You might also like
- Triple Bottom Line Risk Management: Enhancing Profit, Environmental Performance, and Community BenefitsFrom EverandTriple Bottom Line Risk Management: Enhancing Profit, Environmental Performance, and Community BenefitsNo ratings yet
- Critical Risks of Different Economic Sectors: Based on the Analysis of More Than 500 Incidents, Accidents and DisastersFrom EverandCritical Risks of Different Economic Sectors: Based on the Analysis of More Than 500 Incidents, Accidents and DisastersNo ratings yet
- Checklist WeldingDocument5 pagesChecklist WeldingMarko RisticNo ratings yet
- Risk Assessment Tennis CourtDocument2 pagesRisk Assessment Tennis CourtLouis BimpsonNo ratings yet
- Risk Assessment FinalDocument2 pagesRisk Assessment FinalAaron HigginsNo ratings yet
- Risk Assessment Recording FormDocument3 pagesRisk Assessment Recording Formhenry wrightNo ratings yet
- Risk Assesment Fab - Rev-07Document71 pagesRisk Assesment Fab - Rev-07Nikhil PuthiryNo ratings yet
- Risk Assesment Photoshoot2Document3 pagesRisk Assesment Photoshoot2wd05025311No ratings yet
- Grace Ra GardenDocument3 pagesGrace Ra GardenGrace TooneNo ratings yet
- SF 011 Hazard Risk AseessmentDocument3 pagesSF 011 Hazard Risk AseessmentShahid RazaNo ratings yet
- Risk Assessment Format For SampleDocument3 pagesRisk Assessment Format For SampleSaqib RasoolNo ratings yet
- Module 4 HiracDocument22 pagesModule 4 HiracGerald Hernandez100% (1)
- Excavation Risk AssessmentDocument3 pagesExcavation Risk AssessmentWilson Wambua0% (1)
- Lab1 Risk AssessmentsDocument14 pagesLab1 Risk AssessmentsalwkilmunirhNo ratings yet
- Risk Assessment Recording FormDocument2 pagesRisk Assessment Recording Formhenry wrightNo ratings yet
- General Risk AssessmentDocument3 pagesGeneral Risk Assessmentdeja_149547234No ratings yet
- Example Industry Hazard Register 2022Document5 pagesExample Industry Hazard Register 2022She-Ra Sha-Ju LaNo ratings yet
- Risk Assessment Tennis CourtDocument2 pagesRisk Assessment Tennis CourtOliver HorsfieldNo ratings yet
- Appendix A Risk Assessment & Mode of ContractDocument5 pagesAppendix A Risk Assessment & Mode of ContractSherif MahmoudNo ratings yet
- Risk Assessment FinalDocument2 pagesRisk Assessment FinalAaron HigginsNo ratings yet
- Risk Assessment Template CollgeDocument2 pagesRisk Assessment Template CollgeMolly WatkissNo ratings yet
- Risk Assessment Template-Ps4Document3 pagesRisk Assessment Template-Ps4Michael MckayNo ratings yet
- 31.0.11 ALR - Temporary Electrical InstallationDocument3 pages31.0.11 ALR - Temporary Electrical InstallationGerritNo ratings yet
- Travel Risk Assessment Checklist - Security & SafetyDocument13 pagesTravel Risk Assessment Checklist - Security & SafetyHarisNo ratings yet
- Rail Generic Risk Assessments V8 2014Document10 pagesRail Generic Risk Assessments V8 2014SbitNo ratings yet
- Risk Assessment Victoria ParkDocument3 pagesRisk Assessment Victoria ParkBrendan EarleyNo ratings yet
- Risk Assessment For ChapelfordDocument2 pagesRisk Assessment For ChapelfordKyle DavidsonNo ratings yet
- RA Existing Asphalt Milling WorksDocument8 pagesRA Existing Asphalt Milling WorksSolimanNo ratings yet
- Hira - IbsplDocument7 pagesHira - IbsplAbdul Raheem100% (1)
- Risk Assessment Template GymDocument2 pagesRisk Assessment Template GymLouis BimpsonNo ratings yet
- Hazard Identification and Risk Assessment for Loading and Off-Loading with Truck Mounted CraneDocument5 pagesHazard Identification and Risk Assessment for Loading and Off-Loading with Truck Mounted CraneGerrit100% (1)
