You might also like
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- DR Mwanzas Pediatric Protocols 2017Document143 pagesDR Mwanzas Pediatric Protocols 2017Mwambazi MathewsNo ratings yet
- Case ReportDocument27 pagesCase ReportRuni ArumndariNo ratings yet
- Treatment Guidelines: Appendix-1Document25 pagesTreatment Guidelines: Appendix-1CLICK & WATCHNo ratings yet
- Guided by Asso Prof DR Sunil K Agarawalla Presented by DR Minakhi Kumari Sahu (JR-1)Document45 pagesGuided by Asso Prof DR Sunil K Agarawalla Presented by DR Minakhi Kumari Sahu (JR-1)Gobinda Pradhan100% (1)
- Module 6B - ITC ComplicationsDocument36 pagesModule 6B - ITC ComplicationsDexter MasongsongNo ratings yet
- Clinical Features: How Do Youbecome A Carrier of Malaria?Document6 pagesClinical Features: How Do Youbecome A Carrier of Malaria?Ma Sophia LimNo ratings yet
- Acute Diarrhea and Shock in The EDDocument5 pagesAcute Diarrhea and Shock in The EDmohamed fahmyNo ratings yet
- C 2860 Aacbff 1Document9 pagesC 2860 Aacbff 1Muhammad FaizNo ratings yet
- The Case of Ellen TorresDocument4 pagesThe Case of Ellen TorresOmie Calzum YusophNo ratings yet
- Acute GastroenteritisDocument6 pagesAcute GastroenteritisSalman KhanNo ratings yet
- SC GuidlinesDocument54 pagesSC GuidlinesShafaat HussainNo ratings yet
- Dehydration in Peads: Nora Edora Francis PPW 23, Etd Hqe 2Document16 pagesDehydration in Peads: Nora Edora Francis PPW 23, Etd Hqe 2Maman GundohingNo ratings yet
- NOTESDocument4 pagesNOTESEliz Codilla-SyNo ratings yet
- Module 6BDocument40 pagesModule 6BroseannurakNo ratings yet
- Diare: Arlinda Silva Prameswari 201810401011044Document28 pagesDiare: Arlinda Silva Prameswari 201810401011044Lilian Rahma AnandaNo ratings yet
- Protein Calorie MalnutritionDocument97 pagesProtein Calorie Malnutritionnshaikh56No ratings yet
- Approach To Acute Diarrhoea: Dr. Pankaj Kumar Singhal Govt. Medical College, KotaDocument43 pagesApproach To Acute Diarrhoea: Dr. Pankaj Kumar Singhal Govt. Medical College, KotaVandanaNo ratings yet
- Cholera Clin Management ENG Rev JUN 1Document8 pagesCholera Clin Management ENG Rev JUN 1Daniel OktavianusNo ratings yet
- Acute GastroenteritisDocument29 pagesAcute Gastroenteritisjinggalu100% (5)
- Anaphylaxis Wallchart 2022Document1 pageAnaphylaxis Wallchart 2022Aymane El KandoussiNo ratings yet
- Clinical Presentation and Case ManagementDocument34 pagesClinical Presentation and Case ManagementPatrick MukosoNo ratings yet
- Anaphylaxis Wallchart 2018Document1 pageAnaphylaxis Wallchart 2018simranNo ratings yet
- Chidhood Diarrhea 04062014 - 2Document16 pagesChidhood Diarrhea 04062014 - 2Sameera 123No ratings yet
- IMCI UpdatedDocument5 pagesIMCI UpdatedMalak RagehNo ratings yet
- Calf Protocols Ver4Document6 pagesCalf Protocols Ver4Sadam Irshad100% (1)
- Management of Dehydration (Nsgeud)Document3 pagesManagement of Dehydration (Nsgeud)Mary MenuNo ratings yet
- 10 Steps Wall ChartDocument2 pages10 Steps Wall ChartTommy CharwinNo ratings yet
- Flowchart 1 Immediate Management of An AsphyxiatednewbornDocument3 pagesFlowchart 1 Immediate Management of An Asphyxiatednewborndessy pratiwiNo ratings yet
- Emergency Pediatric AidsDocument29 pagesEmergency Pediatric AidsRana SalemNo ratings yet
