You might also like
- Diagnostic Value of MRI-PDFF For Hepatic Steatosis in Patients With Non-Alcoholic Fatty Liver Disease: A Meta-AnalysisDocument10 pagesDiagnostic Value of MRI-PDFF For Hepatic Steatosis in Patients With Non-Alcoholic Fatty Liver Disease: A Meta-AnalysisNada Utami PrahastiwiNo ratings yet
- MMC 4Document26 pagesMMC 4M. PurnomoNo ratings yet
- Quantitative US For Noninvasive Assessment - USFFDocument9 pagesQuantitative US For Noninvasive Assessment - USFFLuciano AlvesNo ratings yet
- Precision Diagnostica y Confiabilidad Del Us en Higado GrasoDocument9 pagesPrecision Diagnostica y Confiabilidad Del Us en Higado GrasoDavidNo ratings yet
- ArtiiiiDocument26 pagesArtiiiiJenny CoronaNo ratings yet
- Ferraioli Et Al 2022 Us Attenuation For Liver Fat Quantification An Aium Rsna Qiba Pulse Echo Quantitative UltrasoundDocument12 pagesFerraioli Et Al 2022 Us Attenuation For Liver Fat Quantification An Aium Rsna Qiba Pulse Echo Quantitative UltrasoundThesisaurus IDNo ratings yet
- MRI PDFF in NASHDocument24 pagesMRI PDFF in NASHParul SoodNo ratings yet
- Diagnostic Value of Non Invasive Liver Function Tests in Liver Fibrosis and Changes in These Parameters Post Metabolic SurgeryDocument7 pagesDiagnostic Value of Non Invasive Liver Function Tests in Liver Fibrosis and Changes in These Parameters Post Metabolic SurgeryTan BulNo ratings yet
- Noninvasive Tests in The Assessment of NASH and NAFLD Fibrosis Now and Into The FutureDocument8 pagesNoninvasive Tests in The Assessment of NASH and NAFLD Fibrosis Now and Into The FutureRaeni Dwi PutriNo ratings yet
- Non-Invasive Diagnosis of NASH and NAFLDDocument17 pagesNon-Invasive Diagnosis of NASH and NAFLDRaeni Dwi PutriNo ratings yet
- BJR FOLFOX 6 DEBIRI Phase 2 TrialDocument7 pagesBJR FOLFOX 6 DEBIRI Phase 2 Trialpaquidermo85No ratings yet
- SWE in HAIDocument15 pagesSWE in HAIValentina IorgaNo ratings yet
- Secretin-Enhanced MRCP: Proceed With Cautious OptimismDocument4 pagesSecretin-Enhanced MRCP: Proceed With Cautious OptimismYuda FhunkshyangNo ratings yet
- Imaging Modalities in Pediatric Nafld: ReviewDocument9 pagesImaging Modalities in Pediatric Nafld: Reviewcitra annisa fitriNo ratings yet
- Drugs in Context: Rigorous - Rapid - ResponsiveDocument10 pagesDrugs in Context: Rigorous - Rapid - ResponsiveAkande AbdulazeezNo ratings yet
- Psa Persistentemente Elevado Post P RadicalDocument20 pagesPsa Persistentemente Elevado Post P RadicalBenjamin HuamanchauNo ratings yet
- BCSH Diagnosis and Management of PlasmacytomasDocument14 pagesBCSH Diagnosis and Management of PlasmacytomasEva YustianaNo ratings yet
- Evaluation of Liver Fibrosis and Cirrhosis On TheDocument7 pagesEvaluation of Liver Fibrosis and Cirrhosis On TheeugeniaNo ratings yet
- Favilla 2015Document2 pagesFavilla 2015DavorIvanićNo ratings yet
- Journal Pre-Proof: International Journal of Radiation Oncology, Biology, PhysicsDocument42 pagesJournal Pre-Proof: International Journal of Radiation Oncology, Biology, PhysicsMilan JovicNo ratings yet
- RPD 05072020Document4 pagesRPD 05072020api-478066704No ratings yet
- Metabolomic Profiling of Amoebic and Pyogenic Liver Abscesses An in Vitro NMR StudyDocument16 pagesMetabolomic Profiling of Amoebic and Pyogenic Liver Abscesses An in Vitro NMR Studysantosh091283No ratings yet
