You might also like
- Functional Human Physiology: For The Exercise and Sport Sciences The Cardiovascular System: Cardiac FunctionDocument186 pagesFunctional Human Physiology: For The Exercise and Sport Sciences The Cardiovascular System: Cardiac FunctionBery Agana F. PurbaNo ratings yet
- Cardiovascular SystemDocument14 pagesCardiovascular SystemAthena Huynh100% (1)
- Regulation of Heart Rate, Stroke Volume, Cardiac Output, Blood FlowDocument20 pagesRegulation of Heart Rate, Stroke Volume, Cardiac Output, Blood FlowShveta MahajanNo ratings yet
- Regional AnesthesiaDocument369 pagesRegional Anesthesiasyifa100% (4)
- Bruce, E.N.-biomedical Signal Processing&Signal ModelingDocument534 pagesBruce, E.N.-biomedical Signal Processing&Signal ModelingReza Rad75% (4)
- Cadiac Cycle, Heart Sound, ECG, HypertensionDocument110 pagesCadiac Cycle, Heart Sound, ECG, HypertensionNilesh100% (1)
- Unit 1 Gastro Intestinal SystemDocument53 pagesUnit 1 Gastro Intestinal SystemPlatypus proNo ratings yet
- The Cardiac CycleDocument9 pagesThe Cardiac CycleKaylababy Hamilton BlackNo ratings yet
- Heart Anatomy: LocationDocument45 pagesHeart Anatomy: LocationZaira100% (1)
- Cardiovascular System: K. Hariharan Iv Eee - 'B'Document33 pagesCardiovascular System: K. Hariharan Iv Eee - 'B'Hari Haran100% (1)
- Heart Muscle: The Heart As A Pump and FunctionDocument4 pagesHeart Muscle: The Heart As A Pump and Functionmcwnotes100% (1)
- Cardiovascular and Syrculation System, 2013Document92 pagesCardiovascular and Syrculation System, 2013Santi Purnama SariNo ratings yet
- Heart MuscleDocument10 pagesHeart Muscle22194No ratings yet
- Cardiovascular SystemDocument34 pagesCardiovascular Systemurooj100% (1)
- CHP 2 The Biological PerspectiveDocument65 pagesCHP 2 The Biological PerspectiveAthaliah Kei'seeNo ratings yet
- Cardiovascular System: Presented by DR Aparna Ramachandran Mds 1 Dept of Public Health DentistryDocument73 pagesCardiovascular System: Presented by DR Aparna Ramachandran Mds 1 Dept of Public Health DentistryAparna RamachandranNo ratings yet
- Lecture - 3 Properties of Cardiac MuscleDocument35 pagesLecture - 3 Properties of Cardiac MuscleMRM7MDNo ratings yet
- Conduction of HeartDocument21 pagesConduction of Heartangelsundar22100% (1)
- Notes On Coordination - Response - Nervous System, Reflex Arc, Type of NeuronesDocument6 pagesNotes On Coordination - Response - Nervous System, Reflex Arc, Type of NeuronesamberNo ratings yet
- PHD Thesis NeuroscienceDocument42 pagesPHD Thesis NeuroscienceAnil Bheemaiah100% (1)
- Activity 1: The Muscle Twitch and The Latent PeriodDocument10 pagesActivity 1: The Muscle Twitch and The Latent PeriodAndiena ElsafiraNo ratings yet
- Cardiac L2Document18 pagesCardiac L2Qutaybah JahmanyNo ratings yet
- Lecture 2: The Heart: Prof. Magidah Alaudi, M.SCDocument62 pagesLecture 2: The Heart: Prof. Magidah Alaudi, M.SCMonicaNo ratings yet
- الجهاز الدوريDocument16 pagesالجهاز الدوريHUAWEI HUAWEINo ratings yet
- 2015A&PIntro CardiovascularHandoutDocument16 pages2015A&PIntro CardiovascularHandoutMaggieHameedNo ratings yet
- Components of The Cardiovascular SystemDocument23 pagesComponents of The Cardiovascular SystemMr. DummyNo ratings yet
- 11 Ant HEART MUSCLEDocument57 pages11 Ant HEART MUSCLEZuhaib AhmedNo ratings yet
