You might also like
- Clinical Case Study on HypothyroidismDocument36 pagesClinical Case Study on HypothyroidismLeslie Rufino100% (1)
- Comprehensive Hematology and Biochemistry Report for Mr. Srinivas VDocument28 pagesComprehensive Hematology and Biochemistry Report for Mr. Srinivas VVijaya SheelamNo ratings yet
- 0a27thyroid Function TestDocument35 pages0a27thyroid Function TestAshokvardhan Chowdary Nandigam67% (3)
- 4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFDocument89 pages4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFjackie funtanilla100% (1)
- Application of Radioimmunoassay in Chemical PathologyDocument8 pagesApplication of Radioimmunoassay in Chemical PathologyKerpersky LogNo ratings yet
- ImmunoAssay ProtocolDocument31 pagesImmunoAssay ProtocolSanta Kumar75% (4)
- Microbiome impact on sex, thyroid, growth and parathyroid hormonesDocument13 pagesMicrobiome impact on sex, thyroid, growth and parathyroid hormonesBrenda FolkNo ratings yet
- Journal Club Presentation: Presented by Sunitha Elza Mathew Ra1422281010014 Pharmd InternDocument18 pagesJournal Club Presentation: Presented by Sunitha Elza Mathew Ra1422281010014 Pharmd InternManali DNo ratings yet
- Thyroid Disorders: Medical Surgical NursingDocument20 pagesThyroid Disorders: Medical Surgical Nursingthanuja mathewNo ratings yet
- Clinical ChemistryDocument19 pagesClinical Chemistrythrowawy100% (2)
- Case Study About HyperthyroidismDocument11 pagesCase Study About HyperthyroidismRheciel Abarquez Briones RN100% (4)
- Previous Exam by System FullDocument26 pagesPrevious Exam by System FullMostafa Mahmoud ElsebeyNo ratings yet
- Spesifikasi Barang Medis Habis Pakai Reagen Laboratorium TA. 2021Document3 pagesSpesifikasi Barang Medis Habis Pakai Reagen Laboratorium TA. 2021Mandalika Putri PratamaNo ratings yet
- Principles of Early Drug DiscoveryDocument11 pagesPrinciples of Early Drug DiscoveryAmrit Karmarkar RPhNo ratings yet
- Analitical ErrorDocument15 pagesAnalitical Errorlabor baiturrahimNo ratings yet
- Bittner 2016 AlzDemDocument10 pagesBittner 2016 AlzDemnour abdallaNo ratings yet
- Nutraceutical antioxidants in neuroprotection and anti-cancer therapyDocument85 pagesNutraceutical antioxidants in neuroprotection and anti-cancer therapyHajrah SuhardiNo ratings yet
- Systematic Review and Meta-Analysis of The Efficacy and Safety of Immunosuppressive Pulse Therapy in The Treatment of Paraquat PoisoningDocument10 pagesSystematic Review and Meta-Analysis of The Efficacy and Safety of Immunosuppressive Pulse Therapy in The Treatment of Paraquat PoisoningRICHARNo ratings yet
- Gold-Nanobeacons For Gene Therapy: Evaluation of Genotoxicity, Cell Toxicity and Proteome Profiling AnalysisDocument63 pagesGold-Nanobeacons For Gene Therapy: Evaluation of Genotoxicity, Cell Toxicity and Proteome Profiling AnalysisGargi MishraNo ratings yet
- The Endocrine Laboratory: Key PointsDocument3 pagesThe Endocrine Laboratory: Key PointsMauricio Lopez AlvarezNo ratings yet
- Role of Serum Procalcitonin in Early Diagnosis of Neonatal SepsisDocument5 pagesRole of Serum Procalcitonin in Early Diagnosis of Neonatal SepsisIqbalNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument19 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Effectiveness of Antithymocyte Globulin InductionDocument5 pagesEffectiveness of Antithymocyte Globulin Inductioncaydin33No ratings yet
- 1 s2.0 S0969805119301076 MainDocument7 pages1 s2.0 S0969805119301076 Mainarifudin_achmadNo ratings yet
- Reviewing Immunoassay Interferences: Detecting and Resolving Erroneous ResultsDocument5 pagesReviewing Immunoassay Interferences: Detecting and Resolving Erroneous ResultsKartika ParamitaNo ratings yet
