You might also like
- A Practical Guide To Endodontic Access Cavity Preparation in Molar TeethDocument8 pagesA Practical Guide To Endodontic Access Cavity Preparation in Molar TeethAlireza RaieNo ratings yet
- A Practical Guide To Endodontic Access Cavity PrepDocument19 pagesA Practical Guide To Endodontic Access Cavity PrepRajeev GargNo ratings yet
- Borkar 2015Document6 pagesBorkar 2015Jing XueNo ratings yet
- Articol PivotDocument7 pagesArticol PivotDragos CiongaruNo ratings yet
- Endodontic Access Preparation The Tools For SuccessDocument9 pagesEndodontic Access Preparation The Tools For SuccessAna YUNo ratings yet
- Endodontic Surgery: Verifiable CPD PaperDocument10 pagesEndodontic Surgery: Verifiable CPD PaperSoal KoasNo ratings yet
- Access Cavity Part 2Document73 pagesAccess Cavity Part 2mrbyy619No ratings yet
- Intricate Internal Anatomy of Teeth and Its Clinical Significance in Endodontics - A ReviewDocument10 pagesIntricate Internal Anatomy of Teeth and Its Clinical Significance in Endodontics - A ReviewManjeevNo ratings yet
- FulltextDocument5 pagesFulltextaulia zahroNo ratings yet
- 107 Nonsurgical Endodontic Therapy of A Dens InvaginatusDocument3 pages107 Nonsurgical Endodontic Therapy of A Dens InvaginatusAurelian DentistNo ratings yet
- Guided Endodontic Access in A Maxillary Molar Using A Dynamic Navigation SystemDocument5 pagesGuided Endodontic Access in A Maxillary Molar Using A Dynamic Navigation SystemAlex KesumaNo ratings yet
- Endodontic Treatment of Curved Root Canal Systems PDFDocument3 pagesEndodontic Treatment of Curved Root Canal Systems PDFRăican AlexandruNo ratings yet
- Enhanced Retention of A Maxillofacial Prosthetic Obturator Using Precision Attachments: Two Case ReportsDocument6 pagesEnhanced Retention of A Maxillofacial Prosthetic Obturator Using Precision Attachments: Two Case ReportsAmalorNo ratings yet
- Restoring Proximal Caries Lesions Conservatively With Tunnel RestorationsDocument8 pagesRestoring Proximal Caries Lesions Conservatively With Tunnel RestorationsyesikaichaaNo ratings yet
- Rotational Path Removable Partial Denture DesignDocument7 pagesRotational Path Removable Partial Denture DesignNapatsorn RakpakwanNo ratings yet
- Endodontic Treatment of Mandibular Second Molar With Diversed Root Canal AnatomyDocument3 pagesEndodontic Treatment of Mandibular Second Molar With Diversed Root Canal AnatomyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Access Procedures:: Breaking and Entering Safely and EffectivelyDocument4 pagesAccess Procedures:: Breaking and Entering Safely and EffectivelyKalpanaNo ratings yet
- Clinical Case Reports - 2023 - Vyver - Apexification of Dens Evaginatus in A Mandibular Premolar A Case ReportDocument6 pagesClinical Case Reports - 2023 - Vyver - Apexification of Dens Evaginatus in A Mandibular Premolar A Case ReportIqra KhanNo ratings yet
- Jurnal KasusDocument4 pagesJurnal KasusDena SeptianiNo ratings yet
- Guided Endodontics for Complex Molar Cases with Calcified CanalsDocument7 pagesGuided Endodontics for Complex Molar Cases with Calcified CanalsJulia PimentelNo ratings yet
- Access Cavity PreparationDocument7 pagesAccess Cavity Preparationnorma paulina carcausto lipaNo ratings yet
- 116 Guidelines For Access CavityDocument8 pages116 Guidelines For Access CavityYodha AdityaNo ratings yet
- Preoperative Radiograph in Endodontics PDFDocument6 pagesPreoperative Radiograph in Endodontics PDFZain AlnahamNo ratings yet
- EMI. Khademi, ClarkDocument11 pagesEMI. Khademi, ClarkMaGe IsTeNo ratings yet
- Chapter 27Document115 pagesChapter 27dorin_1992No ratings yet
- Endodontic Treatment of Mandibular Premolars With Complex Anatomy Case SeriesDocument5 pagesEndodontic Treatment of Mandibular Premolars With Complex Anatomy Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Maxillary Second Molar With Four Roots and Five Canals: SciencedirectDocument5 pagesMaxillary Second Molar With Four Roots and Five Canals: SciencedirectKanish AggarwalNo ratings yet
- Root Perforations: Aetiology, Management Strategies and Outcomes. The Hole TruthDocument10 pagesRoot Perforations: Aetiology, Management Strategies and Outcomes. The Hole TruthGladis Aprilla RizkiNo ratings yet
