You might also like
- Nov 151Document6 pagesNov 151alexandre06frNo ratings yet
- Abedalthagaf 2018Document8 pagesAbedalthagaf 2018NicoNo ratings yet
- 1267 FTP PDFDocument8 pages1267 FTP PDFFathulRachmanNo ratings yet
- ImmunoDocument2 pagesImmunodiceNo ratings yet
- Biologia Futura Emerging Antigen-Specific Therapies For Autoimmune DiseasesDocument10 pagesBiologia Futura Emerging Antigen-Specific Therapies For Autoimmune DiseasesAleksandar MilanovicNo ratings yet
- 2020 - Tun - HL ImmunotherapyDocument10 pages2020 - Tun - HL ImmunotherapyMiguel ÁngelNo ratings yet
- Nri 1936 ArtigoDocument13 pagesNri 1936 ArtigoGlauce L TrevisanNo ratings yet
- DDS For Cancer ImmunotherapyDocument55 pagesDDS For Cancer ImmunotherapyLe Ngoc DuyNo ratings yet
- STING Agonist-Loaded, CD47/PD-L1-targeting Nanoparticles Potentiate Antitumor Immu-Nity and Radiotherapy For GlioblastomaDocument19 pagesSTING Agonist-Loaded, CD47/PD-L1-targeting Nanoparticles Potentiate Antitumor Immu-Nity and Radiotherapy For GlioblastomaAnonymous HUY0yRexYfNo ratings yet
- Immunopotent Part 1Document31 pagesImmunopotent Part 1samyNo ratings yet
- Klinman 2004Document16 pagesKlinman 2004ziNo ratings yet
- Combination Checkpoint Therapy With Anti PD 1 and Anti BTLA Results in A Synergistic Therapeutic Effect Against Murine GlioblastomaDocument10 pagesCombination Checkpoint Therapy With Anti PD 1 and Anti BTLA Results in A Synergistic Therapeutic Effect Against Murine GlioblastomaCher IshNo ratings yet
- Neurochemistry International: SciencedirectDocument12 pagesNeurochemistry International: SciencedirectPaige MunroeNo ratings yet
- Mechanism of Action and Resistance To Monoclonal Antibody TherapyDocument10 pagesMechanism of Action and Resistance To Monoclonal Antibody TherapyYing ChenNo ratings yet
- Novel Immunomodulatory Drugs and Neo-SubstratesDocument8 pagesNovel Immunomodulatory Drugs and Neo-Substratesgundeepdsc8423No ratings yet
- Targeted Therapy in Oncology: Update ArticleDocument5 pagesTargeted Therapy in Oncology: Update ArticleRajeev GuptaNo ratings yet
- 4. Phân phối thuốc trị ung thư bằng hạt nanoDocument11 pages4. Phân phối thuốc trị ung thư bằng hạt nanoPhương AnhNo ratings yet
- γδ T Cells as Immuno-Oncology Treatments in the Era of Precision MedicineHarnessing the potential of the immune system to treat cancers has been the goal of many scientific investigations in the last few decades. Recent advances in cancer biology and immunology have allowed for cancer immunotherapy to become a reality. The premise of cancer immunotherapy is to stimulate the patient’s own immune system to attack and reject the malignant cells, sparing normal surrounding tissues.Document6 pagesγδ T Cells as Immuno-Oncology Treatments in the Era of Precision MedicineHarnessing the potential of the immune system to treat cancers has been the goal of many scientific investigations in the last few decades. Recent advances in cancer biology and immunology have allowed for cancer immunotherapy to become a reality. The premise of cancer immunotherapy is to stimulate the patient’s own immune system to attack and reject the malignant cells, sparing normal surrounding tissues.Bruce LennyNo ratings yet
- 7 Cancer Immunotherapy Etc-2020Document32 pages7 Cancer Immunotherapy Etc-2020Syifa KhairunnisaNo ratings yet
- Jurnal BioselDocument15 pagesJurnal BioselRegita cahyani priscalisyiNo ratings yet
- Gene Therapy Where We Are: and Where To Go?Document60 pagesGene Therapy Where We Are: and Where To Go?Faisal GhairatNo ratings yet
