaniNo ratings yet
- Echinococcosis: Key ConceptsDocument9 pagesEchinococcosis: Key ConceptsDaniNo ratings yet
- Etiology and Pathogenesis of Gout: Tanya J. Major Nicola DalbethDocument13 pagesEtiology and Pathogenesis of Gout: Tanya J. Major Nicola DalbethDaniNo ratings yet
- MainDocument8 pagesMainDaniNo ratings yet
- 1 s2.0 S0889159107000864 MainDocument8 pages1 s2.0 S0889159107000864 MainDaniNo ratings yet
- Academic Performance, Employment, and Sleep Health: A Comparison Between Working and Nonworking StudentsDocument12 pagesAcademic Performance, Employment, and Sleep Health: A Comparison Between Working and Nonworking StudentsDaniNo ratings yet
- Watercolor Company ProfileDocument50 pagesWatercolor Company ProfileDaniNo ratings yet
- Watercolor Company ProfileDocument50 pagesWatercolor Company ProfileDaniNo ratings yet
- Approaches To Glycemic Treatment Standards ofDocument14 pagesApproaches To Glycemic Treatment Standards ofGANA ABISHEKNo ratings yet
- Artículo #2Document12 pagesArtículo #2DaniNo ratings yet
- Artículo FormativaDocument4 pagesArtículo FormativaDaniNo ratings yet
- Coenzyme Q10 in Acute InfluenzaDocument7 pagesCoenzyme Q10 in Acute InfluenzaDaniNo ratings yet
- Preparing For The NASH Epidemic A Call To ActioDocument11 pagesPreparing For The NASH Epidemic A Call To ActioDaniNo ratings yet
- The Incidentally Discovered Adrenal Mass: Clinical PracticeDocument10 pagesThe Incidentally Discovered Adrenal Mass: Clinical PracticeDaniNo ratings yet
- Tugas Basing MandaDocument5 pagesTugas Basing MandaSalman AlfariziNo ratings yet
- Some Lower Bounds On The Reach of An Algebraic Variety: Chris La Valle Josué Tonelli-CuetoDocument9 pagesSome Lower Bounds On The Reach of An Algebraic Variety: Chris La Valle Josué Tonelli-CuetospanishramNo ratings yet
- Carte Tehnica Panou Fotovoltaic Cu Celule Policristaline Eging 250 WDocument1 pageCarte Tehnica Panou Fotovoltaic Cu Celule Policristaline Eging 250 WConstantin CilibiuNo ratings yet
- Project: Study On Building Construction Using Foam ConcreteDocument5 pagesProject: Study On Building Construction Using Foam ConcreteAzhagesanNo ratings yet
- Spare Parts Quotation For Scba & Eebd - 2021.03.19Document14 pagesSpare Parts Quotation For Scba & Eebd - 2021.03.19byhf2jgqprNo ratings yet
- April 2024 Daily Reading Learning Resource PDFDocument166 pagesApril 2024 Daily Reading Learning Resource PDFblackknight120mNo ratings yet
- 06 Story StiffnessDocument2 pages06 Story StiffnessDigvijay GiraseNo ratings yet
- Dumpy LevelDocument8 pagesDumpy LevelKhiel YumulNo ratings yet
- Psychosomatic DisordersDocument79 pagesPsychosomatic DisordersMONIKANo ratings yet
- CalaDocument13 pagesCalaMorris KwangwareNo ratings yet
- Fundamentals of Ship Maintenance and Repair For Future Marine Engineers PDFDocument11 pagesFundamentals of Ship Maintenance and Repair For Future Marine Engineers PDFShawn Wairisal100% (2)
- Nsejs Exam Solutions Paper 2019 PDFDocument27 pagesNsejs Exam Solutions Paper 2019 PDFMrinalini SinghNo ratings yet
- Anatomy-Head and NeckDocument94 pagesAnatomy-Head and NeckXahid IqbalNo ratings yet
- Class 10 Syllabus Breakup ChemistryDocument4 pagesClass 10 Syllabus Breakup ChemistryUmme AbdullahNo ratings yet
- Datasheet Continental ccp800 PDFDocument2 pagesDatasheet Continental ccp800 PDFKarni Aerospace Inc.No ratings yet
- MSDS Matrix Diluent-2 LISSDocument4 pagesMSDS Matrix Diluent-2 LISSLaboratorium RSI PekajanganNo ratings yet
- Lecture 1-5 EEEN323 March2022Document139 pagesLecture 1-5 EEEN323 March2022Lekono KagoNo ratings yet
- Relative Clauses - Revisión Del IntentoDocument4 pagesRelative Clauses - Revisión Del IntentoYordy Rodolfo Delgado RosarioNo ratings yet
- T 703Document4 pagesT 703Marcelo RojasNo ratings yet
- K-90-1900 FM-200 AgentDocument1 pageK-90-1900 FM-200 AgentPutra LangitNo ratings yet
- Plant InvitroDocument219 pagesPlant InvitroMD Nassima100% (4)
- CU50 Service ManualDocument30 pagesCU50 Service ManualjhalmarckNo ratings yet
- Nutella: Italian PronunciationDocument1 pageNutella: Italian PronunciationhbnjknwvnffkjrpaadttirvorgNo ratings yet
- Spare Parts: LKH Centrifugal PumpDocument20 pagesSpare Parts: LKH Centrifugal PumpService CTANo ratings yet
- Affiliated Institutions Anna University, Chennai Regulations - 2009 Curriculum Ii To Iv Semesters (Full Time) M.E. Applied ElectronicsDocument21 pagesAffiliated Institutions Anna University, Chennai Regulations - 2009 Curriculum Ii To Iv Semesters (Full Time) M.E. Applied ElectronicsRamya VNo ratings yet
- A 204Document1 pageA 204AnuranjanNo ratings yet
- 2414 2416 Installation ProcedureDocument4 pages2414 2416 Installation ProcedureJames BondNo ratings yet
- Bright: Insidecrochet - Co.ukDocument100 pagesBright: Insidecrochet - Co.ukЕкатерина Матушинец100% (2)
- Consumer Studies GR 11 Revision Term 1 2023 FinalDocument20 pagesConsumer Studies GR 11 Revision Term 1 2023 FinalCerboh MazibukoNo ratings yet
- Dangote Fertilizer Project NDT Analysis For U/G: Radiographic Test - Ultrasonic TestDocument6 pagesDangote Fertilizer Project NDT Analysis For U/G: Radiographic Test - Ultrasonic Testaakash100% (1)