You might also like
- Am Medicine - Com 210815 m77Document596 pagesAm Medicine - Com 210815 m77Cai Velasco Decena100% (16)
- Medical History QuestionnaireDocument1 pageMedical History QuestionnaireHare MasterYodaNo ratings yet
- Physician's Report Form: Part A (Completed by The Applicant) 1. 2. 3Document4 pagesPhysician's Report Form: Part A (Completed by The Applicant) 1. 2. 3Arturo MBNo ratings yet
- Child Adol Traditional Biopsychosocial TemplateDocument11 pagesChild Adol Traditional Biopsychosocial Templateyeney armenteros100% (1)
- Stress ManagementDocument54 pagesStress ManagementDen Pamplona100% (4)
- OSCE Pediatrics Observed Stations - Dr.D.Y.patil CME Aug 2012Document54 pagesOSCE Pediatrics Observed Stations - Dr.D.Y.patil CME Aug 2012Gideon K. MutaiNo ratings yet
- Global Health InitiativesDocument18 pagesGlobal Health InitiativesJohn Elmer Salazar NiervesNo ratings yet
- Impaired Gas Exchange - NCPDocument4 pagesImpaired Gas Exchange - NCPJaye DangoNo ratings yet
- Improving Hospital Performance and Productivity With The Balanced Scorecard - 2Document22 pagesImproving Hospital Performance and Productivity With The Balanced Scorecard - 2Yunita Soraya HusinNo ratings yet
- Paediatric NP FormDocument2 pagesPaediatric NP FormBOWEN TLCNo ratings yet
- PE - Draft Parq FormDocument2 pagesPE - Draft Parq FormYenny TigaNo ratings yet
- Medical AuthorizationDocument2 pagesMedical AuthorizationAmanda HernandezNo ratings yet
- Medical Form 4-12 YearsDocument1 pageMedical Form 4-12 YearsJackson SilvaNo ratings yet
- Authorization To Consent To Treatment of A Minor 2012Document2 pagesAuthorization To Consent To Treatment of A Minor 2012Nakuru SandwichNo ratings yet
- Medical History Form 3 Years and OlderDocument3 pagesMedical History Form 3 Years and OlderJalisha SarmientoNo ratings yet
- Medical Application Form: Name Relation (E/S/C) D. O. B SEX (M/F) Marital Status Height (CM) Weight (KG) Emirates (VISA)Document3 pagesMedical Application Form: Name Relation (E/S/C) D. O. B SEX (M/F) Marital Status Height (CM) Weight (KG) Emirates (VISA)cmthebossNo ratings yet
- Physical Form 2018Document2 pagesPhysical Form 2018api-247134277No ratings yet
- Updated Health FormsDocument3 pagesUpdated Health Formskevin9392No ratings yet
- International Travel Medical QuestionnaireDocument4 pagesInternational Travel Medical QuestionnairecristinaNo ratings yet
- 23FB12 Permission SlipDocument2 pages23FB12 Permission SlipEmma StevensNo ratings yet
- 302 RUA - Interview WorksheetDocument4 pages302 RUA - Interview WorksheetChristy RobinettNo ratings yet
- Screenshot 2022-06-28 at 9.33.56 AM PDFDocument1 pageScreenshot 2022-06-28 at 9.33.56 AM PDFhelen S. DeeNo ratings yet
- Health Questionnaire: Name (Please Print)Document1 pageHealth Questionnaire: Name (Please Print)CarlosSchlozJuniorNo ratings yet
- Sports Physical Examination: Date of Last Known Tetanus (Lockjaw) Shot: Date of Last Complete Physical ExaminationDocument2 pagesSports Physical Examination: Date of Last Known Tetanus (Lockjaw) Shot: Date of Last Complete Physical ExaminationBrandon Reyes CortezNo ratings yet
