You might also like
- Community Health Workers Promote Civic Engagement and Organizational Capacity To Impact PolicyDocument13 pagesCommunity Health Workers Promote Civic Engagement and Organizational Capacity To Impact Policygujjar gujjarNo ratings yet
- Better Outcomes Lower Costs FSG&GIH Spring 2012Document18 pagesBetter Outcomes Lower Costs FSG&GIH Spring 2012iggybauNo ratings yet
- Community Participation: Concept PaperDocument5 pagesCommunity Participation: Concept PaperShahidul Islam ChowdhuryNo ratings yet
- TrendsDocument10 pagesTrendsJoharahNo ratings yet
- Journal Reading 3Document9 pagesJournal Reading 3Ronaly Angalan TinduganNo ratings yet
- Were Already Doing This Work Ethical Research With Communitybased OrganizationsBMC Medical Research MethodologyDocument10 pagesWere Already Doing This Work Ethical Research With Communitybased OrganizationsBMC Medical Research MethodologyNoelia DemanuelNo ratings yet
- Community Engagement:: A Summary of Theoretical ConceptsDocument22 pagesCommunity Engagement:: A Summary of Theoretical ConceptsJaime ApostolNo ratings yet
- HPPN Abstracts (16 March 2010)Document8 pagesHPPN Abstracts (16 March 2010)hppnukNo ratings yet
- Community Based HealthDocument11 pagesCommunity Based HealthAmira Fatmah QuilapioNo ratings yet
- Health Promot Pract-2004-Yoo-256-65 PDFDocument11 pagesHealth Promot Pract-2004-Yoo-256-65 PDFtaintedmelodyNo ratings yet
- The Role of Research in The Right To Health and The Universal Provision of Health CareDocument5 pagesThe Role of Research in The Right To Health and The Universal Provision of Health CareClaudio Gruber MannNo ratings yet
- Jurnal Nomor 17Document18 pagesJurnal Nomor 17Agusniko SinagaNo ratings yet
- Ethical Considerations in Public Health Practice ADocument13 pagesEthical Considerations in Public Health Practice AStela StoychevaNo ratings yet
- Health Care Equity Tool Kit for Developing Winning PolicyDocument25 pagesHealth Care Equity Tool Kit for Developing Winning PolicyDenden Alicias100% (1)
- Analyzing The Landscape: Community Organizing and Health EquityDocument16 pagesAnalyzing The Landscape: Community Organizing and Health EquityDeddy DarmawanNo ratings yet
- Clarifying Conceptual Gaps in Community Participation for Rural Primary Health CareDocument13 pagesClarifying Conceptual Gaps in Community Participation for Rural Primary Health CareADRIANIUSNo ratings yet
- Community HealthDocument4 pagesCommunity HealthJennifer SamsonNo ratings yet
- Institutional Analysis of Health System Governance: Seye Abimbola, Joel Negin, Alexandra L Martiniuk and Stephen JanDocument8 pagesInstitutional Analysis of Health System Governance: Seye Abimbola, Joel Negin, Alexandra L Martiniuk and Stephen JanDr. Kashif HussainNo ratings yet
- Health Seeking BehaviourDocument27 pagesHealth Seeking BehaviourRommel IrabagonNo ratings yet
- DentatoCraigSmith 1 - LibreDocument12 pagesDentatoCraigSmith 1 - LibreMzee KodiaNo ratings yet
- Theorizing Participation in Health Promotion A Literature ReviewDocument6 pagesTheorizing Participation in Health Promotion A Literature ReviewaflsqyljmNo ratings yet
- Public Health Interventions (Population-Based)Document3 pagesPublic Health Interventions (Population-Based)salsabila adinda100% (1)
- Healthy Public Policy AdvocacyDocument3 pagesHealthy Public Policy AdvocacyLuo MiyandaNo ratings yet
- Age Friendly Communities or Austerity Friendly Communities - TorontoDocument9 pagesAge Friendly Communities or Austerity Friendly Communities - Torontoisabela3bastos-1No ratings yet
- Advocacy & LobbyingDocument24 pagesAdvocacy & LobbyingS.Rengasamy100% (4)
- Abers Networks10.1080@19460171.2020.1860782Document21 pagesAbers Networks10.1080@19460171.2020.1860782Diego LemboNo ratings yet
- Population Health Systems Kingsfund Feb15Document40 pagesPopulation Health Systems Kingsfund Feb15Anonymous IUFzAW9wHGNo ratings yet
- XasxcDocument8 pagesXasxcPetronela NistorNo ratings yet
- ADocument22 pagesAadskhanNo ratings yet
- Social Factors Influencing Individual and Population Health - EditedDocument6 pagesSocial Factors Influencing Individual and Population Health - EditedOkoth OluochNo ratings yet