- Meta 1 - Zheng X - 2018Document9 pagesMeta 1 - Zheng X - 2018matheus.verasNo ratings yet
- Cancers 04 00549Document17 pagesCancers 04 00549pikkilirameshNo ratings yet
- Liver Transplantation - 2016 - Dioguardi Burgio - Correlation of Tumor Response On Computed Tomography With PathologicalDocument10 pagesLiver Transplantation - 2016 - Dioguardi Burgio - Correlation of Tumor Response On Computed Tomography With Pathologicaldahiheg756No ratings yet
- Non Invasve Marksers of Iver Fibrosis in NafldDocument3 pagesNon Invasve Marksers of Iver Fibrosis in NafldSvt Mscofficial2No ratings yet
- Reuter 2010Document8 pagesReuter 2010Hector Javier BurgosNo ratings yet
- Portec 2.Document8 pagesPortec 2.henryNo ratings yet
- The OncologistDocument7 pagesThe OncologistManunart FeungpeanNo ratings yet
- Kanker Serviks Hal 117-200Document84 pagesKanker Serviks Hal 117-200Khairina HerdaNo ratings yet
- Diagnostic Accuracy of FibroScan and Factors Affecting MeasurementsDocument11 pagesDiagnostic Accuracy of FibroScan and Factors Affecting MeasurementsRaeni Dwi PutriNo ratings yet
- Sorafenib in The Management of Metastatic Renal Cell CarcinomaDocument6 pagesSorafenib in The Management of Metastatic Renal Cell CarcinomaC Leite HendriyNo ratings yet
- Antifibrotic Therapies-EmergingDocument3 pagesAntifibrotic Therapies-EmergingVictor Hugo Campos SierraNo ratings yet
- Outcomes Following Different Thermal Ablation Strategies in Patients With Unresectable Colorectal Liver MetastaseDocument9 pagesOutcomes Following Different Thermal Ablation Strategies in Patients With Unresectable Colorectal Liver MetastaseNachchakorn DellNo ratings yet
- Using A Machine Learning Model To Risk Stratify For The Presence of Significant Liver Disease in A Primary Care PopulationDocument18 pagesUsing A Machine Learning Model To Risk Stratify For The Presence of Significant Liver Disease in A Primary Care Populationcerberus thanatosNo ratings yet
- The Physics of Radioembolization - 230807 - 113550Document27 pagesThe Physics of Radioembolization - 230807 - 113550seba gNo ratings yet
- Sequential Chemoradiotherapy With Gemcitabine and Cisplatin For Locoregionally Advanced Nasopharyngeal CarcinomaDocument9 pagesSequential Chemoradiotherapy With Gemcitabine and Cisplatin For Locoregionally Advanced Nasopharyngeal CarcinomadheaonyonNo ratings yet
- Clinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypeDocument12 pagesClinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypesilviailieNo ratings yet
- Journal of Photochemistry & Photobiology, B: BiologyDocument6 pagesJournal of Photochemistry & Photobiology, B: BiologyGabriel ŞarguNo ratings yet
- Semaglutide For The Treatment of Non Alcoholic Steatohepatitis Trial Design and Comparison of Non-Invasive BiomarkersDocument9 pagesSemaglutide For The Treatment of Non Alcoholic Steatohepatitis Trial Design and Comparison of Non-Invasive BiomarkersAntonio SalemeNo ratings yet
- Management of Urologic Cancer: Focal Therapy and Tissue PreservationFrom EverandManagement of Urologic Cancer: Focal Therapy and Tissue PreservationNo ratings yet
- 2012 - MemonDocument7 pages2012 - MemonmaryNo ratings yet
