You might also like
- ckhxtyxsz0ff1o4quch43bvqb-fighting-communicable-diseases-subcommittee-briefingDocument4 pagesckhxtyxsz0ff1o4quch43bvqb-fighting-communicable-diseases-subcommittee-briefingjakuraimanetayNo ratings yet
- Global Health Security Through International Health RegulationsDocument7 pagesGlobal Health Security Through International Health RegulationssarsulthaNo ratings yet
- WHO BAR Topic 2Document8 pagesWHO BAR Topic 2Natasha FrancisNo ratings yet
- Who CDS 2005.29 PDFDocument64 pagesWho CDS 2005.29 PDFrizky yuza ananDANo ratings yet
- Ebola Virus Disease: A Manual for EVD ManagementFrom EverandEbola Virus Disease: A Manual for EVD ManagementMarta LadoNo ratings yet
- Natural Hazards-PandemicsDocument15 pagesNatural Hazards-PandemicsMalina CucoradaNo ratings yet
- Diseases Cause Extinction: Are We Prepared for the Next Global PandemicDocument46 pagesDiseases Cause Extinction: Are We Prepared for the Next Global PandemicaesopwNo ratings yet
- Living in a Void: How the Coronavirus Pandemic affected our LivesFrom EverandLiving in a Void: How the Coronavirus Pandemic affected our LivesNo ratings yet
- X Disease WHODocument3 pagesX Disease WHOEvangelina RivarolaNo ratings yet
- Health Plaque and Policy: Risk Communication For Global Outbreak Management: Ebola Case StudyDocument9 pagesHealth Plaque and Policy: Risk Communication For Global Outbreak Management: Ebola Case StudyDewi AyseNo ratings yet
- The End of Epidemics: how to stop viruses and save humanity nowFrom EverandThe End of Epidemics: how to stop viruses and save humanity nowNo ratings yet
- ARTICLE Zakialevel - DoxDocument12 pagesARTICLE Zakialevel - DoxZakia AmreenNo ratings yet
- Ebola in West AfricaDocument2 pagesEbola in West Africavictorubong404No ratings yet
- A Historical Exploration of Pandemics of Some Selected Diseases in The WorldDocument6 pagesA Historical Exploration of Pandemics of Some Selected Diseases in The Worldbe MominNo ratings yet
- Coronavirus Uncovered: What You Need to Know to Be ProtectedFrom EverandCoronavirus Uncovered: What You Need to Know to Be ProtectedNo ratings yet
- Emerging and Reemerging Infectious DiseasesDocument13 pagesEmerging and Reemerging Infectious DiseasesSayu100% (1)
- Can We Even Define What WHO Member States Are Voting ForDocument7 pagesCan We Even Define What WHO Member States Are Voting FortwisteddickNo ratings yet
- Module 10-CWDocument9 pagesModule 10-CWJayson Delos SantosNo ratings yet
- The Coronavirus Conspiracy: An Exercise in Mass Fear and Mind ControlFrom EverandThe Coronavirus Conspiracy: An Exercise in Mass Fear and Mind ControlNo ratings yet
- Independent Research Paper PlagueDocument17 pagesIndependent Research Paper Plagueapi-413567964No ratings yet
- Lesson 1 - Who Global Health SituationDocument5 pagesLesson 1 - Who Global Health SituationA CNo ratings yet
- Anchit Raut HV EssayDocument19 pagesAnchit Raut HV EssayAnchit RautNo ratings yet
- Nur310 Health Impact FrameworkDocument7 pagesNur310 Health Impact Frameworkapi-449016971No ratings yet
- Use Only: COVID-19 Pandemic: Emerging Perspectives and Future TrendsDocument8 pagesUse Only: COVID-19 Pandemic: Emerging Perspectives and Future TrendsAmin TabishNo ratings yet
- Cholera Outbreaks in Sub Saharan AfricaDocument7 pagesCholera Outbreaks in Sub Saharan AfricaMamadou CoulibalyNo ratings yet
- IMPACT OF COVID-19 PANDEMICDocument7 pagesIMPACT OF COVID-19 PANDEMICJustine Kylle AberinNo ratings yet