- Child's Details: Date of Birth: Nric/Bc/Fin: NameDocument2 pagesChild's Details: Date of Birth: Nric/Bc/Fin: NameAndy LimNo ratings yet
- Medical StatementDocument1 pageMedical StatementDaye CampanillaNo ratings yet
- Medical Details 2023Document2 pagesMedical Details 2023Lord PrydzNo ratings yet
- Epilepsy Report SampleDocument5 pagesEpilepsy Report SampleKavanNo ratings yet
- Health Assessment Record: State of Connecticut Department of EducationDocument3 pagesHealth Assessment Record: State of Connecticut Department of EducationChettamilsNo ratings yet
- Global Health Employee Application Form (Underwritten)Document4 pagesGlobal Health Employee Application Form (Underwritten)rudolfh1309No ratings yet
- Occupational Health Pre-Employment Health Assessment Form March 08Document4 pagesOccupational Health Pre-Employment Health Assessment Form March 08queenmombi100% (2)
- Health Declaration FormDocument1 pageHealth Declaration Formhasminkjk97No ratings yet
- SA04 Medical Examination Report PDFDocument4 pagesSA04 Medical Examination Report PDFSOU FEI Ang0% (1)
- Medical Conditions Declaration Form1Document1 pageMedical Conditions Declaration Form1Khôi Mạc NguyênNo ratings yet
- Interviewer: Wyeth Earl P. Endriano Clinical Group: E Clinical Instructor: Socorro Salvacion-Gasco, D.M, H.R.M, M.N, RNDocument10 pagesInterviewer: Wyeth Earl P. Endriano Clinical Group: E Clinical Instructor: Socorro Salvacion-Gasco, D.M, H.R.M, M.N, RNWyeth Earl Padar EndrianoNo ratings yet
- Health Questionnaire: Private & ConfidentialDocument3 pagesHealth Questionnaire: Private & Confidentialjames pownallNo ratings yet
- PARQDocument1 pagePARQLabbao John PaulNo ratings yet
- Physician S Report FormDocument4 pagesPhysician S Report FormpaolaNo ratings yet
- Heathrow Medicals Cabin Crew Medical and ConsentDocument3 pagesHeathrow Medicals Cabin Crew Medical and ConsentSplash1No ratings yet
- Health Questionnaire Copy1Document2 pagesHealth Questionnaire Copy1dcNo ratings yet
- Par QDocument2 pagesPar Qaicel sagaNo ratings yet
- Envelope - Medical Application Form - New - V3 - Mednet - 1Document3 pagesEnvelope - Medical Application Form - New - V3 - Mednet - 1muhdm7771No ratings yet
- Mom AssessmentDocument13 pagesMom Assessmentapi-508446364No ratings yet
- New Employee Medical QuestionnaireDocument2 pagesNew Employee Medical QuestionnaireRichard R M ThodéNo ratings yet
- Maryland Occ1215Document3 pagesMaryland Occ1215why2kliuNo ratings yet
- Head To Toe Assessment ChecklistDocument4 pagesHead To Toe Assessment ChecklistDhan IvanNo ratings yet
- OB/GYN Care Visit: Personal InformationDocument7 pagesOB/GYN Care Visit: Personal InformationsinarNo ratings yet
- Session 3 Registration PacketDocument4 pagesSession 3 Registration PacketASYMCA YCONo ratings yet
- 8. Эрүүл Мэндийн БичигDocument3 pages8. Эрүүл Мэндийн БичигOtgonbayar BattogtokhNo ratings yet
- Flu Consent FormDocument2 pagesFlu Consent FormTiger Palm TigerNo ratings yet
- Health CertificateDocument3 pagesHealth CertificateĐĂNG TRỊNH HẢINo ratings yet
- NEW PE FORM Bangayan Vhynee SDocument4 pagesNEW PE FORM Bangayan Vhynee SVhynee BangayanNo ratings yet