- SquirtsDocument2 pagesSquirtsRal TibsNo ratings yet
- Sick Young Infants (Referral, Treatment, Oral Drugs) : ImnciDocument46 pagesSick Young Infants (Referral, Treatment, Oral Drugs) : ImnciTanviNo ratings yet
- DIARHEADocument7 pagesDIARHEAahmedmuuseabokorNo ratings yet
- Pharmacological Properties of NDocument2 pagesPharmacological Properties of NMuhammad Salman ZengaNo ratings yet
- Imci Summary Toprank by JadeDocument13 pagesImci Summary Toprank by JadeJade SorongonNo ratings yet
- Alclor: Water Used For Reconstitution Should Be Boiled and CooledDocument1 pageAlclor: Water Used For Reconstitution Should Be Boiled and CooledRubel sheikhNo ratings yet
- Pediatrics: Do Not Forget ENT, Abdomen and Genitals!!Document68 pagesPediatrics: Do Not Forget ENT, Abdomen and Genitals!!Laura GranadosNo ratings yet
- Current Guidelines in Management of DiarrhoeaDocument40 pagesCurrent Guidelines in Management of Diarrhoeaokwadha simionNo ratings yet
- Group 5Document66 pagesGroup 5Cms CSUNo ratings yet
- Fluid and Electrolyte TherapyDocument4 pagesFluid and Electrolyte TherapyKhirren RaoNo ratings yet
- Dr. Shazia Aurangzeb Assistant Professor in Paeds KTHDocument42 pagesDr. Shazia Aurangzeb Assistant Professor in Paeds KTHclaimstudent3515No ratings yet
- IMCI TECHNICAL UPDATES: The KEY To Your Success!! Pls..... Read.. Read.. Read.Document10 pagesIMCI TECHNICAL UPDATES: The KEY To Your Success!! Pls..... Read.. Read.. Read.Kim RamosNo ratings yet
- Session 4: Main SymptomsDocument86 pagesSession 4: Main SymptomszerpthederpNo ratings yet
- 6.1 Quick Ref Guide MNGT Antivenom Reactions SGB2021 Ver. 2Document3 pages6.1 Quick Ref Guide MNGT Antivenom Reactions SGB2021 Ver. 2anju sulishaNo ratings yet
- Who Ten Step Management of Severe MalnutritionDocument4 pagesWho Ten Step Management of Severe MalnutritionShely Karma Astuti33% (3)
- Strategies To Reduce Under 5 Preventable Death in SelangorDocument15 pagesStrategies To Reduce Under 5 Preventable Death in SelangorJoshua Taylor ThomasNo ratings yet
- Neonatal ResuscitationDocument5 pagesNeonatal Resuscitationapi-3712326No ratings yet
- Stabilization CentreDocument64 pagesStabilization CentreShafaat HussainNo ratings yet
- AGE (Updated)Document3 pagesAGE (Updated)Sanielle Karla Garcia LorenzoNo ratings yet
- CholeraDocument1 pageCholeraRevan NasirNo ratings yet
- Flowchart 1 Immediate Management of An Asphyxiated NewbornDocument3 pagesFlowchart 1 Immediate Management of An Asphyxiated Newborndessy pratiwiNo ratings yet
- IMCI Technical UpdatesDocument3 pagesIMCI Technical Updatesmikaela_pascuaNo ratings yet
- Child With Fits in ED - Srl.Document2 pagesChild With Fits in ED - Srl.azeemNo ratings yet
- Laporan Kasus Blok ElektifDocument9 pagesLaporan Kasus Blok ElektifestiNo ratings yet
- Paediatric Protocols FinalDocument33 pagesPaediatric Protocols FinalAbdulkarim Mohamed AbdallaNo ratings yet
- IMCI SumDocument6 pagesIMCI SumLazo JuleeNo ratings yet
- World Health Organization (Who) Guidelines On Treatment of Diarrhea (2005)Document7 pagesWorld Health Organization (Who) Guidelines On Treatment of Diarrhea (2005)Tina AldabaNo ratings yet
- Metabolic Disorders LONG CHAIN FAT OXIDATION DISORDERSDocument5 pagesMetabolic Disorders LONG CHAIN FAT OXIDATION DISORDERSMahmoud khedrNo ratings yet