- Avelumab 45Document10 pagesAvelumab 45bawoji1763No ratings yet
- Immunopharmacology: Dr. Hamad AlshabiDocument8 pagesImmunopharmacology: Dr. Hamad AlshabiHamad Alshabi100% (1)
- The Therapeutic Potential of Nanobodies: Ivana Jovčevska Serge MuyldermansDocument16 pagesThe Therapeutic Potential of Nanobodies: Ivana Jovčevska Serge MuyldermansJessica Asitimbay ZuritaNo ratings yet
- Terapia Con Anticuerpos Monoclonales en LLADocument6 pagesTerapia Con Anticuerpos Monoclonales en LLAMacarena Tapia MaldonadoNo ratings yet
- Immunotherapy in Translational Cancer ResearchFrom EverandImmunotherapy in Translational Cancer ResearchLaurence J. N. CooperNo ratings yet
- Ima y Dasa Reducen MDSCs y Aumentan Respuestas EfectorasDocument12 pagesIma y Dasa Reducen MDSCs y Aumentan Respuestas EfectorasLyanna StarkNo ratings yet
- Fonc 08 00086Document14 pagesFonc 08 00086Siska HarapanNo ratings yet
- IMP MDSCs Tregs y NKs BelloDocument11 pagesIMP MDSCs Tregs y NKs BelloLyanna StarkNo ratings yet
- Improving The Efficacy of Antibody-Based Cancer Therapies: ReviewsDocument12 pagesImproving The Efficacy of Antibody-Based Cancer Therapies: ReviewsktamvadaNo ratings yet
- Monoclonal Antibodies: Dr. Jeevan Jacob Junior Resident in Pharmacology Calicut Medical CollegeDocument63 pagesMonoclonal Antibodies: Dr. Jeevan Jacob Junior Resident in Pharmacology Calicut Medical CollegeEnosNo ratings yet
- Developing Costimulatory Molecules for Immunotherapy of DiseasesFrom EverandDeveloping Costimulatory Molecules for Immunotherapy of DiseasesNo ratings yet
- University of Sulaimaniah: College of Dentistry Presentation:-Asked by Presented ByDocument61 pagesUniversity of Sulaimaniah: College of Dentistry Presentation:-Asked by Presented ByNina MoradNo ratings yet
- Keith Lowden - What's The Deal With This New ChemotherapyDocument25 pagesKeith Lowden - What's The Deal With This New ChemotherapyTam Le Ngoc KhanhNo ratings yet
- Target Therapies in Pancreatic CancerDocument6 pagesTarget Therapies in Pancreatic CancerReneNo ratings yet
- Nej Mo A 2308917Document14 pagesNej Mo A 2308917mnf6bb2tckNo ratings yet
- Recent Developments in Immunotherapy of Acute Myeloid LeukemiaDocument20 pagesRecent Developments in Immunotherapy of Acute Myeloid LeukemiaAkbar ShiddiqNo ratings yet
- Monoclonal Antibodies: Anticancer Therapy Weihua WuDocument13 pagesMonoclonal Antibodies: Anticancer Therapy Weihua WuMuhammad Naeem IqbalNo ratings yet
- (Methods in Molecular Medicine) Caroline J. Springer - Suicide Gene Therapy, Methods and Reviews (2003, Humana Press)Document543 pages(Methods in Molecular Medicine) Caroline J. Springer - Suicide Gene Therapy, Methods and Reviews (2003, Humana Press)fapoki707No ratings yet
- Melero 2007Document12 pagesMelero 2007Django BoyeeNo ratings yet
- Bertoni 2020 CTRDocument11 pagesBertoni 2020 CTRAnselmo GonzalezNo ratings yet
- Antibodies Safety PDFDocument14 pagesAntibodies Safety PDFTai BuiNo ratings yet
- Kuryk Et Al PembrolizumabDocument12 pagesKuryk Et Al PembrolizumabLJ NissenNo ratings yet
- The Clinical Impact of The Molecular Landscape of Acute Myeloid LeukemiaDocument13 pagesThe Clinical Impact of The Molecular Landscape of Acute Myeloid LeukemiaCT DAMNo ratings yet
- Targeted Therapy in CancerDocument51 pagesTargeted Therapy in CancerSatya WangsaNo ratings yet
- Vaccines 10 01993Document18 pagesVaccines 10 01993soprisesNo ratings yet
- Full TextDocument9 pagesFull Textbodeadumitru9261No ratings yet
