You might also like
- Jurnal EbmDocument10 pagesJurnal EbmdeasyNo ratings yet
- Functional Rhinoplasty: David W. Kim,, Krista Rodriguez-BrunoDocument17 pagesFunctional Rhinoplasty: David W. Kim,, Krista Rodriguez-BrunoTarek abo kammerNo ratings yet
- Alveolar Recruitment Maneuvers Under General AnesthesiaDocument12 pagesAlveolar Recruitment Maneuvers Under General AnesthesiaBetzaBarriosNo ratings yet
- Nasal Airflow Assessment in Deviated Septum PatientsDocument2 pagesNasal Airflow Assessment in Deviated Septum PatientsRia Tutkey-MelmambessyNo ratings yet
- Altered Speech Following Adenoidectomy A 20 Year ExperienceDocument5 pagesAltered Speech Following Adenoidectomy A 20 Year Experienceenfanat23No ratings yet
- Pathophysiology of Empty Nose Syndrome: Contemporary ReviewDocument5 pagesPathophysiology of Empty Nose Syndrome: Contemporary ReviewTheodore LiwonganNo ratings yet
- Clinical Consensus Statement Diagnosis and Management of Nasal ValveDocument12 pagesClinical Consensus Statement Diagnosis and Management of Nasal ValveThomasMáximoMancinelliRinaldoNo ratings yet
- American Journal of Otolaryngology-Head and Neck Medicine and SurgeryDocument7 pagesAmerican Journal of Otolaryngology-Head and Neck Medicine and Surgeryabhishekjha0082No ratings yet
- Effects of Surgical Treatment PDFDocument6 pagesEffects of Surgical Treatment PDFAssifa RidzkiNo ratings yet
- Endoscopic Sinus Surgery: Indications and Complications: February 2020Document7 pagesEndoscopic Sinus Surgery: Indications and Complications: February 2020husnul khatimahNo ratings yet
- Thirty Years of Submental Intubation: A Review: Review Paper Oral SurgeryDocument5 pagesThirty Years of Submental Intubation: A Review: Review Paper Oral SurgeryUmer HussainNo ratings yet
- Efficacy of Sinusitis UltrasoundDocument7 pagesEfficacy of Sinusitis UltrasoundYazid MultazamNo ratings yet
- AntibodyDocument5 pagesAntibodyRokhmat Bintang DjaisNo ratings yet
- Estenosis Traqueal ComplejaDocument8 pagesEstenosis Traqueal ComplejaFabiolaNo ratings yet
- Medip,+15 59 1 CEDocument7 pagesMedip,+15 59 1 CEKabir Ahmed LaskarNo ratings yet
- Indian Journal of Otolaryngology and Head & Neck SurgeryDocument14 pagesIndian Journal of Otolaryngology and Head & Neck SurgeryDrKunal KaradeNo ratings yet
- The Nasal Cycle A Comprehensive ReviewDocument11 pagesThe Nasal Cycle A Comprehensive ReviewJabin HuangNo ratings yet
- Laringo y BroncoespasmoDocument4 pagesLaringo y BroncoespasmoLUIS FERNANDO GOMEZ CANONo ratings yet
- Validity of PNIF as Screening Tool for Nasal ObstructionDocument6 pagesValidity of PNIF as Screening Tool for Nasal ObstructionDenise MathreNo ratings yet
- PARS Reader's Digest - Apr 2013Document12 pagesPARS Reader's Digest - Apr 2013info8673No ratings yet
- Impact of Corrective Rhinologic Surgery On Rhinogenic HeadacheDocument4 pagesImpact of Corrective Rhinologic Surgery On Rhinogenic HeadacheSinan Kadir AltunalNo ratings yet
- Journal Atrophic RhinitsDocument0 pagesJournal Atrophic RhinitsDion Satriawan DhaniardiNo ratings yet
- 2008 Chest - The Blue ProtocolDocument9 pages2008 Chest - The Blue Protocoleduardo0% (1)
- A Comparative Study of Endoscopic Versus Conventional Septoplasty An Analysis of 50 CasesDocument6 pagesA Comparative Study of Endoscopic Versus Conventional Septoplasty An Analysis of 50 CasesDay LightNo ratings yet
- Diagnosis of Pleural Effusion A Systematic ApproachDocument11 pagesDiagnosis of Pleural Effusion A Systematic Approachvictor ibarra romeroNo ratings yet
- (9, 13, 27, 42) Complications in EndoscopicDocument18 pages(9, 13, 27, 42) Complications in EndoscopicChiNdy AfiSaNo ratings yet
- Chronic Rhinosinusitis Overview - Less than 40 CharactersDocument6 pagesChronic Rhinosinusitis Overview - Less than 40 CharactersMilanisti22No ratings yet
- EnsDocument6 pagesEnsAlwi Qatsir AlyaNo ratings yet
- Radiological Findings in Patients Undergoing Revision Endoscopic Sinus Surgery: A Retrospective Case Series StudyDocument6 pagesRadiological Findings in Patients Undergoing Revision Endoscopic Sinus Surgery: A Retrospective Case Series StudyFelicia MelaniNo ratings yet