- Case Report EndodonticsDocument49 pagesCase Report EndodonticsFrancis PrathyushaNo ratings yet
- Asalaam Alekkum: DR Gaurav Garg, Lecturer College of Dentistry, Al Zulfi, MUDocument57 pagesAsalaam Alekkum: DR Gaurav Garg, Lecturer College of Dentistry, Al Zulfi, MUMaGe IsTeNo ratings yet
- Endodontic Managementof Fourrootedpremolar JCD2013Document4 pagesEndodontic Managementof Fourrootedpremolar JCD2013Lucas PeixotoNo ratings yet
- Limitations-and-Management-of-Dynamic-Navigation-SDocument10 pagesLimitations-and-Management-of-Dynamic-Navigation-SchannadrasmaNo ratings yet
- 31 Ijss Nov cr02 - 2018Document4 pages31 Ijss Nov cr02 - 2018RAfii KerenNo ratings yet
- Adts Guidelines For Access CavityDocument9 pagesAdts Guidelines For Access CavityOmuraiNo ratings yet
- IJEDe 16 01 ScolavinoPaolone 722 3Document24 pagesIJEDe 16 01 ScolavinoPaolone 722 3Mauri EsnaNo ratings yet
- Telescopic Overdenture: A Case Report: C. S. Shruthi, R. Poojya, Swati Ram, AnupamaDocument5 pagesTelescopic Overdenture: A Case Report: C. S. Shruthi, R. Poojya, Swati Ram, AnupamaRani PutriNo ratings yet
- Endodontic Cavity PreparationDocument166 pagesEndodontic Cavity Preparationagusaranp0% (1)
- Tooth-Support Over Dentures: An Approach To Preventive ProsthodonticsDocument5 pagesTooth-Support Over Dentures: An Approach To Preventive ProsthodonticsAdvanced Research PublicationsNo ratings yet
- Oke 4Document3 pagesOke 4Maika RatriNo ratings yet
- Endodontic AccessDocument5 pagesEndodontic AccessShyambhavi SrivastavaNo ratings yet
- Articulo de Endodoncia PDFDocument14 pagesArticulo de Endodoncia PDFJuan Pablo Rondon OyuelaNo ratings yet
- Endo PDFDocument91 pagesEndo PDFPolo RalfNo ratings yet
- Access Procedures: Tips for Safe and Effective Root Canal EntryDocument4 pagesAccess Procedures: Tips for Safe and Effective Root Canal EntryMonica Ioana TeodorescuNo ratings yet
- Managing Missing Mandibular PremolarsDocument4 pagesManaging Missing Mandibular PremolarsKanish AggarwalNo ratings yet
- Endoguide 5676Document5 pagesEndoguide 5676Ruchi ShahNo ratings yet
- Endodontic and Restorative Management of A Lower Molar With A Calcified Pulp Chamber.Document7 pagesEndodontic and Restorative Management of A Lower Molar With A Calcified Pulp Chamber.Nicolas SantanderNo ratings yet
- Int Endodontic J - 2022 - Clauder - Present Status and Future Directions Managing PerforationsDocument20 pagesInt Endodontic J - 2022 - Clauder - Present Status and Future Directions Managing Perforationsjorge2412No ratings yet
- A P A O F S: Ndodontic Ccess Reparation N Pening OR UccessDocument7 pagesA P A O F S: Ndodontic Ccess Reparation N Pening OR UccessHadil AltilbaniNo ratings yet
- 10 1016@j Joen 2020 11 002Document22 pages10 1016@j Joen 2020 11 002alondraNo ratings yet
- An Alternative Solution For A Complex Prosthodontic Problem: A Modified Andrews Fixed Dental ProsthesisDocument5 pagesAn Alternative Solution For A Complex Prosthodontic Problem: A Modified Andrews Fixed Dental ProsthesisDragos CiongaruNo ratings yet
- JIDA EndodonticsArticleDocument11 pagesJIDA EndodonticsArticleSilviu TipleaNo ratings yet
- Removal of Calcifications From Distal Canals of Mandibular Molars by A Non-Instrumentational Cleaning System: A micro-CT StudyDocument6 pagesRemoval of Calcifications From Distal Canals of Mandibular Molars by A Non-Instrumentational Cleaning System: A micro-CT StudypoojaNo ratings yet
- Tooth Morphology and Access Cavity PreparationDocument232 pagesTooth Morphology and Access Cavity Preparationusmanhameed8467% (3)
- 2013 ABGDsgDocument244 pages2013 ABGDsgteertheshNo ratings yet
- C-shaped Canal Management with Three Obturation SystemsDocument4 pagesC-shaped Canal Management with Three Obturation SystemsJot KhalsaNo ratings yet
- Access Cavity Preparations: Classi Fication and Literature Review of Traditional and Minimally Invasive Endodontic Access Cavity DesignsDocument16 pagesAccess Cavity Preparations: Classi Fication and Literature Review of Traditional and Minimally Invasive Endodontic Access Cavity DesignsAlexandra Illescas GómezNo ratings yet
- Endodontic MishapsDocument19 pagesEndodontic MishapsSayak GuptaNo ratings yet
- Restoration of Endodontically Treated TeethDocument17 pagesRestoration of Endodontically Treated TeethAfaf MagedNo ratings yet