- KBM0701 Stern 21Document6 pagesKBM0701 Stern 21Agus WijataNo ratings yet
- Journal of Clinical Medicine-7 April 2023 PublicationDocument21 pagesJournal of Clinical Medicine-7 April 2023 PublicationNARESHNo ratings yet
- Early Pregnancy Biomarkers in Pre-Eclampsia: A Systematic Review and Meta-AnalysisDocument22 pagesEarly Pregnancy Biomarkers in Pre-Eclampsia: A Systematic Review and Meta-AnalysismochkurniawanNo ratings yet
- Wang 2018Document27 pagesWang 2018Raissa RezendeNo ratings yet
- Bonassi 2002Document14 pagesBonassi 2002Melissa SouzaNo ratings yet
- Basic Study Design Influences The Results of Orthodontiinvestigations PDFDocument11 pagesBasic Study Design Influences The Results of Orthodontiinvestigations PDFemadNo ratings yet
- Exposure Profiling of Reactive Compounds in Complex Mixtures 2013 ToxicologyDocument6 pagesExposure Profiling of Reactive Compounds in Complex Mixtures 2013 ToxicologyMarcelosarlingNo ratings yet
- Interferences With Thyroid Function ImmunoassaysDocument21 pagesInterferences With Thyroid Function Immunoassayssabir osmanNo ratings yet
- 1945892419851312Document10 pages1945892419851312kasandraharahapNo ratings yet
- 4 KNDocument25 pages4 KNMohammad Yusuf AlamudiNo ratings yet
- A Critical Review and Meta Analysis of Epidemiolo - 2021 - Mutation Research GenDocument20 pagesA Critical Review and Meta Analysis of Epidemiolo - 2021 - Mutation Research GenAURORA RENJANI KIRANANo ratings yet
- Multi-Targeted Therapy Resistance Via Drug - Induced Secretome FucosylationDocument42 pagesMulti-Targeted Therapy Resistance Via Drug - Induced Secretome Fucosylationaditya subchanNo ratings yet
- J Ajo 2020 03 018Document24 pagesJ Ajo 2020 03 018koas forensikNo ratings yet
- 4bpharm FindDocument20 pages4bpharm FindA.R.N.U TECH CHANNELNo ratings yet
- Effectiveness of Antimicrobial Photodynamic Therapy in The Periodontis Systematic ReviewDocument42 pagesEffectiveness of Antimicrobial Photodynamic Therapy in The Periodontis Systematic ReviewreizkayNo ratings yet
- HHS Public Access: Multiplex Immunosensor Arrays For Electrochemical Detection of Cancer Biomarker ProteinsDocument31 pagesHHS Public Access: Multiplex Immunosensor Arrays For Electrochemical Detection of Cancer Biomarker ProteinswardaninurindahNo ratings yet
- Efficacy of Rupatadine for Korean Perennial Allergic RhinitisDocument9 pagesEfficacy of Rupatadine for Korean Perennial Allergic RhinitisAnisa RahmaNo ratings yet
- UNICEF Annual ReportDocument15 pagesUNICEF Annual ReportraissametasariNo ratings yet
- Model AbstractsDocument2 pagesModel AbstractsAnonymousNo ratings yet
- 7. Rating the Quality of Evidence—InconsistencyDocument9 pages7. Rating the Quality of Evidence—InconsistencyGeorgina CNo ratings yet
- Interferences With Thyroid Function Immunoassays: Clinical Implications and Detection AlgorithmDocument21 pagesInterferences With Thyroid Function Immunoassays: Clinical Implications and Detection AlgorithmDewi Paramita YuniarahmiNo ratings yet
- Advanced techniques livestock disease diagnosisDocument8 pagesAdvanced techniques livestock disease diagnosisSaghirAurakxaiNo ratings yet
- Use of Anti-Cyclic CitrullinatDocument6 pagesUse of Anti-Cyclic CitrullinatyooyoNo ratings yet
- Molecular Diagnostics for Cancer DetectionDocument6 pagesMolecular Diagnostics for Cancer DetectionMobashir RahmanNo ratings yet
- PKPD For BeginnersDocument8 pagesPKPD For Beginnerstanty_ukNo ratings yet
- Diagnostic and Prognostic Biomarkers of Sepsis in Critical CareDocument8 pagesDiagnostic and Prognostic Biomarkers of Sepsis in Critical Caremr_curiousityNo ratings yet