- Inferior Turbinectomy For Nasal Obstruction Review of 75 CasesDocument4 pagesInferior Turbinectomy For Nasal Obstruction Review of 75 CasesMeilina Elin WardhaniNo ratings yet
- Acceptedpaper - A Rare Case Choanal Stenosis Bilateral in Nasopharyngeal Carcinoma Patient With Endoscopic Surgery Management - DR - Yulialdi Bimanto Heryanto Putra - Yulialdi Bimanto Heryanto PutraDocument7 pagesAcceptedpaper - A Rare Case Choanal Stenosis Bilateral in Nasopharyngeal Carcinoma Patient With Endoscopic Surgery Management - DR - Yulialdi Bimanto Heryanto Putra - Yulialdi Bimanto Heryanto PutraRika Sartyca IlhamNo ratings yet
- Literatür 3Document4 pagesLiteratür 3Sinan Kadir AltunalNo ratings yet
- Lary 24206Document2 pagesLary 24206dr_ismiNo ratings yet
- Role of Swallowing Function of Tracheotomised Patients in Major Head and Neck Cancer SurgeryDocument3 pagesRole of Swallowing Function of Tracheotomised Patients in Major Head and Neck Cancer SurgeryAnonymous xvlg4m5xLXNo ratings yet
- Eccles Nasal Air Flow in Health and DiseaseDocument16 pagesEccles Nasal Air Flow in Health and DiseasemanalNo ratings yet
- Arya PDFDocument26 pagesArya PDFRahmawati JuliaNo ratings yet
- Management of Nasolabial Cysts by Transnasal Endoscopic MarsupializationDocument8 pagesManagement of Nasolabial Cysts by Transnasal Endoscopic Marsupializationfk06No ratings yet
- PARS Reader's Digest - Feb 2013Document12 pagesPARS Reader's Digest - Feb 2013info8673No ratings yet
- Journal of Otolaryngology and Rhinology Jor 2 016Document5 pagesJournal of Otolaryngology and Rhinology Jor 2 016naveed gulNo ratings yet
- 1 s2.0 S0196070922003945 MainDocument8 pages1 s2.0 S0196070922003945 MainJose Miguel CastellonNo ratings yet
- Distal Lakrimal Kanal T Kan KL Na e Lik Eden Lateral Nazal Duvar Patolojilerinin Incelenmesi (#180604) - 160005Document4 pagesDistal Lakrimal Kanal T Kan KL Na e Lik Eden Lateral Nazal Duvar Patolojilerinin Incelenmesi (#180604) - 160005Gusti Zidni FahmiNo ratings yet
- Functional RhinoplastyDocument11 pagesFunctional Rhinoplastycafa10No ratings yet
- Nasal Tip Numbness After RhinoplastyDocument4 pagesNasal Tip Numbness After RhinoplastySinan Kadir AltunalNo ratings yet
- American Journal of Otolaryngology - Head and Neck Medicine and SurgeryDocument4 pagesAmerican Journal of Otolaryngology - Head and Neck Medicine and SurgerySyalara FatharaniNo ratings yet
- Eustachian TubeDocument6 pagesEustachian TubeMusyfiqoh TusholehahNo ratings yet
- Sawh Martinez2019 PDFDocument9 pagesSawh Martinez2019 PDFDanielBallesterosNo ratings yet
- Jurnal LaringitisDocument12 pagesJurnal LaringitismeishellaNo ratings yet
- Semler Et Al 2016Document8 pagesSemler Et Al 2016Neneng VitriyahNo ratings yet
- 234 FarmerDocument6 pages234 FarmerRaghavendra NalatawadNo ratings yet
- aijoc-2013-05-043Document3 pagesaijoc-2013-05-043Hussein AhmedNo ratings yet
- Primary Versus Secondary Tracheoesophageal Puncture: Systematic Review and Meta-AnalysisDocument8 pagesPrimary Versus Secondary Tracheoesophageal Puncture: Systematic Review and Meta-AnalysisIsrael BlancoNo ratings yet
- Reconstruction of The Nasal ColumellaDocument5 pagesReconstruction of The Nasal ColumellaIndah GitaswariNo ratings yet
- MainDocument6 pagesMainDhio ArieyonaNo ratings yet
- Evaluation of Prognostic Factors and Middle Ear RiskDocument5 pagesEvaluation of Prognostic Factors and Middle Ear RiskKye Hoon ParkNo ratings yet
- 2 DiaphragmaticExcursionDocument4 pages2 DiaphragmaticExcursionAnandhu GNo ratings yet
- THT Zalfina CoraDocument7 pagesTHT Zalfina CoraFatiaNo ratings yet
- 216851-Article Text-533920-1-10-20211102Document5 pages216851-Article Text-533920-1-10-20211102Vaino MungobaNo ratings yet
- Airway Management For The Oral Surgery Patient 2018Document20 pagesAirway Management For The Oral Surgery Patient 2018Aldo AguilarNo ratings yet
- Septum Endoscopico o TraeicionaDocument6 pagesSeptum Endoscopico o TraeicionavsberraondoNo ratings yet