- Cardiovascular Physiology 1Document44 pagesCardiovascular Physiology 1maxmus4No ratings yet
- HeartDocument50 pagesHeartmmm479cb4kNo ratings yet
- Circulatory SystemDocument155 pagesCirculatory SystemTrisha Mae BolotaoloNo ratings yet
- CVS - IiDocument12 pagesCVS - IiBinta Elsa JohnNo ratings yet
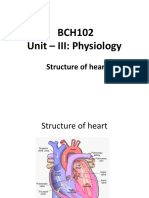
- BCH102 Unit - III: Physiology: Structure of HeartDocument17 pagesBCH102 Unit - III: Physiology: Structure of Heartdivya vajpayeeNo ratings yet
- Hemodinamik Pada Sistem Kardiovaskuler - PPTDocument114 pagesHemodinamik Pada Sistem Kardiovaskuler - PPTIsna ZalwaNo ratings yet
- Coordinated Cycles of Heart Contraction Drive Double Circulate in MammalsDocument5 pagesCoordinated Cycles of Heart Contraction Drive Double Circulate in MammalsMayar HasanNo ratings yet
- Cardiac AssessmentDocument54 pagesCardiac AssessmentAthira PSNo ratings yet
- Life's Progression Through Cardiac PhysiologyDocument91 pagesLife's Progression Through Cardiac PhysiologyprofcarleyNo ratings yet
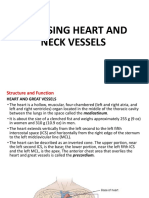
- H.A. Assessing Heart and Neck VesselsDocument55 pagesH.A. Assessing Heart and Neck VesselsMc Ramil B. PraderoNo ratings yet
- Cardiovascular SystemDocument12 pagesCardiovascular SystemDevendra RawatNo ratings yet
- Structure and Function of The HeartaaslDocument5 pagesStructure and Function of The HeartaaslidlydumpfvckNo ratings yet
- Electrical Conduction System of The HeartDocument27 pagesElectrical Conduction System of The HeartAnonymous gUjimJKNo ratings yet
- Jantung PDFDocument1 pageJantung PDFKarensa JanetNo ratings yet
- Cardiac CycleDocument6 pagesCardiac CycleShahina ShayneNo ratings yet
- HeartDocument36 pagesHeartSoovendran VaradarajanNo ratings yet
- 81: Mammalian Heart and Its RegulationDocument75 pages81: Mammalian Heart and Its RegulationIt's Ika100% (1)
- CardioDocument30 pagesCardioPamela LusungNo ratings yet
- Capillary: Nutrients To, and Take Wastes Away From, CellsDocument7 pagesCapillary: Nutrients To, and Take Wastes Away From, CellseyhethNo ratings yet
- Cardio PulmonaryDocument4 pagesCardio PulmonaryAyessa CortesNo ratings yet
- Cardiovascular SystemDocument7 pagesCardiovascular SystemJoão EusébioNo ratings yet
- HSCI 103 LAB 2 ECG & Heart Sounds Worksheet - SP 2021Document10 pagesHSCI 103 LAB 2 ECG & Heart Sounds Worksheet - SP 2021MatthewFlecknoeNo ratings yet
- Chapter 6cardiovascular Physiology PDFDocument17 pagesChapter 6cardiovascular Physiology PDFtahira UroojNo ratings yet
- Lecture No 8Document14 pagesLecture No 8Areesha MushtaqNo ratings yet
- Module 3 The Circulatory SystemDocument11 pagesModule 3 The Circulatory SystemAndriya JoshyNo ratings yet
- Cardiovascular SystemDocument13 pagesCardiovascular SystemRania AshrafNo ratings yet
- @PPT - Fisiologi Jantung - KD 2012Document70 pages@PPT - Fisiologi Jantung - KD 2012irmayanti adewarjaNo ratings yet
- The Heart PDFDocument13 pagesThe Heart PDFMary Ann SacramentoNo ratings yet
- Chapter 20 A&P 2Document7 pagesChapter 20 A&P 2Jilian McGuganNo ratings yet
- CVS 2Document153 pagesCVS 2khalidtalal8000No ratings yet
- Cardiac CycleDocument3 pagesCardiac CycleKhadijah HabeebahNo ratings yet
- Animal Physiolgy. Lec4Document22 pagesAnimal Physiolgy. Lec4ao868598No ratings yet
- 2-Cardiac Electical ActivityDocument26 pages2-Cardiac Electical ActivityhalayehiahNo ratings yet