- Co-Production, Co-Creation and Healthy Change: A Critical Friendly PerspectiveDocument14 pagesCo-Production, Co-Creation and Healthy Change: A Critical Friendly PerspectiveNCVONo ratings yet
- Town and Gown Collaboration: A Practical PerspectiveDocument10 pagesTown and Gown Collaboration: A Practical PerspectivemperezfresnoNo ratings yet
- Essential ArticleDocument16 pagesEssential Articleapi-708352337No ratings yet
- Understanding A Community-Led Approach To Health ImprovementDocument37 pagesUnderstanding A Community-Led Approach To Health ImprovementDori DoriNo ratings yet
- Developing Political CompetenceDocument6 pagesDeveloping Political CompetencernrmmanphdNo ratings yet
- PublicDocument12 pagesPublicJayapriya jayaramanNo ratings yet
- Law and urban governance key to closing health equity gapsDocument9 pagesLaw and urban governance key to closing health equity gapsGetachew YematawNo ratings yet
- Broadening Participation in CommunityDocument34 pagesBroadening Participation in CommunityEdgarsito AyalaNo ratings yet
- WK1 - Community Engagement - Definitions and Organizing Concepts From The LiteratureDocument7 pagesWK1 - Community Engagement - Definitions and Organizing Concepts From The LiteratureShaiNo ratings yet
- Strategic Alliances The Role of Civil Society in HealthDocument12 pagesStrategic Alliances The Role of Civil Society in HealthKunal YadavNo ratings yet
- FTPRO204BAssignment1Myat Thu 32813747Document7 pagesFTPRO204BAssignment1Myat Thu 32813747Myat ThuNo ratings yet
- Community Engagement, Solidarity and CitizenshipDocument22 pagesCommunity Engagement, Solidarity and CitizenshipJaydee Joyce Dalligos Mercado80% (49)
- Health Movement in IndiaDocument4 pagesHealth Movement in IndiasanjnuNo ratings yet
- Strategies To Empower Communities To Reduce Health DisparitiesDocument5 pagesStrategies To Empower Communities To Reduce Health DisparitiesNur KholidahNo ratings yet
- Sexual Health in The Philippines Community Engagement ProposalDocument13 pagesSexual Health in The Philippines Community Engagement ProposalDensel MacalintalNo ratings yet
- Final DraftDocument10 pagesFinal Draftapi-708917177No ratings yet
- 369-Article Text-3770-2-10-20190821 PDFDocument16 pages369-Article Text-3770-2-10-20190821 PDFCIR EditorNo ratings yet
- Applying Critical Systems Thinking To Social Prescribing 2072891232326019Document14 pagesApplying Critical Systems Thinking To Social Prescribing 2072891232326019Sophie PonomariovaNo ratings yet
- 10 Social Participation - Issues of Gender, Weaker Sections and Environment PDFDocument18 pages10 Social Participation - Issues of Gender, Weaker Sections and Environment PDFavi nashNo ratings yet
- Journal About CHNDocument2 pagesJournal About CHNAmira Fatmah QuilapioNo ratings yet
- Community OrganizationDocument8 pagesCommunity Organizationantony.barazaNo ratings yet
- Dai Et Al 2017 Publicity Strategies and Media Logic - Communications Campaigns of eNGOS in ChinaDocument17 pagesDai Et Al 2017 Publicity Strategies and Media Logic - Communications Campaigns of eNGOS in ChinaFaye Yan ZhangNo ratings yet
- Models For Developing Community Organizations To Reinforce Health Management in Small BusinessesDocument11 pagesModels For Developing Community Organizations To Reinforce Health Management in Small BusinessesSoleil Sierra ReigoNo ratings yet
- Community Engagement in Public Health: A Conceptual Framework and Real-Life ExamplesDocument8 pagesCommunity Engagement in Public Health: A Conceptual Framework and Real-Life Examplesrifka yoesoefNo ratings yet
- Science and Health Com CollegeDocument14 pagesScience and Health Com CollegeJeyyNo ratings yet
- Collaborative For Community Wellness Mental Health Report Executive SummaryDocument8 pagesCollaborative For Community Wellness Mental Health Report Executive SummaryThe Daily LineNo ratings yet
- Holman HealthRes 2021Document15 pagesHolman HealthRes 2021Salome Valencia AguirreNo ratings yet
- Inge Petersen and Kim Baillie: University of Kwazulu-NatalDocument20 pagesInge Petersen and Kim Baillie: University of Kwazulu-NatalJamesNo ratings yet
- E HealthChapterDocument32 pagesE HealthChapterCiencia, Salud y Género URJCNo ratings yet