- Risk Assessment PA.20Document3 pagesRisk Assessment PA.20Luke CorbishleyNo ratings yet
- Risk Assessment PA 20Document3 pagesRisk Assessment PA 20Trinity CharnockNo ratings yet
- Safety at OffshoreDocument51 pagesSafety at OffshoreRavi Kant TripathiNo ratings yet
- RMH HiraDocument12 pagesRMH HiraShirley SetshediNo ratings yet
- Risk Asses Ment Fasion Spread 4Document3 pagesRisk Asses Ment Fasion Spread 4Anonymous IXOiMTtHrNo ratings yet
- Risk Assessment PhotoshootDocument2 pagesRisk Assessment PhotoshootlucyNo ratings yet
- EMP-TR347-HFC-MES-020 Tie in ConnectionDocument13 pagesEMP-TR347-HFC-MES-020 Tie in ConnectionsajinNo ratings yet
- Risk Assessment CausewayDocument3 pagesRisk Assessment CausewayPriestley T.A.T.ENo ratings yet
- EICR Risk AssessmentDocument14 pagesEICR Risk Assessmentprince olanNo ratings yet
- Risk Assessment GardenDocument2 pagesRisk Assessment GardenMatthew BaguleyNo ratings yet
- Assessment Task: AWE: Individual Risk Analysis: Step 1: Step 2: Step 3: Step 4: Step 5Document9 pagesAssessment Task: AWE: Individual Risk Analysis: Step 1: Step 2: Step 3: Step 4: Step 5gopiNo ratings yet
- Frontliners HirarcDocument8 pagesFrontliners HirarcSitiAliahNo ratings yet
- Dismantling and Lifting Risks of Existing EDG and Installation of New EDGDocument10 pagesDismantling and Lifting Risks of Existing EDG and Installation of New EDGSubbu AbuNo ratings yet
- Risk Asses Ment Fasion Spread 3Document3 pagesRisk Asses Ment Fasion Spread 3Anonymous IXOiMTtHrNo ratings yet
- Risk Assessment Template 4Document2 pagesRisk Assessment Template 4kyle donnellyNo ratings yet
- Car - Risk AssessmentDocument3 pagesCar - Risk AssessmentLouis BimpsonNo ratings yet
- Risk Assessment Recording FormDocument2 pagesRisk Assessment Recording Formkyle donnellyNo ratings yet
- Site Risk RADocument14 pagesSite Risk RAJohn GeddesNo ratings yet
- Road ReinstatementDocument4 pagesRoad ReinstatementBishop Ojonuguwa AmehNo ratings yet
- Risk Assessment - KitchenDocument3 pagesRisk Assessment - KitchenOlivia BrookesNo ratings yet
- Risk Assessment HouseDocument2 pagesRisk Assessment HouseJai StandingNo ratings yet
- FIMA RISK ASSESSMENT ANALYSISDocument17 pagesFIMA RISK ASSESSMENT ANALYSISNur Alisha AlishaNo ratings yet
- Risk Assessment TrailDocument3 pagesRisk Assessment TrailYasmin DeanNo ratings yet
- METEC DESIGN & CONSTRUCTION RISK ASSESSMENTDocument235 pagesMETEC DESIGN & CONSTRUCTION RISK ASSESSMENTSamy KsNo ratings yet
- Hazard Identification and Risk Assessment FormDocument4 pagesHazard Identification and Risk Assessment FormAli Al-GhamghamNo ratings yet
- Risk Assessment Template - HouseDocument3 pagesRisk Assessment Template - HouseSean SpencerNo ratings yet
- Risk Assessment RiverDocument3 pagesRisk Assessment RiverLuke CorbishleyNo ratings yet
- Risk Asses Ment Fasion Spread 1Document3 pagesRisk Asses Ment Fasion Spread 1Anonymous IXOiMTtHrNo ratings yet
- Adventurer's Guide to Risk Management: Fictional Tales about Risk ManagementFrom EverandAdventurer's Guide to Risk Management: Fictional Tales about Risk ManagementNo ratings yet
- S2 Papers FinalizedDocument149 pagesS2 Papers FinalizedRaffles HolmesNo ratings yet
- Hearing Aid InformationDocument22 pagesHearing Aid InformationDeepakRodeyNo ratings yet
- XR5 9 Element 5 Band Yagi 20-17-15-12-10MDocument16 pagesXR5 9 Element 5 Band Yagi 20-17-15-12-10Msboonuy331No ratings yet
