You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Introduction To Public HealthDocument54 pagesIntroduction To Public HealthKristelle Marie Enanoria Bardon50% (2)
- Calcined Clays For Sustainable Concrete Karen Scrivener, AurÇlie Favier, 2015Document552 pagesCalcined Clays For Sustainable Concrete Karen Scrivener, AurÇlie Favier, 2015Débora BretasNo ratings yet
- Average Waves in Unprotected Waters by Anne Tyler - Summary PDFDocument1 pageAverage Waves in Unprotected Waters by Anne Tyler - Summary PDFRK PADHI0% (1)
- Created By: Susan JonesDocument246 pagesCreated By: Susan JonesdanitzavgNo ratings yet
- 1 s2.0 S0009912017307178 MainDocument23 pages1 s2.0 S0009912017307178 MainParishan SaeedNo ratings yet
- 976c5091-5277-4d13-8655-371a2eb3d13fDocument2 pages976c5091-5277-4d13-8655-371a2eb3d13fParishan SaeedNo ratings yet
- Bone Age For Chronological Age Determination - November2018Document4 pagesBone Age For Chronological Age Determination - November2018Parishan SaeedNo ratings yet
- Decreased Ligand Affinity Rather Than Glucocorticoid Receptor Down-Regulation in Patients With Endogenous Cushing's SyndromeDocument5 pagesDecreased Ligand Affinity Rather Than Glucocorticoid Receptor Down-Regulation in Patients With Endogenous Cushing's SyndromeParishan SaeedNo ratings yet
- Quick Reference Guide Endocrine Hypertension 2 2016 VersionDocument16 pagesQuick Reference Guide Endocrine Hypertension 2 2016 VersionParishan SaeedNo ratings yet
- Cortisol II 2020-03 v6Document5 pagesCortisol II 2020-03 v6Parishan SaeedNo ratings yet
- Effect of Knowledge of Chronologic Age On The Variability of Pediatric Bone Age Determined Using The Greulich and Pyle StandardsDocument7 pagesEffect of Knowledge of Chronologic Age On The Variability of Pediatric Bone Age Determined Using The Greulich and Pyle StandardsParishan SaeedNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument43 pagesSee Full Prescribing Information For Complete Boxed WarningParishan SaeedNo ratings yet
- Guidance Statement: Hormone Supplementation For Pubertal Induction in GirlsDocument21 pagesGuidance Statement: Hormone Supplementation For Pubertal Induction in GirlsParishan SaeedNo ratings yet
- Ece Home 2023 Paag DDocument1 pageEce Home 2023 Paag DParishan SaeedNo ratings yet
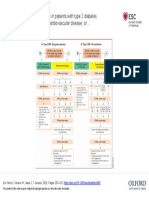
- Guideline Treatment of T2DM 2020 ESCDocument1 pageGuideline Treatment of T2DM 2020 ESCParishan SaeedNo ratings yet
- Glp-1 Receptor Agonists (GLP-1 RA) : Presented By: Nermeen S. Esa (Clinical Pharmacist)Document10 pagesGlp-1 Receptor Agonists (GLP-1 RA) : Presented By: Nermeen S. Esa (Clinical Pharmacist)Parishan SaeedNo ratings yet
- COVID-19 Disease SeverityDocument7 pagesCOVID-19 Disease SeverityParishan SaeedNo ratings yet
- Discussion #3: The Concept of Culture Learning ObjectivesDocument4 pagesDiscussion #3: The Concept of Culture Learning ObjectivesJohn Lery SurellNo ratings yet
- Storage Emulated 0 Android Data Com - Cv.docscanner Cache How-China-Engages-South-Asia-Themes-Partners-and-ToolsDocument140 pagesStorage Emulated 0 Android Data Com - Cv.docscanner Cache How-China-Engages-South-Asia-Themes-Partners-and-Toolsrahul kumarNo ratings yet