- Development and Validation of A Penicillin Allergy Clinical Decision RuleDocument8 pagesDevelopment and Validation of A Penicillin Allergy Clinical Decision RuleRodrigo Ehécatl Torres NevárezNo ratings yet
- Na 2016Document5 pagesNa 2016abdullahkhilji.nitsNo ratings yet
- (Q1) Pone.0169593Document16 pages(Q1) Pone.0169593wiradewi lestariNo ratings yet
- Nephrotic Syndrome: What's New, What's Hot?: Review ArticleDocument8 pagesNephrotic Syndrome: What's New, What's Hot?: Review ArticleIfah Inayah D'zatrichaNo ratings yet
- Bio-PDFDocument41 pagesBio-PDFSNo ratings yet
- ELISA in The Multiplex Era Potential and PitfallsDocument17 pagesELISA in The Multiplex Era Potential and PitfallsHameed SabahNo ratings yet
- Molecular and Biomarker-Based Diagnostics in Early Sepsis - Current Challenges and Future Perspectives PDFDocument40 pagesMolecular and Biomarker-Based Diagnostics in Early Sepsis - Current Challenges and Future Perspectives PDFBram AjaNo ratings yet
- Advancing Toxicity Testing Methods For The 21 CenturyDocument49 pagesAdvancing Toxicity Testing Methods For The 21 CenturynataleebellaNo ratings yet
- Methods: A.M. Lavorato-Rocha, L.G. Anjos, I.W. Cunha, J. Vassallo, F.A. Soares, R.M. RochaDocument5 pagesMethods: A.M. Lavorato-Rocha, L.G. Anjos, I.W. Cunha, J. Vassallo, F.A. Soares, R.M. RochaMuhammadRidwansyahNo ratings yet
- Rood 2017Document19 pagesRood 2017Estefany HurtadoNo ratings yet
- PKPD For BeginnersDocument31 pagesPKPD For Beginnerstanty_ukNo ratings yet
- Ricafort - Finals Journal Critiquing IS LectureDocument2 pagesRicafort - Finals Journal Critiquing IS Lecturesean ricafortNo ratings yet
- Proca 3Document10 pagesProca 3alejandro1122No ratings yet
- Physiology PharmacologyDocument126 pagesPhysiology PharmacologyuneedlesNo ratings yet
- ReviewDocument35 pagesReviewJaganath RaviNo ratings yet
- Review Bias in Clinical Intervention ResearchDocument9 pagesReview Bias in Clinical Intervention ResearchHesed VirtoNo ratings yet
- !! 2020 Drug Hypersensitivity ReactionsDocument12 pages!! 2020 Drug Hypersensitivity ReactionsdregleavNo ratings yet
- ESPR Statement on Bone Age DeterminationDocument4 pagesESPR Statement on Bone Age DeterminationParishan SaeedNo ratings yet
- JML 2022 0170 1Document8 pagesJML 2022 0170 1Parishan SaeedNo ratings yet
- ClinPediatrEndocrinol200716123 9PHPIahandDocument8 pagesClinPediatrEndocrinol200716123 9PHPIahandParishan SaeedNo ratings yet
- Chapter 356.8 - IgA Vasculitis (Henoch-Schonlein)Document2 pagesChapter 356.8 - IgA Vasculitis (Henoch-Schonlein)Parishan SaeedNo ratings yet
- 976c5091-5277-4d13-8655-371a2eb3d13fDocument2 pages976c5091-5277-4d13-8655-371a2eb3d13fParishan SaeedNo ratings yet
- Quick Reference Guide Endocrine Hypertension 2 2016 VersionDocument16 pagesQuick Reference Guide Endocrine Hypertension 2 2016 VersionParishan SaeedNo ratings yet
- Cortisol II 2020-03 v6Document5 pagesCortisol II 2020-03 v6Parishan SaeedNo ratings yet
- Effect of Knowledge of Chronologic Age On The Variability of Pediatric Bone Age Determined Using The Greulich and Pyle StandardsDocument7 pagesEffect of Knowledge of Chronologic Age On The Variability of Pediatric Bone Age Determined Using The Greulich and Pyle StandardsParishan SaeedNo ratings yet
- Decreased Ligand Affinity Rather Than Glucocorticoid Receptor Down-Regulation in Patients With Endogenous Cushing's SyndromeDocument5 pagesDecreased Ligand Affinity Rather Than Glucocorticoid Receptor Down-Regulation in Patients With Endogenous Cushing's SyndromeParishan SaeedNo ratings yet
- Ece Home 2023 Paag DDocument1 pageEce Home 2023 Paag DParishan SaeedNo ratings yet
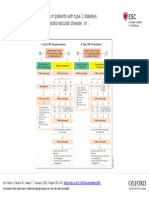
- Guideline Treatment of T2DM 2020 ESCDocument1 pageGuideline Treatment of T2DM 2020 ESCParishan SaeedNo ratings yet
