You might also like
- Immunisation HandbookDocument546 pagesImmunisation HandbookPritam Dugar100% (1)
- Wisdom Chi KungDocument0 pagesWisdom Chi KungDevlinPyxNo ratings yet
- Quiz RespiratoryDocument123 pagesQuiz RespiratoryMedShare100% (23)
- 109 Upper Extremity Questions and AnswersDocument8 pages109 Upper Extremity Questions and AnswersChioma BenedetteNo ratings yet
- ATI NotesDocument16 pagesATI NotesMei Sarte100% (1)
- TEST - Cancer-ParasiteDocument41 pagesTEST - Cancer-ParasiteRazvan Andrei ValcuNo ratings yet
- Algorithm - Managing A COPD Exacerbation in Primary CareDocument1 pageAlgorithm - Managing A COPD Exacerbation in Primary Caremufidah mawaddahNo ratings yet
- The 13 Remedies of DR John Henry Clarke: SULPHUR (Brimstone Flowers of Sulphur.)Document20 pagesThe 13 Remedies of DR John Henry Clarke: SULPHUR (Brimstone Flowers of Sulphur.)Anonymous eKt1FCDNo ratings yet
- ASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFDocument8 pagesASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFAyu WahyuniNo ratings yet
- Study Guide For Med Surg 1Document15 pagesStudy Guide For Med Surg 1desireemaenugentNo ratings yet
- Pedia ReviewerDocument27 pagesPedia ReviewerEvangeline GoNo ratings yet
- ASCIA Guidelines Acute Management Anaphylaxis 2019Document8 pagesASCIA Guidelines Acute Management Anaphylaxis 2019Asadulla KhanNo ratings yet
- Peripheral Neuropathy HandoutDocument16 pagesPeripheral Neuropathy HandoutTatiana IonascuNo ratings yet
- Case Pres CellulitisDocument97 pagesCase Pres CellulitischelybabyjynxNo ratings yet
- DR Mwanzas Pediatric Protocols 2017Document143 pagesDR Mwanzas Pediatric Protocols 2017Mwambazi MathewsNo ratings yet
- Integrated Prevention and Management of Selected Acute and Chronic Illness (IPMSACI) - Job AidDocument9 pagesIntegrated Prevention and Management of Selected Acute and Chronic Illness (IPMSACI) - Job AidCOMDIS-HSDNo ratings yet
- Management of Medical Complications in Severe Acute Malnutrition (SAM)Document4 pagesManagement of Medical Complications in Severe Acute Malnutrition (SAM)Archana SinghNo ratings yet
- Current Guidelines in Management of DiarrhoeaDocument40 pagesCurrent Guidelines in Management of Diarrhoeaokwadha simionNo ratings yet
- Emergency Pediatric AidsDocument29 pagesEmergency Pediatric AidsRana SalemNo ratings yet
- Flowchart 1 Immediate Management of An AsphyxiatednewbornDocument3 pagesFlowchart 1 Immediate Management of An Asphyxiatednewborndessy pratiwiNo ratings yet
- Flowchart 1 Immediate Management of An Asphyxiated NewbornDocument3 pagesFlowchart 1 Immediate Management of An Asphyxiated Newborndessy pratiwiNo ratings yet
- ASCIA HP Guidelines Acute Management Anaphylaxis 2020Document8 pagesASCIA HP Guidelines Acute Management Anaphylaxis 2020Munshi KamrulNo ratings yet
- Acute Management of Anaphylaxis: Adrenaline (Epinephrine) Is The First Line Treatment For AnaphylaxisDocument8 pagesAcute Management of Anaphylaxis: Adrenaline (Epinephrine) Is The First Line Treatment For AnaphylaxissigmapomalNo ratings yet
- NCLEX LABS +few PointersDocument5 pagesNCLEX LABS +few PointersSNo ratings yet
- Kondisi Yang Mengancam Nyawa Dan Memerlukan Intervensi Yang Agresif SecepatnyaDocument3 pagesKondisi Yang Mengancam Nyawa Dan Memerlukan Intervensi Yang Agresif SecepatnyaAbu QaireenNo ratings yet
- CPG Acute Infectious Diarrhea Pocket Guide v2Document21 pagesCPG Acute Infectious Diarrhea Pocket Guide v2Moonyeen Jann Casera BalicNo ratings yet
- DISEASES CASE MANAGEMENT PROTOCOL Final Draft DTD August 2014-VaidDocument34 pagesDISEASES CASE MANAGEMENT PROTOCOL Final Draft DTD August 2014-VaidferasNo ratings yet