- Physiology of CardiovascularDocument74 pagesPhysiology of CardiovascularStevan SalosaNo ratings yet
- Circulation WorksheetDocument3 pagesCirculation Worksheetholagato100% (1)
- Session 5Document41 pagesSession 5tazebNo ratings yet
- First Question: Student's Name: Adel Sulaiman SectionDocument5 pagesFirst Question: Student's Name: Adel Sulaiman SectionDental LecturesMMQNo ratings yet
- CV Physio-IntroductionDocument33 pagesCV Physio-IntroductionHanaNo ratings yet
- Compare and Contrast Process in Plants and Animals: Chemical and Nervous Control 1Document7 pagesCompare and Contrast Process in Plants and Animals: Chemical and Nervous Control 1lostgirlNo ratings yet
- Product Assessment Report - K-Othrine SC 25 Family PublicDocument142 pagesProduct Assessment Report - K-Othrine SC 25 Family PublicwibowoNo ratings yet
- Bio612 Writtenreport Cabaluna NancyDocument10 pagesBio612 Writtenreport Cabaluna NancyNancy Medina CabalunaNo ratings yet
- National NORCET Test-8Document108 pagesNational NORCET Test-8SHIVANIINo ratings yet
- Chapter 7 Student Version The Nervous System 2020 (1138)Document21 pagesChapter 7 Student Version The Nervous System 2020 (1138)S. MartinezNo ratings yet
- Purves 1981 - Microelectrode Methods For Intracellular Recording and IonophoresisDocument156 pagesPurves 1981 - Microelectrode Methods For Intracellular Recording and Ionophoresisdfddddsdf2100% (1)
- Neurophysiology in Oral and Maxillofacial SurgeryDocument35 pagesNeurophysiology in Oral and Maxillofacial SurgeryPriya ManimalaNo ratings yet
- Science Chapter 2 Form 4Document16 pagesScience Chapter 2 Form 4Muhammad Akmal Kamaluddin75% (4)
- Ringer's Solution Stimulates The Blood Plasma of Frogs and Moistens The Exposed Muscle. Isotonic To Amphibians - Hypertonic To HumansDocument2 pagesRinger's Solution Stimulates The Blood Plasma of Frogs and Moistens The Exposed Muscle. Isotonic To Amphibians - Hypertonic To Humansmaypeee100% (1)
- Aimst University Physiology Unit: Dr.P.SunithaDocument50 pagesAimst University Physiology Unit: Dr.P.SunithaYaashinii PeriathambyNo ratings yet
- Sec2 Lec2 ActionPotentials 2022 v2Document31 pagesSec2 Lec2 ActionPotentials 2022 v2GentianaNo ratings yet
- Biology Past Paper Common Questions by Vasumitra Gajbhiye PDFDocument75 pagesBiology Past Paper Common Questions by Vasumitra Gajbhiye PDFDDR Gaming100% (1)
- Henytoin Anticonvulsant Seizures: Phenytoin (Document4 pagesHenytoin Anticonvulsant Seizures: Phenytoin (Ashir SaroyaNo ratings yet
- Biolistrik: DR - Susy OliviaDocument97 pagesBiolistrik: DR - Susy OliviaHartomas BumiharjoNo ratings yet
- Insect MechanoreceptorsDocument6 pagesInsect Mechanoreceptorsjohn cenaNo ratings yet
- ZoologyDocument24 pagesZoologyS V S VardhanNo ratings yet
- Loza Huerta2021 Article Thallium SensitiveFluorescentADocument10 pagesLoza Huerta2021 Article Thallium SensitiveFluorescentAVivien JusztusNo ratings yet
- My Cheat SheetDocument3 pagesMy Cheat SheetTenzin KyizomNo ratings yet
- AP Biology Midterm ReviewDocument3 pagesAP Biology Midterm ReviewAndy LiNo ratings yet
- Chapter 12Document24 pagesChapter 12MaskManNo ratings yet
- CH 48Document11 pagesCH 48randomtamaNo ratings yet
- Greater Electromyographic Responses Do Not Imply.31 PDFDocument4 pagesGreater Electromyographic Responses Do Not Imply.31 PDFAgustin LopezNo ratings yet