- The Ebola Emergency - Immediate Action and Ongoing Strategy - Ferrar and Piot in NEJMDocument2 pagesThe Ebola Emergency - Immediate Action and Ongoing Strategy - Ferrar and Piot in NEJMandrek82No ratings yet
- Prepared And Prevailing: A Comprehensive Handbook for the Post-COVID-19From EverandPrepared And Prevailing: A Comprehensive Handbook for the Post-COVID-19No ratings yet
- UGBS Working Paper Series 01-2021Document19 pagesUGBS Working Paper Series 01-2021maxiluuvNo ratings yet
- Jamaophthalmology Sommer 2020 Ic 200013 PDFDocument2 pagesJamaophthalmology Sommer 2020 Ic 200013 PDFfaisaladeNo ratings yet
- Lecture 8Document15 pagesLecture 8Engr XsadNo ratings yet
- Adiong Thesis Semi-FinalDocument20 pagesAdiong Thesis Semi-FinalWalter MamadNo ratings yet
- Running Head: Community Health and Population-Focused Nursing 1Document7 pagesRunning Head: Community Health and Population-Focused Nursing 1Best EssaysNo ratings yet
- Global Pandemics and Human Security - Docx Research Article 2Document14 pagesGlobal Pandemics and Human Security - Docx Research Article 2quratNo ratings yet
- Covid 19-ResearchDocument9 pagesCovid 19-ResearchBravo,Jessy Anne G.No ratings yet
- 10 Biggest Threats To Global Disease in 2019Document14 pages10 Biggest Threats To Global Disease in 2019sitaNo ratings yet
- Implications of Human Activities For Emegging Infectious DiseasesDocument12 pagesImplications of Human Activities For Emegging Infectious DiseasesVeliborNo ratings yet
- COVID-19 AFRICA, HAITI, AND THE U. S. VIRGIN ISLANDS:: The Response, the Aftermath, & Future ProjectionsFrom EverandCOVID-19 AFRICA, HAITI, AND THE U. S. VIRGIN ISLANDS:: The Response, the Aftermath, & Future ProjectionsNo ratings yet
- Movie Analysis (Contagion 2011)Document14 pagesMovie Analysis (Contagion 2011)Erika ZalamedaNo ratings yet
- Research ArticleDocument4 pagesResearch ArticleDinda AzzahraNo ratings yet
- Running Head: Community Health and Population-Focused Nursing 1Document6 pagesRunning Head: Community Health and Population-Focused Nursing 1Best EssaysNo ratings yet
- Pandemic 3Document8 pagesPandemic 3api-610300472No ratings yet
- Pandemic of DiseaseDocument16 pagesPandemic of DiseasePranjali ThakurNo ratings yet
- Reflection Paper #3Document2 pagesReflection Paper #3Marc Jalen ReladorNo ratings yet
- Session 5 - Pandemics 2023Document31 pagesSession 5 - Pandemics 2023Mashita Fajri MaysuraNo ratings yet
- Ebola VirusDocument14 pagesEbola Virusrama hanggara dNo ratings yet
- ZOOL 143 Topic 1Document8 pagesZOOL 143 Topic 1nattydreadfathelahNo ratings yet
- A Simple Guide To Pandemics, Diagnosis, Treatment And Related ConditionsFrom EverandA Simple Guide To Pandemics, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Nejm 09-04-2015Document107 pagesNejm 09-04-2015Javier B GreenNo ratings yet
- FMSC Research - TB and HivDocument11 pagesFMSC Research - TB and Hivapi-608287742No ratings yet
- Charla Virus LiptonDocument5 pagesCharla Virus Liptonterapiasbreves2012No ratings yet
- COVID-19 Key To Prevention & Survival: 1, #1From EverandCOVID-19 Key To Prevention & Survival: 1, #1Rating: 5 out of 5 stars5/5 (1)
- The Spread, Treatment, and Prevention of HIV-1: Evolution of A Global PandemicDocument12 pagesThe Spread, Treatment, and Prevention of HIV-1: Evolution of A Global PandemicLatiefah NWNo ratings yet
- International Journal of Infectious Diseases: G.G. SimonDocument4 pagesInternational Journal of Infectious Diseases: G.G. Simonlucasdesouza2No ratings yet
- 93 Codex Alimentarius CommissionDocument165 pages93 Codex Alimentarius Commissioncpinto39No ratings yet