- Physical Activity Readiness Questionnaire (PAR-Q) : Aecoronel2101qc@student - Fatima.edu - PHDocument2 pagesPhysical Activity Readiness Questionnaire (PAR-Q) : Aecoronel2101qc@student - Fatima.edu - PHMikhaela CoronelNo ratings yet
- Year 9 Camp Health and Medical ConsentDocument3 pagesYear 9 Camp Health and Medical ConsentFiona CharringtonNo ratings yet
- COVID - Screening - Student - Child Care - Jan6 - AODA - 0Document5 pagesCOVID - Screening - Student - Child Care - Jan6 - AODA - 0KimDoll BNo ratings yet
- Registration Forms Session 4Document4 pagesRegistration Forms Session 4ASYMCA YCONo ratings yet
- Part 1 (To Be Completed by A Parent or Legal Guardian)Document1 pagePart 1 (To Be Completed by A Parent or Legal Guardian)Akshara PabbarajuNo ratings yet
- Medical Application Form (New) - V3-2021!10!12 - RAKDocument3 pagesMedical Application Form (New) - V3-2021!10!12 - RAKAnkita NiravNo ratings yet
- Pre Exercise Screening FormDocument3 pagesPre Exercise Screening FormYunonNo ratings yet
- Edical Tatement: Have You Ever Had or Do You Currently HaveDocument1 pageEdical Tatement: Have You Ever Had or Do You Currently HaveGeorge Vladut PintilieNo ratings yet
- Antenatal Booking ProformaDocument10 pagesAntenatal Booking ProformaracaneteNo ratings yet
- Student Medical RecordDocument3 pagesStudent Medical Recordhamsa RasbiehNo ratings yet
- Case 25 - USMLE 2 CSDocument5 pagesCase 25 - USMLE 2 CSJonadab SilvaNo ratings yet
- Health HistoryDocument1 pageHealth Historymolly_hayes_24No ratings yet
- Raising Children With Chronic Illness: A Mother's JourneyFrom EverandRaising Children With Chronic Illness: A Mother's JourneyNo ratings yet
- Field-Based Health-Related Physical Fitness Tests in Children and Adolescents: A Systematic ReviewDocument10 pagesField-Based Health-Related Physical Fitness Tests in Children and Adolescents: A Systematic ReviewAyamKalkun BandungNo ratings yet
- Nutrition and Sport. New Conceptual Approaches Today: Nutrición y Deporte. Nuevos Enfoques Conceptuales en La ActualidadDocument3 pagesNutrition and Sport. New Conceptual Approaches Today: Nutrición y Deporte. Nuevos Enfoques Conceptuales en La ActualidadAyamKalkun BandungNo ratings yet
- ASAQ The Reliability PaperDocument5 pagesASAQ The Reliability PaperAyamKalkun BandungNo ratings yet
- Place Essay - What Are The Health Challenges An Esport Player Faces and How Can They Be Addressed by Stakeholders?Document8 pagesPlace Essay - What Are The Health Challenges An Esport Player Faces and How Can They Be Addressed by Stakeholders?AyamKalkun BandungNo ratings yet
- Republic Act 9710 - BookletDocument131 pagesRepublic Act 9710 - BookletpcwlibraryNo ratings yet
- Yojana - July - 2022 - On TribalsDocument41 pagesYojana - July - 2022 - On TribalsNAMANNo ratings yet
- Clinical Veterinary Advisor Dogs and Cats by Etienne Cote DVMDACVIMCardiology and Small Animal Internal Medicine - 5 Star ReviewDocument2 pagesClinical Veterinary Advisor Dogs and Cats by Etienne Cote DVMDACVIMCardiology and Small Animal Internal Medicine - 5 Star ReviewMirsad Gilic0% (1)