- Hipoglicemia CodeDocument1 pageHipoglicemia Codeneonatos HSJDNo ratings yet
- IMCI Guideline-2023 HeshamElsayedDocument57 pagesIMCI Guideline-2023 HeshamElsayedMalak Rageh100% (2)
- Second Round Allotment List PG 2019Document38 pagesSecond Round Allotment List PG 2019Archana SinghNo ratings yet
- Xia Abstract and BioDocument1 pageXia Abstract and BioArchana SinghNo ratings yet
- Ibvt08i3p203 PDFDocument12 pagesIbvt08i3p203 PDFMithlesh DewanganNo ratings yet
- Index Medical College, Hospital & Research Centre: 1. Department of AnatomyDocument21 pagesIndex Medical College, Hospital & Research Centre: 1. Department of AnatomyArchana SinghNo ratings yet
- Department of Anaesthesiology: Medical College, Hospital & Research CentreDocument3 pagesDepartment of Anaesthesiology: Medical College, Hospital & Research CentreArchana SinghNo ratings yet
- Multiple Pilomatricomas in The Setting of Myotonic DystrophyDocument3 pagesMultiple Pilomatricomas in The Setting of Myotonic DystrophyArchana SinghNo ratings yet
- Government of India Press Information Bureau Press Note Civil Services Examination, 2020Document16 pagesGovernment of India Press Information Bureau Press Note Civil Services Examination, 2020All In OneNo ratings yet
- Differential Diagnosis of Myotonic Disorders: Aanem MonographDocument7 pagesDifferential Diagnosis of Myotonic Disorders: Aanem MonographArchana SinghNo ratings yet
- WHO CG Table 7.8Document1 pageWHO CG Table 7.8Archana SinghNo ratings yet
- Congenital Myotonic Dystrophy With Asymptomatic Mother: ASE EportsDocument3 pagesCongenital Myotonic Dystrophy With Asymptomatic Mother: ASE EportsArchana SinghNo ratings yet
- Congenital Myotonic Dystrophy With Asymptomatic Mother: ASE EportsDocument3 pagesCongenital Myotonic Dystrophy With Asymptomatic Mother: ASE EportsArchana SinghNo ratings yet
- HD21 Deg PmeritDocument12 pagesHD21 Deg PmeritArchana SinghNo ratings yet
- Hypocalcemia AIIMS PDFDocument19 pagesHypocalcemia AIIMS PDFabhivnairNo ratings yet
- Oculopalatal Myoclonus: Eye Movement Studies, Mri Findings and The Difficulty of TreatmentDocument6 pagesOculopalatal Myoclonus: Eye Movement Studies, Mri Findings and The Difficulty of TreatmentArchana SinghNo ratings yet
- Notice: Ref. U-12021/44/2019/17-MEC Dated: 11-04-2020Document371 pagesNotice: Ref. U-12021/44/2019/17-MEC Dated: 11-04-2020Archana SinghNo ratings yet
- Department of Microbiology Patliputra Medical College, DhanbadDocument3 pagesDepartment of Microbiology Patliputra Medical College, DhanbadArchana SinghNo ratings yet
- Welcome To Xodo: With Xodo You CanDocument11 pagesWelcome To Xodo: With Xodo You CanKindly ReminderNo ratings yet
- L1 Hypo, Hyperthyroidism and Hashimoto ThyroiditisDocument12 pagesL1 Hypo, Hyperthyroidism and Hashimoto ThyroiditisSivaNo ratings yet
- 5th Year Passmedicine Notes 3Document20 pages5th Year Passmedicine Notes 3quojo041No ratings yet
- Introduction & Epidemiology Clinical Features: End-Stage Renal Disease (ESRD)Document2 pagesIntroduction & Epidemiology Clinical Features: End-Stage Renal Disease (ESRD)Nikki VillanuevaNo ratings yet
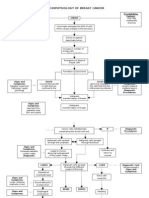