- Approach To Acute Diarrhoea: Dr. Pankaj Kumar Singhal Govt. Medical College, KotaDocument43 pagesApproach To Acute Diarrhoea: Dr. Pankaj Kumar Singhal Govt. Medical College, KotaVandanaNo ratings yet
- Clinical Presentation and Case ManagementDocument34 pagesClinical Presentation and Case ManagementPatrick MukosoNo ratings yet
- 01 - Management of Critically Ill ChildrenDocument42 pages01 - Management of Critically Ill ChildrenMin MinTheinNo ratings yet
- Do'S and Don'Ts For DoctorsDocument4 pagesDo'S and Don'Ts For DoctorsTalha ENo ratings yet
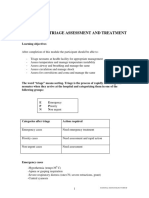
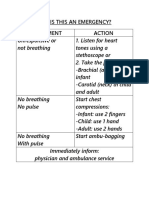
- Emergency Triage Assessment and Treatment: National Neonatology ForumDocument6 pagesEmergency Triage Assessment and Treatment: National Neonatology ForumSatya Prakash TiwariNo ratings yet
- ASCIA Guidelines ADVANCED Acute Management Anaphylaxis Dec2016Document7 pagesASCIA Guidelines ADVANCED Acute Management Anaphylaxis Dec2016SPV DoctorNo ratings yet
- Medical EmergenciesDocument9 pagesMedical EmergenciesThe KittyNo ratings yet
- PHC EmergencyDocument42 pagesPHC Emergencyمحمداحمد محمدنور ابايزيدNo ratings yet
- Triage Emergency Signs and Normal VSDocument4 pagesTriage Emergency Signs and Normal VSbonziebuddyNo ratings yet
- Pediatric Life SupportDocument33 pagesPediatric Life SupportAndre montolaluNo ratings yet
- Stabilization CentreDocument64 pagesStabilization CentreShafaat HussainNo ratings yet
- Akp Important Guidelines 22 Guidlines Brief FinalDocument55 pagesAkp Important Guidelines 22 Guidlines Brief FinalRaheelNo ratings yet
- Ammonia Algorithm v9Document5 pagesAmmonia Algorithm v9Danielle ConcepcionNo ratings yet
- Anaphylaxis Guidance CardsDocument2 pagesAnaphylaxis Guidance CardsElein Datu SeruNo ratings yet
- ASCIA Guidelines Acute Management Anaphylaxis Dec2016Document5 pagesASCIA Guidelines Acute Management Anaphylaxis Dec2016kkkssbbNo ratings yet
- Morning Case Report: October 4th 2011Document22 pagesMorning Case Report: October 4th 2011Felicia adeline ChristianNo ratings yet
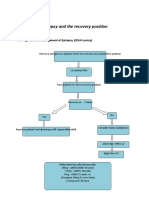
- Epilepsy Recovery Period - Second YrDocument3 pagesEpilepsy Recovery Period - Second YrBrian MaloneyNo ratings yet
- Pediatric Emergencies ?-1Document96 pagesPediatric Emergencies ?-1zahraaNo ratings yet
- Aclspediatric BradycardiaDocument2 pagesAclspediatric BradycardiasalamredNo ratings yet
- OB - Hypertensive DisordersDocument4 pagesOB - Hypertensive DisordersJasmine Nicole RemetreNo ratings yet
- Gut FeelingsDocument70 pagesGut FeelingsAngela MagnoNo ratings yet
- Emergency GuidelinesDocument11 pagesEmergency GuidelineswinstonappsNo ratings yet
- Pedia ReportDocument4 pagesPedia ReportBeda MalecdanNo ratings yet
- Eclampsia PPHDocument43 pagesEclampsia PPHizafamirna743No ratings yet
- Guidelines and Protocols Of: Diabetes EmergenciesDocument36 pagesGuidelines and Protocols Of: Diabetes Emergenciesyassen hassanNo ratings yet
- 3.15 Febrile Child Under 5 Years Without A FocusDocument8 pages3.15 Febrile Child Under 5 Years Without A Focusiffi82No ratings yet
- Chapter 5. Diarrhoea and Severe DehydrationDocument24 pagesChapter 5. Diarrhoea and Severe DehydrationSwarnavo DasNo ratings yet
- Sepsis Flow Chart FinalDocument2 pagesSepsis Flow Chart FinalDevindraPrptNo ratings yet
- Paediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Document14 pagesPaediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Nadia SalwaniNo ratings yet
- DKA Protocol TGDocument11 pagesDKA Protocol TGabelNo ratings yet
- Nursing Care During LaborDocument19 pagesNursing Care During LaborBaniwas Marie AgnesNo ratings yet
- Intravenous Insulin Prescription and Fluid Protocol: For Diabetic Keto-Acidosis (Dka)Document4 pagesIntravenous Insulin Prescription and Fluid Protocol: For Diabetic Keto-Acidosis (Dka)sunrise755No ratings yet