- CN 19 1246Document18 pagesCN 19 1246Alexandra MoraesNo ratings yet
- The Basics of Cancer ImmunotherapyFrom EverandThe Basics of Cancer ImmunotherapyHaidong DongNo ratings yet
- Biologics in OculoplastyDocument4 pagesBiologics in OculoplastyVishNo ratings yet
- 1 s2.0 S104453232100066X MainDocument17 pages1 s2.0 S104453232100066X MainAnita DewiNo ratings yet
- Paper 4 - Developement of A Bispecific Antibody Targeting PD-L1 and TIGIT With Optimal CytotocityDocument11 pagesPaper 4 - Developement of A Bispecific Antibody Targeting PD-L1 and TIGIT With Optimal CytotocityChauPhuongNo ratings yet
- World-Class Research Center Digital Biodesign and Personalized HealthcareDocument32 pagesWorld-Class Research Center Digital Biodesign and Personalized HealthcareMurad DzhavadovNo ratings yet
- Luthra2021 Article RoleOfDifferentPeptidesForCancDocument17 pagesLuthra2021 Article RoleOfDifferentPeptidesForCancAkdicmsNo ratings yet
- Development of in Vitro Assays For Advancing Radioimmunotherapy Against Brain TumorsDocument25 pagesDevelopment of in Vitro Assays For Advancing Radioimmunotherapy Against Brain TumorsDr Andrew EkpenyongNo ratings yet
- Recent Progresses in Phototherapy-Synergized Cancer ImmunotherapyDocument46 pagesRecent Progresses in Phototherapy-Synergized Cancer Immunotherapygan publishingNo ratings yet
- Immune Checkpointtargeted Therapy Cancer and Autoimmune Diseases Represent Two Sides of The Same CoinDocument4 pagesImmune Checkpointtargeted Therapy Cancer and Autoimmune Diseases Represent Two Sides of The Same Coinpratiwi eka rahmawatiNo ratings yet
- Gpc3 Generate de Celule Dendritice 2010Document11 pagesGpc3 Generate de Celule Dendritice 2010grigmihNo ratings yet
- SARS-CoV-2 and Covid19 Lecture 3 - 2Document5 pagesSARS-CoV-2 and Covid19 Lecture 3 - 2Aishwarya SinghNo ratings yet
- Big Data in HealthcareDocument14 pagesBig Data in HealthcareAishwarya SinghNo ratings yet
- Anomaly Detection 2Document8 pagesAnomaly Detection 2Aishwarya SinghNo ratings yet
- Intro DBM 2Document3 pagesIntro DBM 2Aishwarya SinghNo ratings yet
- Lecture 3 Immunology of CancerDocument4 pagesLecture 3 Immunology of CancerAishwarya SinghNo ratings yet
- Endogenous Viral Elements Lecture 2Document3 pagesEndogenous Viral Elements Lecture 2Aishwarya SinghNo ratings yet
- Virus Phylogenetics and Evolution - Principles and Applications LectureDocument4 pagesVirus Phylogenetics and Evolution - Principles and Applications LectureAishwarya SinghNo ratings yet
- Intro DBMDocument2 pagesIntro DBMAishwarya SinghNo ratings yet
- Lecture 1 The Mechanisms and Consequences of T Cell Activation, With Reference To Signaling, Differentiation and MemoryDocument3 pagesLecture 1 The Mechanisms and Consequences of T Cell Activation, With Reference To Signaling, Differentiation and MemoryAishwarya SinghNo ratings yet
- Introduction 1Document3 pagesIntroduction 1Aishwarya SinghNo ratings yet
- Thyroid Hormone SummaryDocument11 pagesThyroid Hormone SummaryAishwarya SinghNo ratings yet
- Healthy Ice CreamDocument1 pageHealthy Ice CreamAishwarya SinghNo ratings yet
- Lecture 2 Dendritic CellsDocument4 pagesLecture 2 Dendritic CellsAishwarya SinghNo ratings yet
- SARS-CoV-2 and Covid19 Lecture 3Document4 pagesSARS-CoV-2 and Covid19 Lecture 3Aishwarya SinghNo ratings yet
- What Is Biopharmaceutics?: Brand NameDocument10 pagesWhat Is Biopharmaceutics?: Brand NameAhmad Jamal HashmiNo ratings yet
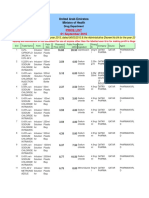