- Daftar Obat Floorstock RuanganDocument3 pagesDaftar Obat Floorstock Ruangandini mahdianiNo ratings yet
- WHO STAGE Advisory Group Discusses Mitigating COVID-19 Impacts on MNCAHNDocument33 pagesWHO STAGE Advisory Group Discusses Mitigating COVID-19 Impacts on MNCAHNAbebe TilahunNo ratings yet
- BencinDocument4 pagesBencinimtiazbscNo ratings yet
- Po 2021 FebruariDocument28 pagesPo 2021 FebruariNila Permata SariNo ratings yet
- Patients Rights: Presented By: Ederlyn Papa-Destura, RN, ManDocument57 pagesPatients Rights: Presented By: Ederlyn Papa-Destura, RN, ManteuuuuNo ratings yet
- Supervisi Apoteker (Icu)Document24 pagesSupervisi Apoteker (Icu)Erin FatmawatiNo ratings yet
- Nestle Infant Formula Controversy ExplainedDocument3 pagesNestle Infant Formula Controversy ExplainedChristine Leal-EstenderNo ratings yet
- WHO 2019 NCoV Vaccine Deployment 2020Document89 pagesWHO 2019 NCoV Vaccine Deployment 2020jadwongscribdNo ratings yet
- TISS Placement Brochure 2013-15Document88 pagesTISS Placement Brochure 2013-15Dharam MeenaNo ratings yet
- Quality of TBHIV Data Reported by Health Facilities in UgandaDocument117 pagesQuality of TBHIV Data Reported by Health Facilities in UgandastevekonahNo ratings yet
- Stock TSJ 020823Document17 pagesStock TSJ 020823APOTEK K24 JAKALNo ratings yet
- Medicamentos Orales, Suspension, E Inalados (Nacionalizados)Document6 pagesMedicamentos Orales, Suspension, E Inalados (Nacionalizados)Daniel PerezNo ratings yet
- Export Data Obat 4 Satuan 20210602200832Document2,090 pagesExport Data Obat 4 Satuan 20210602200832merlaapril25No ratings yet
- Obat Topical2Document43 pagesObat Topical2nurwahidaNo ratings yet
- Suicide PreventionDocument34 pagesSuicide PreventionanirudhNo ratings yet
- Daftar List Harga Obat Spesialis Penyakit DalamDocument4 pagesDaftar List Harga Obat Spesialis Penyakit DalamWanty Nur IndahNo ratings yet
- Rwanda Medicaments EssentielsDocument85 pagesRwanda Medicaments EssentielsportosinNo ratings yet
- Ghid OMS CANCER PDFDocument160 pagesGhid OMS CANCER PDFm_manuela2002No ratings yet
- 1st Day Lecture - CHN 2 PDFDocument6 pages1st Day Lecture - CHN 2 PDFR-Chian Jose GermanpNo ratings yet
- Global Patient Safety Challenge - WHODocument35 pagesGlobal Patient Safety Challenge - WHOjoaopinheiro88No ratings yet
- List of AntibioticsDocument9 pagesList of Antibioticsdesi_mNo ratings yet
- How Globalization and Disease Spread Have Increased Focus on Global HealthDocument2 pagesHow Globalization and Disease Spread Have Increased Focus on Global HealthDeomar Joseph ParadoNo ratings yet
- Daftar Obat High Alert Dan LasaDocument1 pageDaftar Obat High Alert Dan LasaDwinda Juli sandaniNo ratings yet
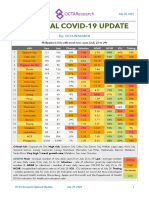
- National COVID-19 Update by Octa Research On July 30, 2021Document2 pagesNational COVID-19 Update by Octa Research On July 30, 2021RapplerNo ratings yet
- Dialyzable MedsDocument2 pagesDialyzable MedsMerry Janne RebolesNo ratings yet
- Sepulveda 2002 Paliative Care Who PerspectiveDocument6 pagesSepulveda 2002 Paliative Care Who PerspectiveDaniela MunteleNo ratings yet
- Aji GantengDocument76 pagesAji GantengAdjie Sastra NegaraNo ratings yet
- 01-15 Maret 2021Document21 pages01-15 Maret 2021Medika AntapaniNo ratings yet
- Quarter Iii Week 1 - Module: Health Trends, Issues and Concern (Global Level)Document55 pagesQuarter Iii Week 1 - Module: Health Trends, Issues and Concern (Global Level)Mark Jay Bongolan100% (1)