- Burn and Reconstructive Centers of Colorado at Swedish Medical Center Raises Burn AwarenessDocument3 pagesBurn and Reconstructive Centers of Colorado at Swedish Medical Center Raises Burn AwarenessPR.comNo ratings yet
- Amoebiasis and Its Control PDFDocument11 pagesAmoebiasis and Its Control PDFLams AnkingNo ratings yet
- RENAL DISEASES Lab Act No. 22Document32 pagesRENAL DISEASES Lab Act No. 22KimberlyjoycsolomonNo ratings yet
- FDA Administrative Order No. 2020-0010 Regulations On The Conduct of Clinical Trials For Investigational Products Clinical Trial/ Clinical StudyDocument14 pagesFDA Administrative Order No. 2020-0010 Regulations On The Conduct of Clinical Trials For Investigational Products Clinical Trial/ Clinical StudyFrietzyl Mae GeneralaoNo ratings yet
- Forensic NursingDocument50 pagesForensic NursingSurya Mohan JhaNo ratings yet
- Baza Date Test Excel - Varianta 2019 FADocument654 pagesBaza Date Test Excel - Varianta 2019 FAMierlea Alexandru-Nicolae100% (1)
- Shikimic Acid Might Interrupt Spike Protein Functionality - Peak ProsperityDocument6 pagesShikimic Acid Might Interrupt Spike Protein Functionality - Peak ProsperityMas ThulanNo ratings yet
- MODULE 7 - CAPABILITY AND CAPACITY BUILDING IN DISASTER PREPAREDNESSDocument7 pagesMODULE 7 - CAPABILITY AND CAPACITY BUILDING IN DISASTER PREPAREDNESSKaguraNo ratings yet
- 12 Adverse Effects of The Ketogenic DietDocument2 pages12 Adverse Effects of The Ketogenic DietAhmed AmerNo ratings yet
- Abstracts of The 18th Congress of The European Geriatric Medicine SocietyDocument439 pagesAbstracts of The 18th Congress of The European Geriatric Medicine SocietyCristina Fernández DíazNo ratings yet
- COPD AsthmaDocument16 pagesCOPD Asthma09172216507No ratings yet
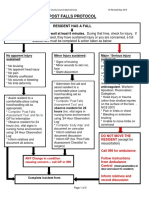
- 4-Hampshire Falls ProtocolDocument5 pages4-Hampshire Falls ProtocolsheenaNo ratings yet
- Module 6Document26 pagesModule 6xtnreyesNo ratings yet
- Jin Dan Syaitan: Sebab Penyakit Rohani Dan Jasmani: Jinn and Shay Ān: Causes of Spiritual and Physical IllnessDocument17 pagesJin Dan Syaitan: Sebab Penyakit Rohani Dan Jasmani: Jinn and Shay Ān: Causes of Spiritual and Physical IllnessAbu Musaddad KalamNo ratings yet
- Drug StudyDocument4 pagesDrug StudyKaloy KamaoNo ratings yet
- Pharmacy Bulletin Aug11Document6 pagesPharmacy Bulletin Aug11Rema Panickar SugunanNo ratings yet
- Topics For Skills Laboratory N - 104 Community Health Nursing 1Document2 pagesTopics For Skills Laboratory N - 104 Community Health Nursing 1Bem PladeroNo ratings yet
- Hypothesis-Oriented Algorithm For CliniciansDocument6 pagesHypothesis-Oriented Algorithm For CliniciansGirijashankar KhuntiaNo ratings yet
- Death Obituary Cause of Death CMFLD PDFDocument4 pagesDeath Obituary Cause of Death CMFLD PDFMayerRhodes8No ratings yet
- Labor ExerciseDocument2 pagesLabor ExerciseDon RaulNo ratings yet
- HIV / AIDS: Social and Ethical Issues: EditorialDocument2 pagesHIV / AIDS: Social and Ethical Issues: EditorialventyNo ratings yet
- Executive Order 202-202.67 (October 5)Document143 pagesExecutive Order 202-202.67 (October 5)OANo ratings yet