- The Cambridge Handbook of Clinical Assessment and Diagnosis (2019)Document534 pagesThe Cambridge Handbook of Clinical Assessment and Diagnosis (2019)Ofelia Kerr100% (4)
- Alexthymia in Sexual Disorder Clinic PatientsDocument7 pagesAlexthymia in Sexual Disorder Clinic PatientsFélix Aníbal Acuña OlivosNo ratings yet
- Prolonged Fasting - How Is It PosiblerDocument17 pagesProlonged Fasting - How Is It PosiblersaturninojonesNo ratings yet
- f3 Home-Sci Simplified Notes SPDocument20 pagesf3 Home-Sci Simplified Notes SPmicah isabokeNo ratings yet
- Ps DM - Ogl 365-Module 6 PaperDocument3 pagesPs DM - Ogl 365-Module 6 Paperapi-573130450No ratings yet
- Shell Rimula R2 40 (CF) : Performance, Features & BenefitsDocument2 pagesShell Rimula R2 40 (CF) : Performance, Features & BenefitsMuhammad SaputraNo ratings yet
- Continuous Monitoring of Erns: Set of Ern Core IndicatorsDocument23 pagesContinuous Monitoring of Erns: Set of Ern Core IndicatorsElenaNo ratings yet
- Jurnal MastoiditisDocument12 pagesJurnal Mastoiditisahtiyal murdinNo ratings yet
- mgmt404 Final Project HMPDocument22 pagesmgmt404 Final Project HMPapi-25526962850% (2)
- COVID vaccination certificate for Indian teenDocument1 pageCOVID vaccination certificate for Indian teenShubham TiwariNo ratings yet
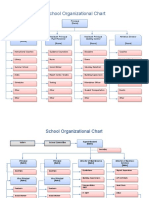
- School Organizational ChartDocument4 pagesSchool Organizational ChartislahNo ratings yet
- Tagaytay Es - Annex ADocument4 pagesTagaytay Es - Annex AEduardoAlejoZamoraJr.No ratings yet
- Implementing Trauma-Informed Care in Primary Hamberger-2019-Medical Settings-Evidence-Based Rationale and Approaches PDFDocument22 pagesImplementing Trauma-Informed Care in Primary Hamberger-2019-Medical Settings-Evidence-Based Rationale and Approaches PDFMonica DyerNo ratings yet
- Incident Investigation and Reporting ProcedureDocument6 pagesIncident Investigation and Reporting ProcedureSérgio CoutoNo ratings yet
- How To Make Easy French ToastDocument4 pagesHow To Make Easy French Toastbintang pamungkasNo ratings yet
- Neurotoxicity of Local Anesthetics in DentistryDocument7 pagesNeurotoxicity of Local Anesthetics in DentistryVinicíus PavaniNo ratings yet
- The Female Reproductive System: Dr. Emanuel Muro HkmuDocument41 pagesThe Female Reproductive System: Dr. Emanuel Muro HkmuMustafa DadahNo ratings yet
- Intelligent ConstructionDocument4 pagesIntelligent ConstructionRikesh SapkotaNo ratings yet
- Dysmenorrhea Social Support Anxiety Pain LevelsDocument8 pagesDysmenorrhea Social Support Anxiety Pain LevelsEgawidya EgaNo ratings yet
- Ndian Nstitute of Ourism & Ravel Anagement: I T T MDocument69 pagesNdian Nstitute of Ourism & Ravel Anagement: I T T Msilly_chilly100% (4)
- Dawit Tadesse Fortification AssignmentDocument13 pagesDawit Tadesse Fortification AssignmentDeavoNo ratings yet
- Blue Royale PlanDocument8 pagesBlue Royale PlanMikele Molina BetervoNo ratings yet
- Orthop J Sports Med 2021 9 7 23259671211013394Document6 pagesOrthop J Sports Med 2021 9 7 23259671211013394Fernando SousaNo ratings yet
- Underground Interrogation With Steve CotterDocument12 pagesUnderground Interrogation With Steve CotterTom HillNo ratings yet
- Cramming Is BadDocument3 pagesCramming Is Badlady joNo ratings yet
- Introduction: A New Hierarchy of NeedsDocument5 pagesIntroduction: A New Hierarchy of Needsgun2 block100% (1)
- LAP Form v2Document2 pagesLAP Form v2realwavesbhNo ratings yet
- Nur3116 Social Determinants of Health PaperDocument6 pagesNur3116 Social Determinants of Health Paperapi-578141969No ratings yet
- The Kübler-Ross Change Curve: Emotional Response To ChangeDocument9 pagesThe Kübler-Ross Change Curve: Emotional Response To ChangeChanel PostelNo ratings yet
- PRA Tool Box: 6.1. Brief Introduction To PRADocument16 pagesPRA Tool Box: 6.1. Brief Introduction To PRAfaisalNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (19)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Secure Love: Create a Relationship That Lasts a LifetimeFrom EverandSecure Love: Create a Relationship That Lasts a LifetimeRating: 5 out of 5 stars5/5 (18)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)