- MOH Medicines Price List For Official Use As On 1st of Sep 2016Document579 pagesMOH Medicines Price List For Official Use As On 1st of Sep 2016Sajitha SujeeshNo ratings yet
- MG Pharnmachieve QuestionsDocument28 pagesMG Pharnmachieve QuestionsSylvia AmakaNo ratings yet
- ĐÁP ÁN TIẾNG ANH CHUYÊN NGÀNHDocument12 pagesĐÁP ÁN TIẾNG ANH CHUYÊN NGÀNHLinh PhạmNo ratings yet
- High Alert Medications 2018Document30 pagesHigh Alert Medications 2018Eman MohamedNo ratings yet
- Urologsep 15Document145 pagesUrologsep 15handryhuaNo ratings yet
- Medical Surgical Skills Checklist PDFDocument5 pagesMedical Surgical Skills Checklist PDFHussain R Al-MidaniNo ratings yet
- The Use of Subcutaneous Omeprazole in The Treatment of Dyspepsia in Palliative Care PatientsDocument3 pagesThe Use of Subcutaneous Omeprazole in The Treatment of Dyspepsia in Palliative Care PatientscarinasheliapNo ratings yet
- Radiation Therapy and Esophageal CancerDocument14 pagesRadiation Therapy and Esophageal Cancerkrsna2studyNo ratings yet
- Complementary and Alternative Medicine - LectureDocument41 pagesComplementary and Alternative Medicine - LecturekitcathNo ratings yet
- Vendedores 01-12-22 ExcelDocument54 pagesVendedores 01-12-22 ExcelDaniel Gonzalez Amaro100% (1)
- Ultiva (Remifentanil) Side Effects, Interactions, Warning, Dosage & Uses PDFDocument1 pageUltiva (Remifentanil) Side Effects, Interactions, Warning, Dosage & Uses PDFcarlnoinNo ratings yet
- Chokde Hudierez - Virtual Hospital Pharmacy Internship JournalDocument5 pagesChokde Hudierez - Virtual Hospital Pharmacy Internship JournalCHOKDE HUDIEREZNo ratings yet
- AsthmaDocument2 pagesAsthmaMarya Fanta C LupuNo ratings yet
- Ethic LectureDocument4 pagesEthic LectureKAMAL ALSOFIANYNo ratings yet
- GCC Guidelines For Ectd SubmissionDocument18 pagesGCC Guidelines For Ectd SubmissionSatadal Deb RoyNo ratings yet
- Rak 4.1Document14 pagesRak 4.1Apotik Karya SehatNo ratings yet
- DRUG Plasil (Metoclopra Mide)Document2 pagesDRUG Plasil (Metoclopra Mide)rholiboi0% (1)
- CH1 Pharma AssignmentDocument3 pagesCH1 Pharma AssignmentJayson Cruz100% (10)
- A Current Review of Cytochrome P450 Interactions of Psychotropic DrugsDocument19 pagesA Current Review of Cytochrome P450 Interactions of Psychotropic Drugsdrguillermomedina100% (1)
- Guidance On Converting Between Anticoagulant RegimensDocument4 pagesGuidance On Converting Between Anticoagulant Regimenskratai NNo ratings yet
- Cloxacillin, Sodium: How Should I Take Cloxacillin?Document7 pagesCloxacillin, Sodium: How Should I Take Cloxacillin?Stacy MC PelitoNo ratings yet
- Au 31 Februari 2017Document149 pagesAu 31 Februari 2017Agnes CynthiaNo ratings yet
- Pharmacy Time Table 2023-2024 1st IsseDocument8 pagesPharmacy Time Table 2023-2024 1st IsseIhtisham SafdarNo ratings yet
- Pharmacology Clear and Simple A Guide To Drug Classifications and Dosage Calculations 2nd Edition Watkins Solutions ManualDocument4 pagesPharmacology Clear and Simple A Guide To Drug Classifications and Dosage Calculations 2nd Edition Watkins Solutions ManualJamesJoFrancis100% (1)
- Exemestane: Adverse Reactions PharmacokineticsDocument1 pageExemestane: Adverse Reactions PharmacokineticsThe ForumNo ratings yet
- Harga ManualDocument114 pagesHarga ManualRini OktaNo ratings yet
- Prodrug Design PDFDocument29 pagesProdrug Design PDFmehulpatel100% (1)
- Programmes in TamilnaduDocument3 pagesProgrammes in Tamilnadudhandapani_kcNo ratings yet
- Toxicidd de Anestesicos Locales1Document6 pagesToxicidd de Anestesicos Locales1Sintia Andrea Peñaloza FernándezNo ratings yet