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 pagesPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- CPG Acute Infectious DiarrheaDocument10 pagesCPG Acute Infectious DiarrheaKristine Jade OdtujanNo ratings yet
- Endocrine Disorders PDFDocument55 pagesEndocrine Disorders PDFAkram HusseinNo ratings yet
- NURSING CARE PLAN - Spontaneous AbortionDocument2 pagesNURSING CARE PLAN - Spontaneous Abortionderic97% (36)
- Parameatal Cyst :A Case ReportDocument3 pagesParameatal Cyst :A Case ReportDr.ankit AnandNo ratings yet
- Plasma ExpandersDocument4 pagesPlasma ExpandersNix EnarioNo ratings yet
- Clinical Practicum Worksheet: Nursing Care PlanDocument4 pagesClinical Practicum Worksheet: Nursing Care PlanOrlea Francisco-SisioNo ratings yet
- Manejo de Hipermenorrea en AdolescentesDocument9 pagesManejo de Hipermenorrea en AdolescentesDavid VargasNo ratings yet
- Human Health and DiseaseDocument20 pagesHuman Health and DiseaseA BeheraNo ratings yet
- Viral Meningitis: Current Issues in Diagnosis and TreatmentDocument9 pagesViral Meningitis: Current Issues in Diagnosis and Treatmentrisna sariNo ratings yet
- Scoliosis PDFDocument19 pagesScoliosis PDFdallas100% (1)
- Duodenal GistDocument5 pagesDuodenal Gistmudasir61No ratings yet
- Parenteral Therapy:: Intravenous Therapy (IVT) or VenipunctureDocument3 pagesParenteral Therapy:: Intravenous Therapy (IVT) or VenipunctureMabes100% (1)
- Annex D Health Declaretion FormDocument2 pagesAnnex D Health Declaretion FormMa. Leonora TumamposNo ratings yet
- Peppermint LetterDocument2 pagesPeppermint LetterKelli AdamsNo ratings yet
- Cqi Indicators As Per Nabh 5Th Edition: S. No. Standard Ref. Deptt. KPI Formula FrequencyDocument3 pagesCqi Indicators As Per Nabh 5Th Edition: S. No. Standard Ref. Deptt. KPI Formula FrequencyNatasha Bhasin91% (11)
- 2803NRS Acute Nursing Practice Exam NotesDocument18 pages2803NRS Acute Nursing Practice Exam NotesGrace CallowNo ratings yet
- Evaluation and Treatment of Hypertensive Emergencies in AdultsDocument13 pagesEvaluation and Treatment of Hypertensive Emergencies in Adultsjavier ariasNo ratings yet
- Medical Self Declaration FormDocument1 pageMedical Self Declaration FormVarun SinglaNo ratings yet
- Reading Comprehension: HIVDocument2 pagesReading Comprehension: HIVFlori75% (8)
- ConcorDocument40 pagesConcorviczNo ratings yet
- 2.tukak PeptikDocument42 pages2.tukak PeptikEfvi VhyLiaNo ratings yet
- Pulsatilla NigricansDocument20 pagesPulsatilla NigricansastronayanNo ratings yet
- Vascular Disease and Foot Assessment in Diabetes: Evidence-Based Management 42Document7 pagesVascular Disease and Foot Assessment in Diabetes: Evidence-Based Management 42JULIANINo ratings yet
- Information Sheet 4.1-4: 1. Occupational Health and Safety IndicatorsDocument3 pagesInformation Sheet 4.1-4: 1. Occupational Health and Safety Indicatorsmark ian joverNo ratings yet
- Mansonella StreptocercaDocument14 pagesMansonella StreptocercaALLISON PAMITTANNo ratings yet
- Problem Nursing Diagnosis Background Knowledge Goal and Objective Nursing Intervention Rationale EvaluationDocument2 pagesProblem Nursing Diagnosis Background Knowledge Goal and Objective Nursing Intervention Rationale Evaluationcherrymae mataNo ratings yet