- Efficacy of EUS-RFA in Pancreatic Tumors: Is It Ready For Prime Time? A Systematic Review and Meta-AnalysisDocument9 pagesEfficacy of EUS-RFA in Pancreatic Tumors: Is It Ready For Prime Time? A Systematic Review and Meta-AnalysisRadinal MauludiNo ratings yet
- CLRRTDocument15 pagesCLRRTArturo ArturoNo ratings yet
- Octreosc Vs FDGDocument7 pagesOctreosc Vs FDGLaura PredescuNo ratings yet
- MDV 161Document12 pagesMDV 161rasika bhatNo ratings yet
- Likhitsup 2019Document7 pagesLikhitsup 2019jacky hariantoNo ratings yet
- Shearwave 17 12 11Document10 pagesShearwave 17 12 11Saritza MoleroNo ratings yet
- Robot Assisted Radical Cystectomy PDFDocument21 pagesRobot Assisted Radical Cystectomy PDFPierre Vivanco ZavalaNo ratings yet
- Livsey 2003Document6 pagesLivsey 2003Migue PerezNo ratings yet
- Nodal - Multi-Institut Oligo - Plus COREDocument13 pagesNodal - Multi-Institut Oligo - Plus COREsilviuNo ratings yet
- A Discovery of Screening Markers For Rheumatoid Arthritis byDocument10 pagesA Discovery of Screening Markers For Rheumatoid Arthritis byswamy cheekatlaNo ratings yet
- 1 s2.0 S2590280622000079 MainDocument10 pages1 s2.0 S2590280622000079 MainDimas Bintoro KyhNo ratings yet
- Surgical OncologyDocument9 pagesSurgical OncologyASONo ratings yet
- Perlemakan Hati Non-AlkoholikDocument5 pagesPerlemakan Hati Non-AlkoholikChristinaNo ratings yet
- Abdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceDocument8 pagesAbdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceWitrisyah PutriNo ratings yet
- Yi Luo Somascan Proteomics Identifies Serum BiomarkersDocument14 pagesYi Luo Somascan Proteomics Identifies Serum BiomarkersLaia BertranNo ratings yet
- Diagnosisofrenalcell Carcinoma: A Clinician'S PerspectiveDocument6 pagesDiagnosisofrenalcell Carcinoma: A Clinician'S PerspectiveGangsar DamaiNo ratings yet
- TSWJ2012 731089Document9 pagesTSWJ2012 731089samamansorNo ratings yet
- 1677 5538 Ibju 42 04 0694Document10 pages1677 5538 Ibju 42 04 0694Lucas VibiamNo ratings yet
- Referral - NAFLD in Primary CareDocument3 pagesReferral - NAFLD in Primary CareParul SoodNo ratings yet
- Mediterranean Diet & Physical Activity in NAFLDDocument3 pagesMediterranean Diet & Physical Activity in NAFLDParul SoodNo ratings yet
- Mechanism of NAFLD Dev & Therapeutic Strategies - Arun SanyalDocument15 pagesMechanism of NAFLD Dev & Therapeutic Strategies - Arun SanyalParul SoodNo ratings yet
- MRI Accuracy in Pediatric NAFLDDocument52 pagesMRI Accuracy in Pediatric NAFLDParul SoodNo ratings yet
- NAFLD in Asia 2019Document10 pagesNAFLD in Asia 2019Parul SoodNo ratings yet
- MRI PDFF in NASHDocument24 pagesMRI PDFF in NASHParul SoodNo ratings yet
- MRI & Liver Histology Features in NASHDocument17 pagesMRI & Liver Histology Features in NASHParul SoodNo ratings yet
- Non Invasive Imaging in NASHDocument3 pagesNon Invasive Imaging in NASHParul SoodNo ratings yet
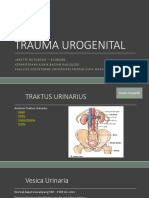
- Trauma UrogenitalDocument17 pagesTrauma UrogenitaljanetteNo ratings yet
- CcrnexamhandbookDocument42 pagesCcrnexamhandbookSpam SpazzamNo ratings yet
- Localized Dental Abrasion Caused by An Unusually Vicious Habit: Cases Report and Literature ReviewDocument8 pagesLocalized Dental Abrasion Caused by An Unusually Vicious Habit: Cases Report and Literature ReviewTheodora ComanNo ratings yet