- O&G Off-Tag Assesment Logbook: Traces-Pdf-248732173Document9 pagesO&G Off-Tag Assesment Logbook: Traces-Pdf-248732173niwasNo ratings yet
- Anaphylaxis Wallchart 2018Document1 pageAnaphylaxis Wallchart 2018simranNo ratings yet
- Pediatric Advanced Life Support: Jan Bazner-Chandler CPNP, CNS, MSN, RNDocument65 pagesPediatric Advanced Life Support: Jan Bazner-Chandler CPNP, CNS, MSN, RNد. محمد فريد الغنامNo ratings yet
- Clinical Pathway Peds Sepsis 2012Document3 pagesClinical Pathway Peds Sepsis 2012Kim MedairosNo ratings yet
- Case ReportDocument27 pagesCase ReportRuni ArumndariNo ratings yet
- Pre EclampsiaDocument3 pagesPre EclampsiaStar SingsonNo ratings yet
- ASV - Treatment Protocol.Document5 pagesASV - Treatment Protocol.Kayalvizhi ThirumalNo ratings yet
- Severe Sepsisand Septic Shock GuidelinesDocument17 pagesSevere Sepsisand Septic Shock GuidelinesdrquamrulNo ratings yet
- Individualised Perioperative Open-Lung Approach Versus Standard Protective Ventilation in Abdominal Surgery (IPROVE) - A Randomised Controlled TrialDocument11 pagesIndividualised Perioperative Open-Lung Approach Versus Standard Protective Ventilation in Abdominal Surgery (IPROVE) - A Randomised Controlled TrialVic HNNo ratings yet
- Text Book Reading: Hipoxic Ischaemic EncephalopatyDocument23 pagesText Book Reading: Hipoxic Ischaemic EncephalopatyPanduRespatiNo ratings yet
- CasestudyvaccinesDocument5 pagesCasestudyvaccinesapi-323720899No ratings yet
- FEARS Database-FDA Database of glp1 Disproportionate Adverse EventsDocument20 pagesFEARS Database-FDA Database of glp1 Disproportionate Adverse EventsW Antonio Rivera MartínezNo ratings yet
- MSC Yoga - Semester 2 Hatha Yoga Pradipika - Answers To 10 Marks QuestionsDocument32 pagesMSC Yoga - Semester 2 Hatha Yoga Pradipika - Answers To 10 Marks QuestionsHenrickNo ratings yet
- DiphtheriaDocument1 pageDiphtheriaapi-275493729No ratings yet
- Chronic Renal Failure Due To EhrlichiosiDocument4 pagesChronic Renal Failure Due To EhrlichiosiUNICORN TIMENo ratings yet
- MediPrime Claim FormDocument8 pagesMediPrime Claim Formrahul0105100% (1)
- Steroids PowerPointDocument33 pagesSteroids PowerPointLeeYates340% (1)
- AfflictionsDocument12 pagesAfflictionsshiraaazNo ratings yet
- Health Guard Customer Information Sheet: Bajaj Allianz General Insurance Company LimitedDocument3 pagesHealth Guard Customer Information Sheet: Bajaj Allianz General Insurance Company LimitedKumud GandhiNo ratings yet
- FLM-porto Systemic AnastomosisDocument10 pagesFLM-porto Systemic AnastomosisYusuf Bin ZaidiNo ratings yet
- Thyroid DiseaseDocument30 pagesThyroid Diseasemy Lord JesusNo ratings yet
- Physical Medicine and Therapy. Means of PT. Therapeutic Exercise. Electrotherapy. Balneology and Climate MedicineDocument64 pagesPhysical Medicine and Therapy. Means of PT. Therapeutic Exercise. Electrotherapy. Balneology and Climate MedicineEcaterina GorganNo ratings yet
- Problems in Nutrition and EliminationDocument4 pagesProblems in Nutrition and EliminationBianca BautistaNo ratings yet
- What Is Kidney (Renal) Failure?: Female Urinary TractDocument6 pagesWhat Is Kidney (Renal) Failure?: Female Urinary TractthenameisvijayNo ratings yet
- NCMB316 Lec MidtermDocument28 pagesNCMB316 Lec Midterm2 - GUEVARRA, KYLE JOSHUA M.No ratings yet
- Daun PDFDocument5 pagesDaun PDFDaniel OktavianusNo ratings yet
- Glycogen Storage DiseaseDocument7 pagesGlycogen Storage DiseaseJuliana CorreaNo ratings yet
- CLT ScriptDocument3 pagesCLT ScriptMarioNo ratings yet
- Masumeen (As) - XKP - Duas From TIBB AL a-IMMA - Islamic Medical WisdomDocument124 pagesMasumeen (As) - XKP - Duas From TIBB AL a-IMMA - Islamic Medical WisdomAkbar Ali KhanNo ratings yet
- BoilsDocument48 pagesBoilsPű JäNo ratings yet