- B Ed 3 Sem Physics Teaching Group C Science 1 Paper 1 Summer 2018Document3 pagesB Ed 3 Sem Physics Teaching Group C Science 1 Paper 1 Summer 2018Rrr KkkNo ratings yet
- RCS England Trainees Guide To A Quality Improvement Project 2021Document17 pagesRCS England Trainees Guide To A Quality Improvement Project 2021Wee K WeiNo ratings yet
- 11 Physics Test Paper Ch3 1Document4 pages11 Physics Test Paper Ch3 1Devendar SharmaNo ratings yet
- Ceph Reference ArchitectureDocument12 pagesCeph Reference ArchitectureGermgmaan100% (1)
- Erasmus Rotterdam University MCDocument24 pagesErasmus Rotterdam University MCAndreea CroitoruNo ratings yet
- A Robust Firearm Identification Algorithm ProposalDocument7 pagesA Robust Firearm Identification Algorithm ProposalEuneel EscalaNo ratings yet
- List of Students Allotted in Open Elective Subjects (B. Tech and M. Tech (Dual Degree) Integrated MSc. - 4th Semester - Regular - 2018 - 19) - 2 PDFDocument26 pagesList of Students Allotted in Open Elective Subjects (B. Tech and M. Tech (Dual Degree) Integrated MSc. - 4th Semester - Regular - 2018 - 19) - 2 PDFArpan JaiswalNo ratings yet
- The Image of The CityDocument17 pagesThe Image of The CityMay Rose ParagasNo ratings yet
- Textiles and Clothing SustaninabilityDocument134 pagesTextiles and Clothing Sustaninabilitydike100% (1)
- SFM Issue Repor 15-4-2023Document3 pagesSFM Issue Repor 15-4-2023Esdras Fransua CisnerosNo ratings yet
- Chapter 14 Chemical EquilibriumDocument29 pagesChapter 14 Chemical EquilibriumlynloeNo ratings yet
- IP Modulator User's Guide - Oct - 09Document68 pagesIP Modulator User's Guide - Oct - 09reivajjwNo ratings yet
- FLIR Blackfly Users ManualDocument53 pagesFLIR Blackfly Users ManualPavan Kumar BittuNo ratings yet
- Effect of Pregnancy Induced Hypertension on Mothers and Babies Hematological ProfilesDocument3 pagesEffect of Pregnancy Induced Hypertension on Mothers and Babies Hematological ProfilesAbdifatah AhmedNo ratings yet
- Catalogus 2010 ENGELSDocument52 pagesCatalogus 2010 ENGELShacikadiNo ratings yet
- Philips HF C-Arm BrochureDocument2 pagesPhilips HF C-Arm Brochuregarysov50% (2)
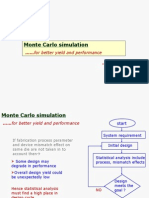
- Cadence Monte Carlo Simulation TutorialDocument51 pagesCadence Monte Carlo Simulation Tutorialkuomatt100% (1)
- CD 0400 CH 4 X 100 ML: For in Vitro Diagnostic Use Only. LinearityDocument1 pageCD 0400 CH 4 X 100 ML: For in Vitro Diagnostic Use Only. LinearityNguyễn ThơiNo ratings yet
- Mobile Network Optimization MapDocument1 pageMobile Network Optimization MapShahzad Farooq100% (1)
- SPC英文版教材Document83 pagesSPC英文版教材bing cai100% (2)
- Shock Classification and PathophysiologyDocument40 pagesShock Classification and PathophysiologyErick Anca100% (2)
- IAL Edexcel Pure Math 1 January 2020Document28 pagesIAL Edexcel Pure Math 1 January 2020Mohamed Said Daw100% (4)
- BAlochistanDocument14 pagesBAlochistanzee100% (1)
- The Respiratory System - Freebie GuideDocument4 pagesThe Respiratory System - Freebie GuideIndustria Quimica0% (1)
- The Storage Handling and Transportation of Ammonium Nitrate Based Fertilisers 2015Document58 pagesThe Storage Handling and Transportation of Ammonium Nitrate Based Fertilisers 2015Minh Đức TạNo ratings yet
- Experiment# 3 Projectile Motion (Tasks 3 and 4)Document18 pagesExperiment# 3 Projectile Motion (Tasks 3 and 4)Hafiz MuhammadNo ratings yet
- Kyle 106 - 119 - 131 - 141Document1 pageKyle 106 - 119 - 131 - 141Gerson SouzaNo ratings yet