- Class II malocclusion: The aftermath of a “perfect stormDocument15 pagesClass II malocclusion: The aftermath of a “perfect stormThuyNo ratings yet
- Fixed Functional ApplianceDocument71 pagesFixed Functional AppliancekpNo ratings yet
- Palatal and Facial Veneers To TreatDocument11 pagesPalatal and Facial Veneers To TreatSabrina Antonella Zeballos ClarosNo ratings yet
- Ceramic Laminate Veneers: Clinical Procedures With A Multidisciplinary ApproachDocument24 pagesCeramic Laminate Veneers: Clinical Procedures With A Multidisciplinary ApproachDaniel AtiehNo ratings yet
- The Clincal Management of Ectopically Erupting First Permanent MolarsDocument6 pagesThe Clincal Management of Ectopically Erupting First Permanent MolarsFourthMolar.comNo ratings yet
- Developing Occlusion in Primary and Mixed DentitionDocument45 pagesDeveloping Occlusion in Primary and Mixed Dentitionpriti adsulNo ratings yet
- Brochure Veraviewepocs 3D R100 2019 ENDocument16 pagesBrochure Veraviewepocs 3D R100 2019 ENJosé Daniel Campos MéndezNo ratings yet
- 120 0215 Damon QuickReferenceGuideDocument12 pages120 0215 Damon QuickReferenceGuideAna Kuper0% (1)
- Class Ii Amalgam Cavity Preparation For AmalgamDocument82 pagesClass Ii Amalgam Cavity Preparation For AmalgamVidya Sagar100% (1)
- A Case of Nasopalatine Dust Cyst: Presentation, Diagnosis and ManagementDocument4 pagesA Case of Nasopalatine Dust Cyst: Presentation, Diagnosis and ManagementKertamayaNo ratings yet
- Dietschi 2020 Interceptive Treatment of Tooth Wear - Revised Protocol For The Full Molding TrechniqueDocument24 pagesDietschi 2020 Interceptive Treatment of Tooth Wear - Revised Protocol For The Full Molding TrechniqueCherifNo ratings yet
- Davidovitch1995 PDFDocument6 pagesDavidovitch1995 PDFRahulLife'sNo ratings yet
- Orthodontic Chart: Patient Information RecordDocument8 pagesOrthodontic Chart: Patient Information Recordpunyetanghangsarap Food Delivery ServiceNo ratings yet
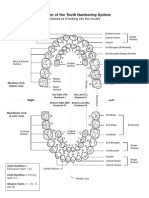
- Diagram of The Tooth Numbering SystemDocument1 pageDiagram of The Tooth Numbering Systemsaleh900No ratings yet
- ANTERIOR TEETH AND SMILE DESIGNDocument40 pagesANTERIOR TEETH AND SMILE DESIGNSahana RangarajanNo ratings yet
- Finite Element Analysis of Porcelain Veneers for Diastema ClosureDocument5 pagesFinite Element Analysis of Porcelain Veneers for Diastema ClosureMirnaLizNo ratings yet
- Brian Willison-2022 Lab Course ProjectsDocument3 pagesBrian Willison-2022 Lab Course ProjectsFabio RibeiroNo ratings yet
- Anterior Teeth Ndbe McqsDocument5 pagesAnterior Teeth Ndbe McqsParneetNo ratings yet
- B. The Overbite Achieved During TreatmentDocument60 pagesB. The Overbite Achieved During TreatmentRC Dome100% (3)
- Occlusal Equilibration: Presented By: Dr. Kelly NortonDocument36 pagesOcclusal Equilibration: Presented By: Dr. Kelly NortonLesley StephenNo ratings yet
- S4 BlankDocument117 pagesS4 BlankEun SaekNo ratings yet
- Esthetic Treatment of Altered Passve EruptionDocument19 pagesEsthetic Treatment of Altered Passve EruptiontaniaNo ratings yet
- Tooth Structure Removal Associated With Various Preparation Designs For Anterior TeethDocument7 pagesTooth Structure Removal Associated With Various Preparation Designs For Anterior TeethAlina AnechiteiNo ratings yet
- EndoPerio 003Document8 pagesEndoPerio 003kapawenkNo ratings yet
- Int Endodontic J - 2016 - Ahmed - A New System For Classifying Root and Root Canal MorphologyDocument10 pagesInt Endodontic J - 2016 - Ahmed - A New System For Classifying Root and Root Canal MorphologyRodrigo Cassana RojasNo ratings yet
- Lip Posture and Its Signi Ficance Treatment Plannin G: Indiamapoli., IndDocument20 pagesLip Posture and Its Signi Ficance Treatment Plannin G: Indiamapoli., IndYeraldin EspañaNo ratings yet
- Flat Plane OcclusionDocument22 pagesFlat Plane OcclusionDavid TaylorNo ratings yet
- 1 ManualDocument10 pages1 Manualwendyjemmy8gmailcomNo ratings yet
- Evolution of Orthodontic BracketsDocument281 pagesEvolution of Orthodontic Bracketssajida khan100% (2)
- The Relevance of Root Canal Isthmuses in Endodontic RehabilitationDocument13 pagesThe Relevance of Root Canal Isthmuses in Endodontic RehabilitationVictorNo ratings yet