- PSYC1111 Ogden Psychology of Health and IllnessDocument108 pagesPSYC1111 Ogden Psychology of Health and IllnessAleNo ratings yet
- CSEC Eng A Summary ExerciseDocument1 pageCSEC Eng A Summary ExerciseArisha NicholsNo ratings yet
- ImpetigoDocument16 pagesImpetigokikimasyhurNo ratings yet
- Site Master S113C, S114C, S331C, S332C, Antenna, Cable and Spectrum AnalyzerDocument95 pagesSite Master S113C, S114C, S331C, S332C, Antenna, Cable and Spectrum AnalyzerKodhamagulla SudheerNo ratings yet
- Directions: Choose The Best Answer For Each Multiple Choice Question. Write The Best Answer On The BlankDocument2 pagesDirections: Choose The Best Answer For Each Multiple Choice Question. Write The Best Answer On The BlankRanulfo MayolNo ratings yet
- Capacitor Banks in Power System Part FourDocument4 pagesCapacitor Banks in Power System Part FourTigrillo100% (1)
- Pagan and Wiccan Quotes and GuidanceDocument8 pagesPagan and Wiccan Quotes and GuidanceStinkyBooNo ratings yet
- Operations Management (Scheduling) PDFDocument4 pagesOperations Management (Scheduling) PDFVijay Singh ThakurNo ratings yet
- 2501 Mathematics Paper+with+solution EveningDocument10 pages2501 Mathematics Paper+with+solution EveningNenavath GaneshNo ratings yet
- Update UI Components With NavigationUIDocument21 pagesUpdate UI Components With NavigationUISanjay PatelNo ratings yet
- Seismic Response of Elevated Liquid Storage Steel Tanks Isolated by VCFPS at Top of Tower Under Near-Fault Ground MotionsDocument6 pagesSeismic Response of Elevated Liquid Storage Steel Tanks Isolated by VCFPS at Top of Tower Under Near-Fault Ground MotionsciscoNo ratings yet
- SBE13 CH 18Document74 pagesSBE13 CH 18Shad ThiệnNo ratings yet
- PETE 689 Underbalanced Drilling (UBD) : Well Engineering Read: UDM Chapter 5 Pages 5.1-5.41Document74 pagesPETE 689 Underbalanced Drilling (UBD) : Well Engineering Read: UDM Chapter 5 Pages 5.1-5.41Heris SitompulNo ratings yet
- S - BlockDocument21 pagesS - BlockRakshit Gupta100% (2)
- Nespresso Case StudyDocument7 pagesNespresso Case StudyDat NguyenNo ratings yet
- Faith-Based Organisational Development (OD) With Churches in MalawiDocument10 pagesFaith-Based Organisational Development (OD) With Churches in MalawiTransbugoyNo ratings yet
- ReadingDocument2 pagesReadingNhư ÝNo ratings yet
- Echnical Ocational Ivelihood: Edia and Nformation IteracyDocument12 pagesEchnical Ocational Ivelihood: Edia and Nformation IteracyKrystelle Marie AnteroNo ratings yet
- CN and OS Lab ManualDocument53 pagesCN and OS Lab Manualsudheer mangalampalliNo ratings yet
- Cambridge English Key Sample Paper 1 Reading and Writing v2Document9 pagesCambridge English Key Sample Paper 1 Reading and Writing v2kalinguer100% (1)
- Marcelo H Del PilarDocument8 pagesMarcelo H Del PilarLee Antonino AtienzaNo ratings yet
- HIS Unit COMBINES Two Birthdays:: George Washington's BirthdayDocument9 pagesHIS Unit COMBINES Two Birthdays:: George Washington's BirthdayOscar Panez LizargaNo ratings yet
- Modern DrmaDocument7 pagesModern DrmaSHOAIBNo ratings yet
- Mathematics Grade 5 Quarter 2: Answer KeyDocument4 pagesMathematics Grade 5 Quarter 2: Answer KeyApril Jean Cahoy100% (2)