- Guidance Statement: Hormone Supplementation For Pubertal Induction in GirlsDocument21 pagesGuidance Statement: Hormone Supplementation For Pubertal Induction in GirlsParishan SaeedNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument43 pagesSee Full Prescribing Information For Complete Boxed WarningParishan SaeedNo ratings yet
- COVID-19 Anticoagulation - UpToDateDocument1 pageCOVID-19 Anticoagulation - UpToDateParishan SaeedNo ratings yet
- Glp-1 Receptor Agonists (GLP-1 RA) : Presented By: Nermeen S. Esa (Clinical Pharmacist)Document10 pagesGlp-1 Receptor Agonists (GLP-1 RA) : Presented By: Nermeen S. Esa (Clinical Pharmacist)Parishan SaeedNo ratings yet
- COVID-19 Disease SeverityDocument7 pagesCOVID-19 Disease SeverityParishan SaeedNo ratings yet
- Congenital HypothyroidismDocument37 pagesCongenital HypothyroidismAwaluddin SalamNo ratings yet
- Case Ana - CC - Primary HyperthyroidismDocument15 pagesCase Ana - CC - Primary HyperthyroidismKatrina CanlapanNo ratings yet
- Medibuddy PHLB388673014Document15 pagesMedibuddy PHLB388673014Tejasvi VineshNo ratings yet
- M4vmvns3ua5zc1zzyn0sigr2Document2 pagesM4vmvns3ua5zc1zzyn0sigr2Sagar VashisthNo ratings yet
- 2 - Thyroxine and Treatment of Hypothyroidism - 2019Document8 pages2 - Thyroxine and Treatment of Hypothyroidism - 2019Johanna Bustos NutricionistaNo ratings yet
- KI 70 Therapeutic Potential in Graves Ca ThyroidDocument4 pagesKI 70 Therapeutic Potential in Graves Ca ThyroidGaurav MalhotraNo ratings yet
- Laboratorio Clinico Toledo: Patient Number Birthdate SexDocument1 pageLaboratorio Clinico Toledo: Patient Number Birthdate SexMirle BonetNo ratings yet
- Haematology Complete Blood Count (CBC EXT) : 021808250310 MR - AJAY KUMAR 662326Document7 pagesHaematology Complete Blood Count (CBC EXT) : 021808250310 MR - AJAY KUMAR 662326ANSHU KUMAR RANANo ratings yet
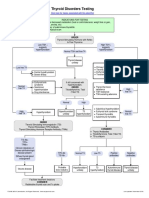
- Thyroid Testing AlgorithmDocument1 pageThyroid Testing AlgorithmRezi HelperNo ratings yet
- Revalence of Thyroid Disorders in A Tertiary Care CenterDocument5 pagesRevalence of Thyroid Disorders in A Tertiary Care CenterAvisa Cetta CresmaNo ratings yet
- Jardine Jade Albert C. Valdez, RMTDocument48 pagesJardine Jade Albert C. Valdez, RMTEj BersalonaNo ratings yet
- Congenital Hypothyroidism: Screening, Diagnosis, Management, and OutcomeDocument7 pagesCongenital Hypothyroidism: Screening, Diagnosis, Management, and OutcomeIbrahim Abdul KareemNo ratings yet
- Overview of Thyroiditis - UpToDateDocument7 pagesOverview of Thyroiditis - UpToDateCamila NogueiraNo ratings yet
- Biochem Experiment 5Document6 pagesBiochem Experiment 5Julius Memeg PanayoNo ratings yet
- 2003, Vol.32, Issues 2, Consultative EndocrinologyDocument210 pages2003, Vol.32, Issues 2, Consultative Endocrinologyomar ramirezNo ratings yet
- Hormonal Regulation of ExerciseDocument11 pagesHormonal Regulation of ExerciseMozil Fadzil KamarudinNo ratings yet
- Chapter 12 Coordination and Response GuideDocument18 pagesChapter 12 Coordination and Response GuideyokekeannNo ratings yet
- Endocrine GlandsDocument36 pagesEndocrine GlandsnasyitahnorzlanNo ratings yet
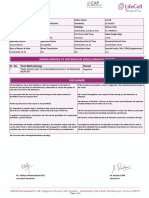
- Inborn Errors of Metabolism (Iem) Summary Report: Sr. No. Test Methodology Result Test TypeDocument2 pagesInborn Errors of Metabolism (Iem) Summary Report: Sr. No. Test Methodology Result Test TypeMallikharjunaRao medaNo ratings yet
- Neonatal Screening For Congenital Hypothyroidism - Toni TorresaniDocument6 pagesNeonatal Screening For Congenital Hypothyroidism - Toni TorresaniDIMAMIANo ratings yet
- Daw Khin Nwe Win Sharing Health EdcuationDocument180 pagesDaw Khin Nwe Win Sharing Health EdcuationAungNo ratings yet