- Hpeb 553 Fall 2021 07-24-2021 1Document9 pagesHpeb 553 Fall 2021 07-24-2021 1api-661484626No ratings yet
- Mental Health Doesnt Have To Be SpookyDocument4 pagesMental Health Doesnt Have To Be Spookyapi-661484626No ratings yet
- Hpeb301 Syllabus 2021 QbrownDocument6 pagesHpeb301 Syllabus 2021 Qbrownapi-661484626No ratings yet
- Minorities and Mental Health Event ProposalDocument9 pagesMinorities and Mental Health Event Proposalapi-661484626No ratings yet
- WGST 113 Online SP 2021 Syllabus KLDocument12 pagesWGST 113 Online SP 2021 Syllabus KLapi-661484626No ratings yet
- F 51 Ea 22 CF 1 Ad 9 F 420 CB 6Document7 pagesF 51 Ea 22 CF 1 Ad 9 F 420 CB 6api-661484626No ratings yet
- Key Insights Chart LeadershipDocument1 pageKey Insights Chart Leadershipapi-661484626No ratings yet
- Max Life Smart Secure Plus Plan Features SnapshotDocument40 pagesMax Life Smart Secure Plus Plan Features Snapshotvinayak kbNo ratings yet
- The Bluff Estate - Information Memo PDFDocument51 pagesThe Bluff Estate - Information Memo PDFDaniel VeldhovenNo ratings yet
- D096673877 7117287603297891 SchedulescDocument3 pagesD096673877 7117287603297891 SchedulescrakeshNo ratings yet
- Managing Business Finance During Challenging TimesDocument36 pagesManaging Business Finance During Challenging TimesYong Chun WahNo ratings yet
- Income Tax Declaration Form FY 22 23 AY 23 24Document2 pagesIncome Tax Declaration Form FY 22 23 AY 23 24kishoreNo ratings yet
- Icea Umbrella PF Proposal - Emergency Hospital EntebbeDocument16 pagesIcea Umbrella PF Proposal - Emergency Hospital EntebbeMBUSA JOHNNo ratings yet
- IAS 19 SummaryDocument6 pagesIAS 19 SummaryMuchaa VlogNo ratings yet
- How marketing helps businesses and the economyDocument39 pagesHow marketing helps businesses and the economyKeerthi Ganesan100% (1)
- GCAP - EnglishDocument2 pagesGCAP - EnglishJITENDRANo ratings yet
- Roles and Responsibilities of UnderwritingDocument6 pagesRoles and Responsibilities of UnderwritingShubham DubeyNo ratings yet
- Sec Form DDocument8 pagesSec Form DColin RamNo ratings yet
- 1.1. Principles of General InsuranceDocument22 pages1.1. Principles of General Insurancebeena antuNo ratings yet
- Association of Average Adjusters RulesDocument20 pagesAssociation of Average Adjusters RulesJohanes Alverandy AriowibowoNo ratings yet
- En AR Group Annual Report Allianz 2019Document180 pagesEn AR Group Annual Report Allianz 2019Sabina MunteanuNo ratings yet
- 837 Dental Ion GuideDocument440 pages837 Dental Ion GuidejxwjwalanNo ratings yet
- People's Trans East v. Doctors of New MillenniumDocument3 pagesPeople's Trans East v. Doctors of New MillenniumJayson RacalNo ratings yet
- Plan Comparison ChartDocument3 pagesPlan Comparison ChartBassoNo ratings yet
- ENG Lista Ubezpieczycieli I Oferowanych Produktów Ubezpieczeniowych Nowelizacja Uoc 30052023Document17 pagesENG Lista Ubezpieczycieli I Oferowanych Produktów Ubezpieczeniowych Nowelizacja Uoc 30052023Rusi VakaNo ratings yet
- Opt, Excise Tax and DSTDocument4 pagesOpt, Excise Tax and DSTHiedi SugamotoNo ratings yet
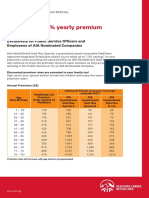
- Enjoy Up To 7.3% Yearly Premium DiscountDocument2 pagesEnjoy Up To 7.3% Yearly Premium DiscountAlvin WangNo ratings yet
- Dia Mae A. Generoso - Learning Activity 3Document10 pagesDia Mae A. Generoso - Learning Activity 3Dia Mae Ablao GenerosoNo ratings yet
- Revere JournalDocument28 pagesRevere JournalalexanneseNo ratings yet
- Pdic LawDocument30 pagesPdic LawDadangNo ratings yet
- ICWIM Ed 4Document403 pagesICWIM Ed 4Tarek ElzayatNo ratings yet
- Eric Ripoli, CPA: Professional SummaryDocument4 pagesEric Ripoli, CPA: Professional Summarykiran2710No ratings yet
- Guide To Fenero Contractor SolutionDocument13 pagesGuide To Fenero Contractor SolutionnonitathomasNo ratings yet
- Chapter 2Document86 pagesChapter 2Halid Habtamu100% (1)
- Module 2 - Intro To Healthcare MarketingDocument14 pagesModule 2 - Intro To Healthcare MarketingMilan FantasyNo ratings yet
- 3001 A 184552264 00 B00 PyDocument2 pages3001 A 184552264 00 B00 PyRaghu DsNo ratings yet
- V2 Exam 1 PMDocument29 pagesV2 Exam 1 PMMaharishi VaidyaNo ratings yet