- HerbalDocument4 pagesHerbalrocketwapNo ratings yet
- Urinary Bladder MassDocument2 pagesUrinary Bladder Masskarl de guzmanNo ratings yet
- Incident ReportDocument3 pagesIncident Reportthuynh12No ratings yet
- 4 SporozoaDocument42 pages4 SporozoaFranz SalazarNo ratings yet
- Pediatric Rheumatology CarteDocument628 pagesPediatric Rheumatology CarteCrischentian BrinzaNo ratings yet
- Occular Manifestations in Systemic DiseaseDocument42 pagesOccular Manifestations in Systemic DiseasekhalidNo ratings yet
- 2019 Preceptorship H N TNM Classification 8th Edition Jean Pascal MachielsDocument36 pages2019 Preceptorship H N TNM Classification 8th Edition Jean Pascal MachielsGalgalo GarbichaNo ratings yet
- Anaesthesiology Case (Kaarthigan)Document36 pagesAnaesthesiology Case (Kaarthigan)Kaarthigan RamaiahNo ratings yet
- HemoflagellatesDocument61 pagesHemoflagellatesMuhammad Nadhiev100% (1)
- DR Bhavini Sandip Shah Director: Microbiology Department of Microbiology Neuberg Supratech Labs AhmedabadDocument49 pagesDR Bhavini Sandip Shah Director: Microbiology Department of Microbiology Neuberg Supratech Labs Ahmedabadkrutarth shahNo ratings yet
- Asthma - FactsDocument24 pagesAsthma - Factsvsvp100No ratings yet
- Simulation Based Training For Anaesthesia ResidentsDocument8 pagesSimulation Based Training For Anaesthesia ResidentsSajal SahaNo ratings yet
- 43THYROID II 2021 ThyroiditisDocument29 pages43THYROID II 2021 ThyroiditisRaju ThapaNo ratings yet
- Skin and Soft Tissue InfectionsDocument8 pagesSkin and Soft Tissue InfectionsMARTIN REY EDRICK SANTOSNo ratings yet
- Vocabulary Work Book Check Your English Vocabulary For MedicineDocument50 pagesVocabulary Work Book Check Your English Vocabulary For MedicineMarius Belean100% (1)
- HAMP NCAL CompetencyModuleDocument47 pagesHAMP NCAL CompetencyModuleerlyNo ratings yet
- Urinary Catherization: St. Paul University Dumaguete College of Nursing Dumaguete City First Semester, 2021-2022Document9 pagesUrinary Catherization: St. Paul University Dumaguete College of Nursing Dumaguete City First Semester, 2021-2022Franz goNo ratings yet
- Hema I Chapter 12 - ESRDocument30 pagesHema I Chapter 12 - ESRTesfaNo ratings yet
- Hot Tub Mystery SolutionDocument2 pagesHot Tub Mystery Solutionkelsey100% (1)
- Rakesh SainiDocument4 pagesRakesh SainiAdarsh SonkarNo ratings yet
- Heart Volume Issue 2017 (Doi 10.1136 - Heartjnl-2017-312112) Ruwald, Martin H - Syncope andDocument3 pagesHeart Volume Issue 2017 (Doi 10.1136 - Heartjnl-2017-312112) Ruwald, Martin H - Syncope andZauzaNo ratings yet
- "First Time in History" - Cancer Vanishes For Every Patient in Drug TrialDocument3 pages"First Time in History" - Cancer Vanishes For Every Patient in Drug TrialDIPIN JAINNo ratings yet
- 120 HAAD Exam QuestionsDocument10 pages120 HAAD Exam QuestionsConsolacion Binarao Dolores50% (8)
- Quiet Time For Patients in Acute CareDocument24 pagesQuiet Time For Patients in Acute Careapi-354868439No ratings yet
- Wound Cleansing: Benefits of Hypochlorous AcidDocument5 pagesWound Cleansing: Benefits of Hypochlorous Acidlps DiamondNo ratings yet
- Techniques in Facial Fat Grafting PDFDocument7 pagesTechniques in Facial Fat Grafting PDFshininghmNo ratings yet
- Alcohol Withdrawal ManagemetnDocument1 pageAlcohol Withdrawal Managemetnericka0% (1)